Article Text

Abstract
Objective To evaluate the current provision and outcome of community-based education (CBE) in UK medical schools.
Design and data sources An online survey of UK medical school websites and course prospectuses and a systematic review of articles from PubMed and Web of Science were conducted. Articles in the systematic review were assessed using Rossi, Lipsey and Freeman's approach to programme evaluation.
Study selection Publications from November 1998 to 2013 containing information related to community teaching in undergraduate medical courses were included.
Results Out of the 32 undergraduate UK medical schools, one was excluded due to the lack of course specifications available online. Analysis of the remaining 31 medical schools showed that a variety of CBE models are utilised in medical schools across the UK. Twenty-eight medical schools (90.3%) provide CBE in some form by the end of the first year of undergraduate training, and 29 medical schools (93.5%) by the end of the second year. From the 1378 references identified, 29 papers met the inclusion criteria for assessment. It was found that CBE mostly provided advantages to students as well as other participants, including GP tutors and patients. However, there were a few concerns regarding the lack of GP tutors’ knowledge in specialty areas, the negative impact that CBE may have on the delivery of health service in education settings and the cost of CBE.
Conclusions Despite the wide variations in implementation, community teaching was found to be mostly beneficial. To ensure the relevance of CBE for ‘Tomorrow's Doctors’, a national framework should be established, and solutions sought to reduce the impact of the challenges within CBE.
Strengths and limitations of this study This is the first study to review how community-based education is currently provided throughout Medical Schools in the UK. The use of Rossi, Lipsey and Freeman's method of programme evaluation means that the literature was analysed in a consistent and comprehensive way. However, a weakness is that data from the online survey was obtained from online medical school prospectuses. This means the data may be incomplete or out of date. Data in the literature review may also be skewed by publication bias.
- EDUCATION & TRAINING (see Medical Education & Training)
- MEDICAL EDUCATION & TRAINING
- PRIMARY CARE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
The context of healthcare in the UK is changing, with an increasingly aging population and a growing focus on the prevention and management of disease.1 This has prompted the need to ensure that medical graduates are adequately prepared to address these evolving healthcare needs, rather than maintaining a reactive approach to illness in the UK. These needs include the prevention and management of chronic health conditions such as diabetes, heart disease, cancer and other long-term illnesses. The promotion of health as well as the delivery of care of conditions like these often occurs within the community, outside the context of University teaching hospitals, provided by professionals from several disciplines, including a significant input from social services. In the recently published UK government's white paper, Equity and Excellence: Liberating the National Health Service (NHS),2 a need for a healthcare system focused on personalised care reflecting individuals’ health and care needs was outlined. This would involve supporting carers and encouraging multidisciplinary care. These social demographic and political drivers require strong input from multiprofessional healthcare providers in primary care and the recruitment of more general practitioners (GPs) in order to fulfil the growing need for community-based care.
This concept also resonates globally and is considered important by health regulatory bodies that license medical schools. In 1987, the WHO recommended the reform of health professional curricula by incorporating methods to prepare students for providing care at all levels of healthcare settings,3 which can be achieved by, among other things, aligning education with community needs. The UK General Medical Council's (GMC's) document ‘Tomorrow's Doctors’ recommend that clinical placements should reflect the changing patterns of healthcare and that they must provide experience in a variety of environments including hospitals, general practices and community medical services.4
Curricula in the UK medical schools, therefore, currently offer community-based education (CBE) in various forms and models of teaching.5 CBE is defined as a medical education programme that may employ any variety of teaching methods to promote an understanding of health concerns at a community level. The programme is set within the community, and involves individuals within the community.
Previous publications have evaluated these models of medical teaching in the community, including analyses of their advantages and drawbacks.6–28 However, a thorough literature search (as conducted in November 2013) found no existing systematic reviews on community-based teaching across all existing UK medical schools. It remains unclear what the extent of community-based teaching in UK medical schools is, the impact this had made to the standards of healthcare, and how the effectiveness of community-based teaching programmes has been measured. Knowledge of this is considered important, as it would guide the structuring of undergraduate medical curricula to adapt to changing contexts in the UK, hence effectively developing a future generation of doctors who are appropriately prepared for upcoming healthcare needs. The aim of this study, therefore, was to conduct an online survey of the current provision of community-based teaching within UK undergraduate medical schools to appreciate the extent of implementation. A systemic review was also conducted to comprehensively evaluate community-based teaching in UK medical curricula on the domains of programme needs, implementation, impact, and cost.
Methods
Online survey
An online survey of the current provision of community-based teaching in UK medical curricula was completed by NC through accessing official online material of medical schools between 31 November 2013 and 8 December 2013. An up-to-date list of all the registered medical schools was obtained from the Medical Schools Council (MSC) website on 31 November 2013.29 All graduate-entry courses were excluded. This was due to the wide variations of graduate-entry course structure, as well as the lack of literature on postgraduate community-based medical education. This was a prerequisite in order for the results of both the online survey and systematic review to be evaluated in parallel.
Online material of the undergraduate medical curriculum was sourced using the Google search engine, and included content from university websites or online course prospectuses for the 2014 intake. The information search was specific to descriptions of both mandatory and elective components of the curriculum relating to ‘primary care’, ‘general practice’, or ‘community medicine’.
Systematic review: data sources
A systematic literature review was conducted using the electronic databases PubMed and Web of Science to source for papers published on undergraduate community-based medical education. With the understanding that community-based education has evolved over the years, only publications published within the past 15 years, from November 1998 to 2013, were included in this study. The search criteria was (‘community-based’, ‘community-oriented’, ‘community involvement’, or; ‘primary health care’) and (‘medical curriculum’, ‘medical students’, ‘undergraduate medical education’ or ‘undergraduate medical school’).
Systematic review: selection criteria and data extraction
The relevance of the articles was screened by the title and abstract, based on the inclusion and exclusion criteria. Articles were selected if they described undergraduate medical education within the UK. Papers that included healthcare professionals apart from medical students were excluded. Any articles that were duplicated, not available in full text, or not published in English were also regarded as unsuitable for the review. In total, 29 peer-reviewed articles were identified as relevant, and were selected for further qualitative content analysis by SL and NT (see figure 1). Data on the following were extracted from each article: (1) Format of CBE; (2) Type of evaluation used to assess the programme; (3) Findings of this evaluation; and (4) Method of data collection. Rossi, Lipsey and Freeman's (2004) approach to programme evaluation was adopted to systematically categorise the evaluation findings on CBE (see table 1). The domains applicable to this study were the needs assessment, implementation assessment, impact assessment and cost assessment. The impact assessment was further subcategorised into the impact on students (target population of CBE), and the impact on others involved in CBE programmes.
Domains in Rossi, Lipsey and Freeman's approach to programme evaluation

Flow chart of search strategy used in systematic review.
Abstraction of data was performed independently by reviewers SL and NT. Themes were also independently drawn from data analysis of the impact assessments on students. Disagreements between the two reviewers were resolved by arriving at a consensus.
Results
Current provision of community-based teaching in UK medical schools
We were able to obtain information from the medical school websites about the provision of community-based teaching in all 32 undergraduate medical schools, and this is outlined in table 2 and summarised in table 3. All undergraduate medical schools provided some form of community-based teaching or placement. There was, however, variation in the structure, duration and time in the course when community teaching was delivered (see tables 2 and 3). CBE mainly took the form of clinical placements, patient studies and optional modules. The duration of community-based teaching or placements varied from half day visits to various community settings (as undertaken in schools such as Hull York, Newcastle, Nottingham and St George's) to a year-long module on primary care and population medicine (as undertaken in Brighton & Sussex). Analysis of the varying formats of CBE (with the exclusion of Norwich, due to the lack of year-by-year curriculum details) revealed that most medical schools (a total of 31) provide early exposure to general practice or community teaching. Twenty-eight medical schools (90.3%) provide community teaching from the first year of undergraduate medical education. By the end of the second year of preclinical education, students of 29 medical schools (93.5%) would have received some form of community-based teaching.
An outline of community-based teaching in undergraduate medical courses within the UK
Summary of findings from online survey
The most popular form of community-based teaching within medical schools was general practice placements with 83.9% (26 schools from a total of 31) providing general practice placements within the first 2 years of study. Patient studies were the least common form of placements. These were defined as projects where students visited patients within the community or at home. Only 38.7% (12 schools) provided this format of community education at some point in their courses.
Fourteen (45.2%) medical schools provided regular exposure to community teaching in every year or phase of the course.
With regards to optional modules offered to students, only three of the medical schools offered them—9.7%. This implies that, if students are particularly interested in community care, they may find it difficult to achieve extra studies in this area.
Literature review of studies evaluating community-based teaching
A summary of the studies evaluated in the systematic literature review are outlined in table 4. The main methods of evaluation employed in the studies were questionnaires, interviews and focus groups of the key stakeholders in CBE—students, patients, tutors and other staff in the community setting.
Summary of systematic review
Needs assessment of CBE
Studies of student expectations of CBE highlighted that students valued experiential patient-centred learning and tutor supervision in the community setting.14 ,30 In a Sheffield study,14 students also recognised that CBE was a powerful vehicle for changing their approach to medicine and illness, where the patient as a person is given emphasis over the disease.
Implementation assessment of CBE
All forms of community-based teaching were generally well-received by medical students, patients and participating healthcare professionals, supporting the continuation of existing community-based teaching programmes in the future. This included community-based teaching which was incorporated into specialty modules such as Obstetrics and Gynaecology,31 Psychiatry22 and Surgery.27 The unique approach of incorporating primary healthcare in an intercalated Bachelor of Science medical research year also received positive feedback.23
Three studies found that students preferred the implementation of practice-based teaching over hospital-based teaching. Hastings et al11 found that students in Leicester preferred practice-based teaching on the grounds of both teaching method and content. O'Sullivan et al12 had similar findings among students from University College London, where practice-based teaching bore qualities of better teaching attitudes, teaching methods and course organisation. Interestingly, these findings were consistent with Powell and Easton's27 investigation on Imperial College students undertaking their surgery module. These students preferred surgical teaching within general practices due to the learner-centred approach in teaching, more protected teaching time and regular access to suitable patients for acquiring clinical skills.
The success of community teaching in Leicester was analysed by Hastings et al.11 It was found that the improved quality of teaching by GP tutors was attributed to a higher proportion of GP tutors attending teacher-training courses. General practices were also found to have greater resource availability and NHS funding specifically allocated to support the teaching of medical undergraduates. All these factors placed hospital doctors at a disadvantage in preparing good-quality clinical teaching sessions in comparison to GPs.
Impact assessment of CBE
Studies of CBE impact on students bore the following themes: (1) Learning outcomes, (2) Behavioural changes to primary care and (3) Traits of future doctors. These are summarised in figure 2.
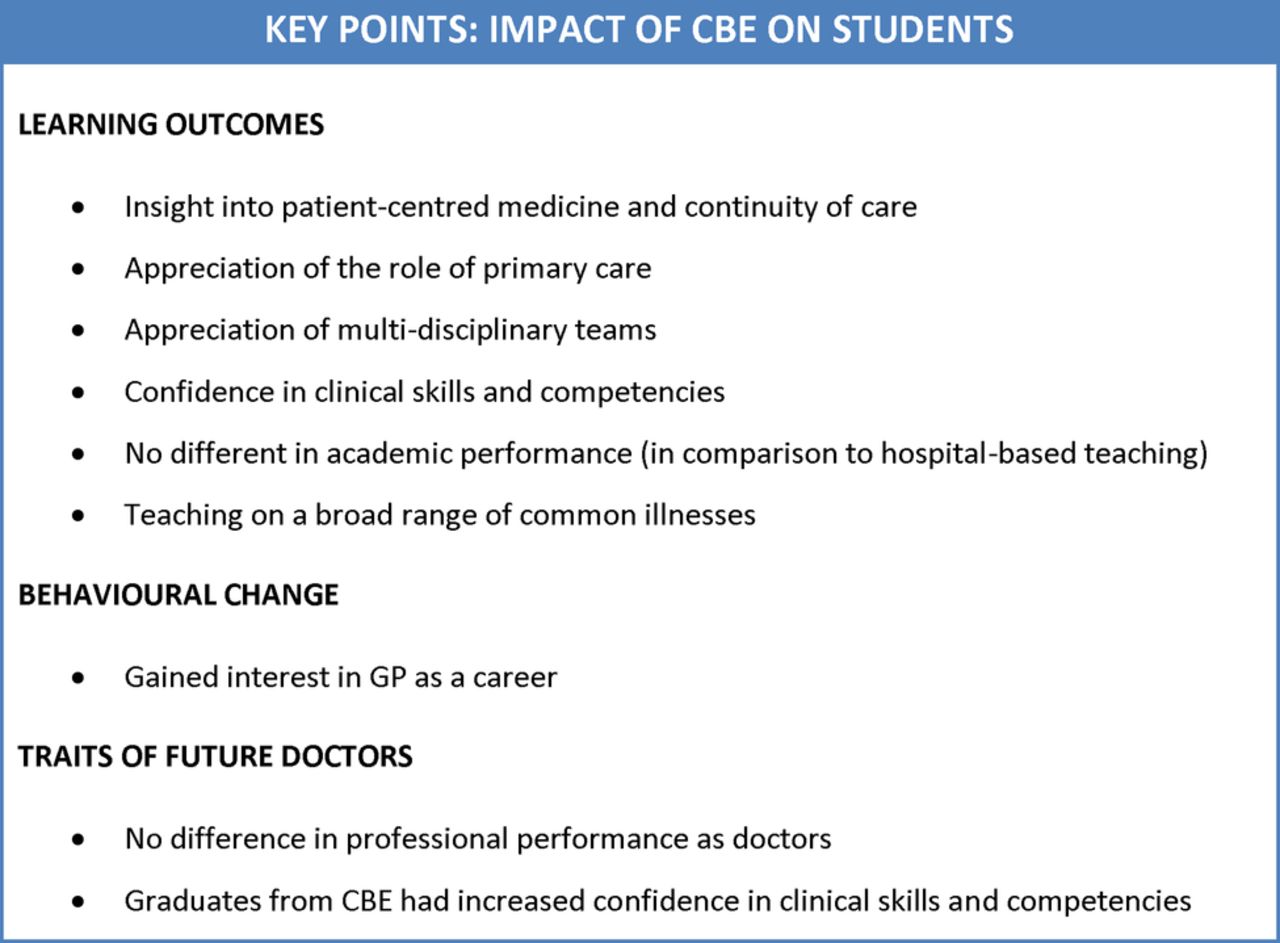
Key points: impact of community-based education on students.
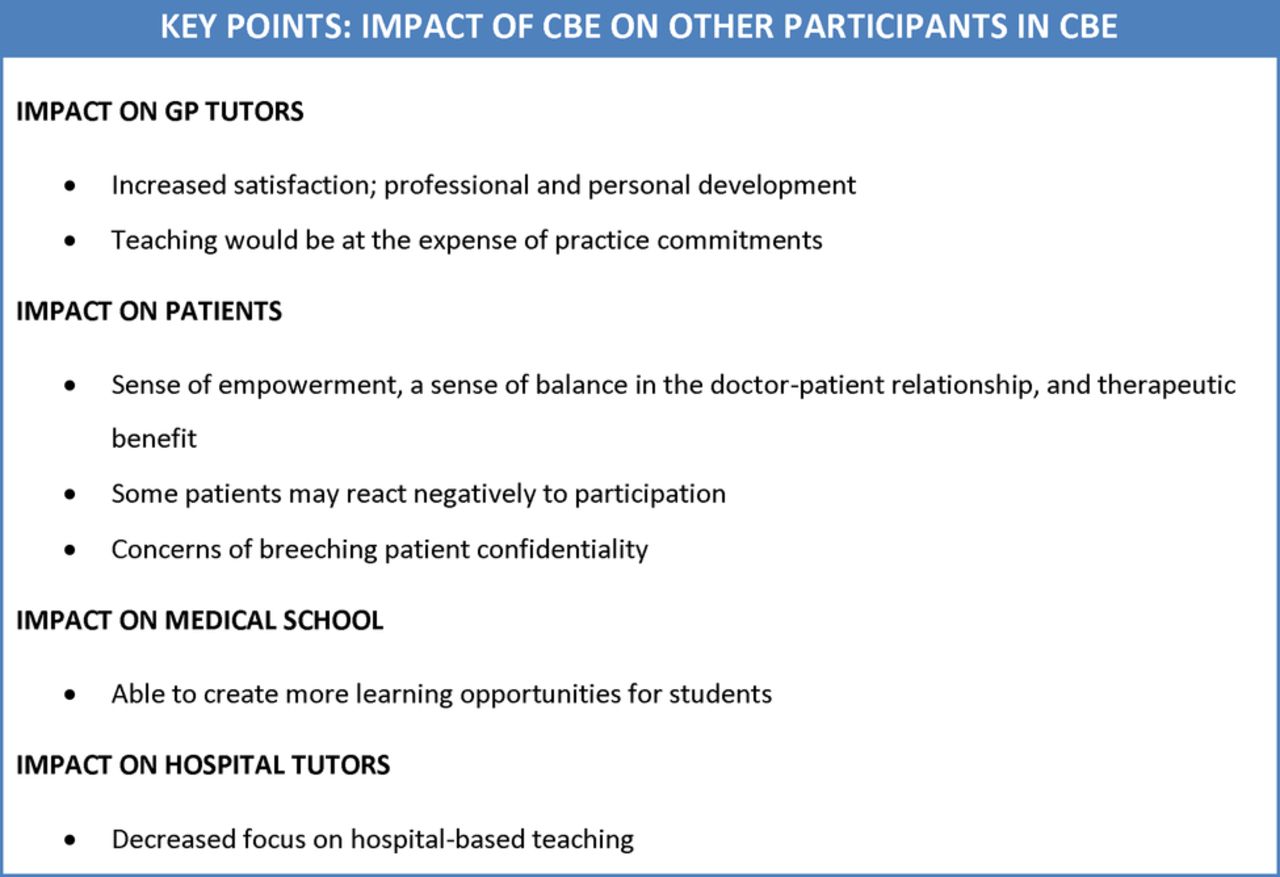
CBE also had an impact on participating doctors, staff, patients and medical schools. A summary of this is shown in figure 3.
{kind=link}
{kind=link}
{kind=link}
Key points: impact of community-based education (CBE) on other participants in CBE.
Impact on students: learning outcomes
Implementation of CBE in medical schools had a significant positive impact on medical students’ learning outcomes. The following results provide evidence of the strong educational value among students: 11 studies showed that medical students gained insight into patient-centred medicine and continuity of care, which were learning outcomes that students viewed as important in their education.10 ,13 ,17 ,19–21 ,23 ,25 ,26 ,28 ,32 This was measured quantitatively through questionnaires that were administered to students, supplemented by quantitative feedback gathered from focus groups and interviews.
Students’ appreciation and understanding of the role of primary care was found in four studies.20 ,21 ,28 ,32 This was revealed through questionnaires, where students rated the extent of their understanding of primary care and its relationship with other levels of care. Two studies reported the benefit of community placements in broadening the student's awareness of teamwork in multidisciplinary teams.19 ,30 Another study reported the positive finding of successfully exposing students to a broad and varied range of clinical problems in a community setting.33
In comparison to hospital-based teaching, improved confidence in clinical skills and competencies was found to be a favourable outcome of CBE in four studies.10 ,12 ,19 ,20 This finding was derived from questionnaires and focus group interviews from students who had experienced CBE.
Two studies found no difference in academic performance between students under CBE and ‘traditional’ hospital-based teaching.17 ,20 One study of students who undertook a specialty placement in Obstetrics and Gynaecology also found that there was no difference in clinical performance as rated by their tutors, and no statistically significant difference in student final clerkship grades.34
Although most evaluations produced consistent evidence on the benefits of community teaching, two studies highlighted the lack of in-depth knowledge of specialist teaching when conducted by GP tutors: the significance of this finding was measured qualitatively through student interviews,27 and quantitatively through academic scores for the respective specialty modules.34
Impact on students: behavioural changes to primary care
Two studies found that the implementation of CBE resulted in a reversal of negative attitudes towards primary care, and an increase of interest in general practice as a career option among students.23 ,32
Impact on students: traits of future doctors
Studies also showed that medical graduates from curricula with increased emphasis on community-based teaching were at no disadvantage to graduates from the traditional hospital-based teaching.17 ,33 Academically, graduates from a community-based curriculum performed as well as their counterparts on their final formative assessments. Moreover, graduates from curricula where community-based teaching had been offered had the advantage of increased confidence in communication skills and clinical skill competencies. This outcome of CBE was evaluated in three studies.17 ,20 ,28 Two of these three studies additionally reported that graduates felt less confident in their medical knowledge on disease processes.20 ,28 However, there was no evident difference found in comparison to graduates of ‘traditional’ programmes of old medical curricula which had no CBE component when measured by academic results and feedback from educational supervisors.20 ,28
Impact on others involved in CBE orogrammes
In three studies, it was found that GP tutors and participating staff had both role satisfaction and development of professional and personal ethics.7 ,13 ,24 Grant and Robling24 also found strengthened team ethics between members of the primary healthcare team.
Doctors and staff, however, were found to have organisational issues in juggling community teaching with practice commitments. The expense of one over the other was described in CBE implemented by the University of Birmingham.7 The unfavourable outcome of blurred boundaries in the doctor–patient relationship was also reported as a concern in two studies.18 ,22
Five studies evaluated the positive patient outcomes of CBE: Four of these studies reported the beneficial sense of empowerment that patients gained from participating in community teaching.9 ,21 ,22 ,24 The remaining study reported that patients developed feelings of altruism from helping medical students in their education.18
Apart from gaining a sense of empowerment, Walters et al22 also reported the development of a more balanced doctor–patient relationship, and a therapeutic benefit for the patients as a result of talking to students about their medical condition.
Among these five studies on patient outcomes, two studies included further evaluations on the negative impact that resulted from patient participation. The negative outcomes comprised, reinforced feelings of ill-health which may be distressing or anxiety-provoking and concerns of breaching patient confidentiality.18 ,22
Powel et al's 27 evaluation also shed light on the benefits that medical schools gained from tapping into teaching within the community. By doing so, medical schools were able to increase the availability of learning opportunities to medical students.
Two studies raised the possibility of the negative impact that CBE would have on hospital tutors.7 ,13 The concern raised in these studies was with regards to a shift of focus away from teaching conducted by hospital-based tutors, and towards an emphasis on teaching in the community.
Cost assessment of CBE
Only one study evaluated the costs of running a community-based course. An evaluation of CBE in Cambridge revealed that the programme was cost-feasible as the total expenditure on one student-year of community-based teaching was within the cost estimates of Service Increment for Teaching (SIFT) funding.17 The study also noted that the balance between placement costs and facilities costs stood at a ratio of approximately 2:1, which is a reverse of the traditionally allocated 1:4 ratio in SIFT funds. This finding implied that the traditional allocations for SIFT funds would be inappropriate when applied to community-based teaching.
Discussion
This study was conducted to analyse the current provision of community-based education across undergraduate medical schools in the UK. All medical schools were found to offer some community-based teaching in their curricula, which falls in line with the recommendations of the WHO and the GMC which also follows the social demographic and political changes within the UK. Furthermore, a significant proportion of medical schools offered community-based teaching early in the medical course. The benefits of this early exposure is explored by Dornan et al,35 ,36 where the opportunity to learn in context of clinical settings enabled students to develop an awareness of their interpersonal skills, attitudes and abilities.
In general, community-based teaching was well-received by medical students due to its good educational value on many levels of learning outcomes. It also gave students insight into the option of general practice as a future career. This is consistent with the direction of travel the UK healthcare workforce needs to address due to the changing demographics and the emphasis changing in healthcare delivery from management to prevention. Not only was community-based teaching of value to students, but it was also found to produce medical graduates of equal clinical skills and competencies to their counterparts who were taught under the ‘traditional’ hospital-based medical programme.17 ,33 This outcome is consistent with findings in Australian medical schools which showed that students generally did as well as or, in some areas of clinical competencies, even better than their counterparts who received hospital-based teaching.7 Community-based teaching in medicine was also beneficial to medical schools in maximising the sources of available learning opportunities for medical students.27 Moreover, community-based teaching in medicine was found to offer a unique opportunity to foster inter-professional learning—an outcome that is consistent with the political drivers for better patient care.37
Although it was evident that community-based teaching has a vast array of benefits, several drawbacks were identified and underscored as challenges to the implementation of CBE. Studies reflected the challenges of general practice tutors lacking adequate knowledge in specialty areas,27 and community teaching having a negative impact on the delivery of health service in some general practices.7 Murray and Modell38 discuss possible solutions to these issues, such as the development of university-linked practices that would scrutinise the effectiveness of teaching. It is imperative that these solutions are explored and tested in current CBE programmes so that the impact of programme drawbacks may be reduced. This would be the way-forward to strengthening the implementation of CBE in medical curricula.
An assortment of models were seen to be used for community-based teaching in the UK, where programmes varied in their methods of delivery, durations of exposure and points of undergraduate education at which the teaching was delivered. This is congruous with guidance from the GMC publication ‘Tomorrow's Doctors’, which states that it was for each medical school to design its own curriculum to suit its own circumstance. It should be noted that community-based education broadly encompasses varied delivery formats, including both clinical and non-clinical experiences. Unfortunately, the diversification of CBE poses a challenge for developing a standardised set of criteria for evaluating the outcomes of CBE. Consequently, it becomes difficult to establish a national framework for quality assurance of medical curricula, and to make recommendations for improving the implementation of CBE.
In order to achieve the expectations laid out for ‘Tomorrow's Doctors’,4 there is a principal need to define the competencies that are required to prevent illness and promote health in the primary care or community-based setting. Ladhani et al,38 for example, categorised six themes of community-based education competencies within nursing and medicine: public health; cultural diversity; leadership and management; community development and advocacy; research and evidence-based practice; and generic competencies. Subsequently, a national framework may be derived from these key competencies so as to measure the effectiveness of community-based teaching in achieving these targeted goals.
The development of a national framework was explored and suggested by Cotton et al,39 where a list of criteria for quality practice-based teaching in the UK was consensually derived from views of medical educators and students at a national conference. However, since its development, there has been no literature found on the use of these criteria to objectively evaluate community-based education at a local, regional or national level. More work in this area should be encouraged to achieve a national standard for community-based education in the UK.
Little data was found on the cost implications of community-based teaching. Given the wide variations in the format of CBE programmes conducted across the UK, it is difficult to make general conclusions about the cost impact of community-based teaching. Nonetheless the findings from Oswald et al's17 study sets a benchmark for other similar community teaching within the UK. Oswald et al found that the absolute costs per student session of community teaching was within the budgets of SIFT funding. The cost-feasibility implied in this study is consistent with Murray et al's40 1993 study of the University College London teaching programme, where community teaching cost £60 per student session, comparing well with the SIFT provision of £64 per student session. However, Oswald et al discusses that the national formula for SIFT funds is inappropriate for community teaching due to a mismatch in the 2:1 ratio of placement costs and facilities costs in community teaching, versus the traditionally allotted 1:4 SIFT ratio between placement costs and facilities costs. SIFT funding to medical education institutions is traditionally divided to cater for the costs of clinical placements (about 20%) and the costs of facilities (80%). The 1995 Winyard Report specified that the use of SIFT funding would support teaching conducted in settings other than the main university hospital, such as in general practices and community settings.41 This report unfortunately failed to realise the inappropriateness of applying the 1:4 formula (for facilities and placement costs) in the context of primary care. The allocation of 80% SIFT funding to facilities would be disadvantageous to community-based teaching since this money will be retained for usage within the hospital setting. It is important that the provision of SIFT funding is reconsidered so that it suits a growing emphasis of community-based education in the medical curriculum and therefore help develop these settings as centres of education.
The strengths of our study are that it provides the most up-to-date picture of the UK landscape of community-based teaching in medical schools' and the fact that the literature review was conducted in a systematic way. The use of Rossi, Lipsey and Freeman's widely accepted approach to programme evaluation also ensured that programme evaluations in the literature were analysed comprehensively.
The weaknesses of the online survey are that it relied on data provided on the websites of medical schools which can occasionally be out of date and incomplete. The online survey also had the disadvantage of inconsistency in the extent of details provided online. For example, the online sources may not have mentioned details on clinical placements which are primarily hospital-based, but also provide supplementary clinical teaching within the community setting, (eg, shadowing of a community midwife in an Obstetrics and Gynaecology placement). To address these weaknesses, the method of information collection may be improved by contacting course administrators to obtain detailed and focused information on any community-based teaching that is offered to students in all the course modules. A weakness of the literature review is publication bias. The majority of the papers included in the review were written in support of CBE, and there are very few publications which focused on the disadvantages of CBE. This imbalance may have skewed our data in favour of CBE.
Conclusion
In this study, all undergraduate medical schools in the UK were found to offer some form of community-based teaching in their medical curriculum. The delivery of CBE varied broadly, but all forms of community teaching were generally found to be beneficial and was therefore well-received by students, patients, participating staff and medical schools. The challenges and cost issues of community teaching should also not be overlooked, and solutions to address these need to be explored such that the delivery of CBE may be improved.
Under the pressures of social demographics and political drivers to incorporate more community-based teaching in medical education, there is a need to ensure that CBE is delivered at acceptable quality standards for it to achieve its anticipated benefits. A national framework would need to be established to ensure these standards are met. This would then succeed to act as a standardised national guideline for evaluating the effectiveness of CBE programmes in developing professional competencies that are expected of ‘Tomorrow's Doctors'.
References
Footnotes
-
Contributors WA came up with the concept of the study. NC performed the medical school online survey. SWWL and NT performed the literature review. SWWL, NC and NT wrote the draft of the manuscript. SWWL, NC, NT and WA were involved in editing the manuscript.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.