Article Text

Abstract
Background Better understanding, documentation and evaluation of different refugee health interventions and their means of health system integration and intersectoral collaboration are needed.
Objectives Explore the barriers and facilitators to the integration of health services for refugees; the processes involved and the different stakeholders engaged in levaraging intersectoral approaches to protect refugees’ right to health on resettlement.
Design Scoping review.
Methods A search of articles from 2000 onward was done in MEDLINE, Web of Science, Global Health and PsycINFO, Embase. Two frameworks were applied in our analysis, the ‘framework for analysing integration of targeted health interventions in systems’ and ‘Health in All Policies’ framework for country action. A comprehensive description of the methods is included in our published protocol.
Results 6117 papers were identified, only 18 studies met the inclusion criteria. Facilitators in implementation included: training for providers, colocation of services, transportation services to enhance access, clear role definitions and appropriate budget allocation and financing. Barriers included: lack of a participatory approach, insufficient resources for providers, absence of financing, unclear roles and insufficient coordination of interprofessional teams; low availability and use of data, and turf wars across governance stakeholders. Successful strategies to address refugee health included: networks of service delivery combining existing public and private services; system navigators; host community engagement to reduce stigma; translation services; legislative support and alternative models of care for women and children.
Conclusion Limited evidence was found overall. Further research on intersectoral approaches is needed. Key policy insights gained from barriers and facilitators reported in available studies include: improving coordination between existing programmes; supporting colocation of services; establishing formal system navigator roles that connect relevant programmes; establishing formal translation services to improve access and establishing training and resources for providers.
- intersectoral
- right to health
- access
- refugees
- integration
- resettlement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Our study employs a systematic approach by using two frameworks, the ‘framework for analysing integration of targeted health interventions in systems’ and ‘Health in All Policies’ framework for country action to develop a stronger understanding of the processes and actors involved in integration and intersectoral action.
Our findings can be applied for policy and action aiming to enhance the integration of refugee health services within health systems, and identifying research needs to advance the right to health for refugees.
The lack of evidence on intersectoral and integrated approaches from low-income and middle-income countries may impact the generalisability of the findings.
Introduction
Upholding the right to health is a fundamental challenge for governments worldwide, particularly when providing services to vulnerable or hard to reach populations such as refugees. The Office of the United Nations High Commission for Human Rights identifies the right to health as a fundamental part of human rights, first articulated in the 1946 Constitution of WHO.1 Entitlements under the right to health include universal health coverage—now a target under Sustainable Development Goal (SDG) 3—broadly covering access to preventative and curative services, essential medicines, timely basic health services, health-related education, participation in health-related decision making at both national and community levels, as well as financial protection.1 2 Especially relevant to the plight of refugees, the right to health includes non-discrimination whereby health services, commodities and facilities must be provided to all without any discrimination. Lastly, these health services must be accessible, medically and culturally appropriate, available in adequate amount and quality, which includes having a trained health workforce, safe products and sanitation.2
‘Refugees’ are individuals fleeing armed conflict or persecution as defined by the 1951 Refugee Convention which also identifies their basic rights, specifically that refugees should not be returned to situations that are deemed a threat to their life or freedom.3 A key distinction of refugee rights is that they are a matter of national legislation, and of international law.4 Despite these legal protections, refugees face many challenges in accessing health services, especially more vulnerable groups like women and children.5 Many states explicitly exclude refugees from the level of protection afforded to their citizens, instead choosing to offer ‘essential care’ or ‘emergency healthcare’, which is differentially defined across countries.6 The Committee on the Elimination of Racial Discrimination, and the Committee on Economic, Social and Cultural Rights, both include general statements that hold States accountable to ‘the right of non-citizens to an adequate standard of physical and mental health by, inter alia, refraining from denying or limiting their access to preventive, curative and palliative health services’.7 The increasing number of refugees over the past years makes the realisation and protection of these rights both a legal, ethical and a logistical challenge.5 In addition, the boundaries of the right to health have expanded due to increased understanding of social determinants of health and the health impacts of the lived environment.8 9 Refugees face challenges in navigating health, legal, education, housing, social protection and employment services, which further threatens their quality of life and health status.10 Therefore, a lack of coordination and integration across these services undermines their effectiveness.11
Much like the shift from the more vertical approaches of the millennium development goals towards the more integrated SDGs, the protection of the right to health calls for an intersectoral approach whereby health is applied to all policies for all people.12 As such, for states to effectively protect the right to health for refugees, there is a need to work across sectors and disciplines to better integrate targeted programmes and initiatives, thereby improving standards of care during resettlement. Some evidence exists that supporting collaboration and coordination across social services for refugees improves the effectiveness and quality of care received.10 Many fragmented psychosocial programmes exist across sectors to attempt to address the unique challenges faced by refugees but these are largely unevaluated and lack sustainability.13 14 Better understanding, documentation, evaluation and reporting of the dynamic nature of different interventions, and their means of health system integration and intersectoral collaboration, are necessary to ensure that lessons learnt are implemented in the design of future policies and programmes.
Therefore, we conducted a scoping review that describes the barriers and facilitators to integrated health services for refugees; the process involved in protecting refugee health; and the different stakeholders engaged in leveraging intersectoral approaches to protect refugees’ right to health on resettlement. We focused on three specific research questions:
What are the barriers and facilitators in integrating targeted services for refugees within existing health systems?
What strategies are involved in addressing refugees’ right to health on resettlement?
Which stakeholders are involved in leveraging intersectoral approaches to protect refugees’ right to health?
Methods
Study design
We selected the scoping review method as we were interested in mapping the concepts relevant to the complex nature of this topic, the changing global landscape around it, and the emerging and diverse knowledge base, which makes the method well matched to our research objectives.15 16 We drafted a scoping review protocol following the methods outlined by the Joanna Briggs Institute Methods Manual for scoping reviews.17 Our protocol was registered with the Open Science Framework,18 and published in BMJ Open.19 Since our full methods are available in the published protocol, a summary is provided below.19
Information sources and search strategy
A search of articles was done by two experienced librarians at the Karolinska Institutet using the following electronic databases: MEDLINE, Web of Science, Global Health and PsycINFO, Embase. See online supplementary appendix I for the comprehensive search strategy. Search terms included umbrella terms for three topics: refugees (eg, immigrants, migrants, asylum seekers, transients); health and social services (eg, healthcare, patient experience, health services, interdisciplinary, intersectoral collaboration, access to care)and health equity (eg, disparities, social determinants, rights-based approaches). These were combined to comprise the search (detailed search terms in online supplementary appendix).
Supplementary file 1
Eligibility criteria
Population
Refugees as defined by the 1951 Refugee Convention.3
Intervention
A programme, approach or technical innovation that aims to protect refugees’ right to health, including interventions aimed at addressing the social determinants of health. Interventions outside of the health sector that affect health were included.
Comparators
This component was not necessary as the focus was on gauging the state of evidence.
Outcomes
Eligible studies and papers include those discussing plans for action, strategies, barriers, facilitators or outcomes using an intersectoral approach.
Types of studies included
Randomised control trials, pre–post design evaluations, qualitative evaluations and economic evaluations were included. Further, implementation research and operations research studies were eligible for inclusion, as well as studies or reports outlining stakeholder experiences and plans.
Exclusion criteria
Papers published in a language other than English were excluded. Other categories of migrants were not included as their legal entitlements are different to those of refugees which are protected under international law. If the studies did not display some level of integration nor intersectorality, they were not assessed further.20 Studies or commentaries that solely discuss theories and conceptual models were excluded.
Time period
Only studies from 2000 onward have been included.
Setting
Eligible studies are set in countries receiving refugees and asylum seekers (who may eventually qualify for refugee status) and serving as hosts for resettlement.
Frameworks to address research questions
Two published frameworks were used in our analysis to understand integration of health services within health systems and to analyse intersectoral approaches to support these services. The first framework by Atun et al,21 is a tool for analysing integration of targeted health interventions in health systems, where integration is defined as ‘the extent, pattern and rate of adoption and eventual assimilation of health interventions into each of the critical functions of a health system’.21 The framework for integration was also used to assess the process, and actors involved in integration.20
The second framework applied in our analysis is that of the Health in All Policies (HiAP) framework for country action. HiAP is defined as a way for countries to protect population health through ‘an approach to public policies across sectors that systematically takes into account the health implications of decisions, seeks synergies and avoids harmful health impacts in order to improve population health and health equity’.22 Components of this framework, adapted to refugee needs, were used in the review to frame barriers and facilitators in integrating refugee services through intersectoral collaboration.
Data abstraction
A data abstraction chart was developed based on the two frameworks used in this study. The chart was tested by two researchers and revised as appropriate. The revised chart was used by the same researchers to abstract descriptive and qualitative data as relevant to the elements of the frameworks used. Elements included in the chart were: intervention description; barriers and facilitators; contextual details; target population; type of evaluation; outcomes; stakeholder involvement in governance, financing, planning, service delivery, monitoring and evaluation, and engagement. Deductive reasoning was used to identify barriers and facilitators in intersectoral collaboration for refugee health. Open coding was applied to visualise themes across interventions as well as barriers and facilitators.23 Axial coding was applied to then draw connections to enabling strategies for intersectoral collaboration.23 General conclusions were drawn based on these themes, leading to suggestions for strengthening programmes and policies.
Patient and public involvement
There was no patient or public involvement required in conducting this scoping review.
Results
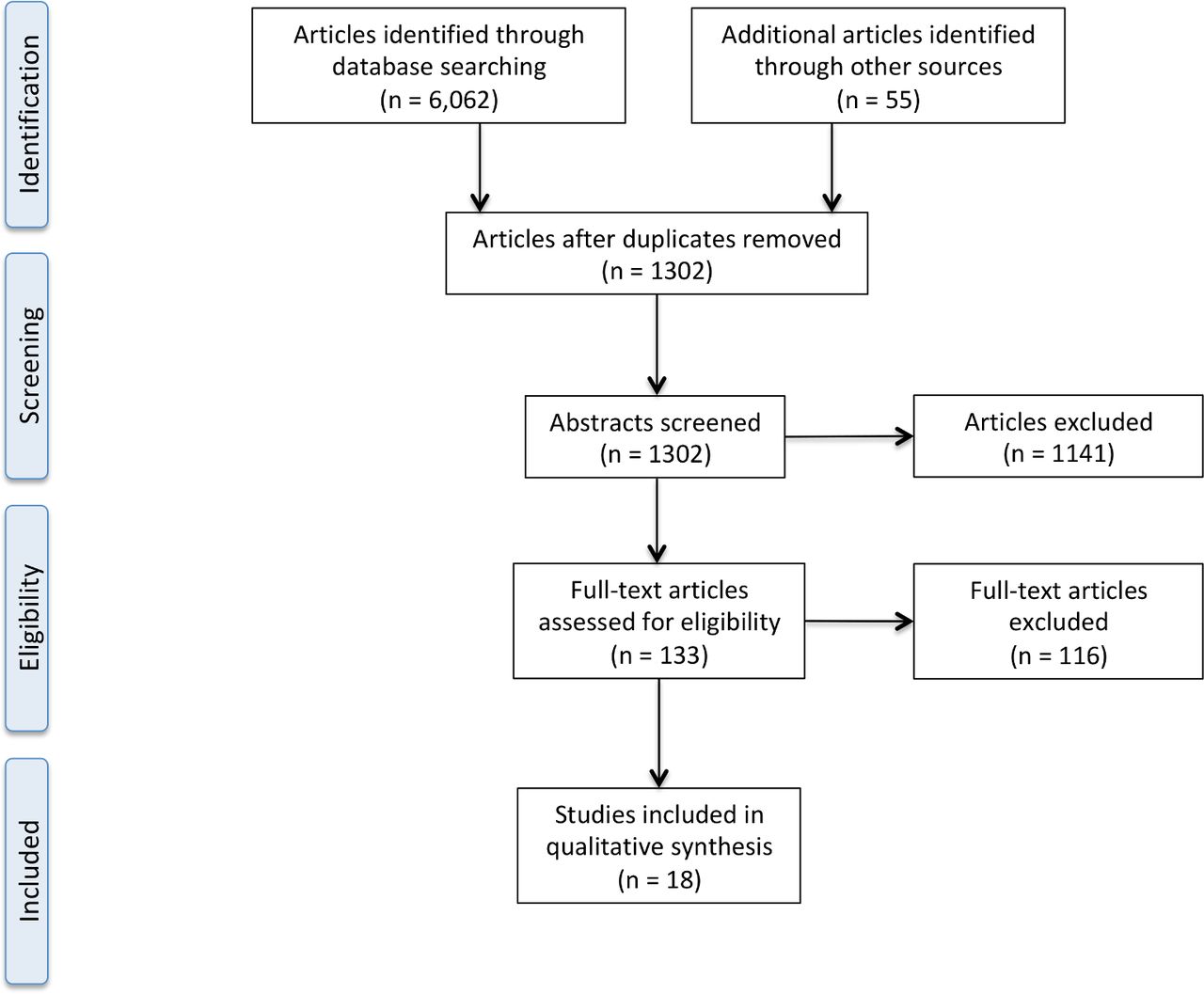
Of the 6117 records identified through the search strategy, 1302 abstracts were screened after removing duplicates. A total of 1141 were excluded based on exclusion criteria described above as assessed by two independent reviewers, 131 full texts were assessed, with the references of 15 selected articles additionally screened for inclusion criteria, a total of 18 studies were included in our review (see figure 1). Five studies were programmes or interventions carried out in the USA, one in Australia, two in Canada, one in Ethiopia and Uganda, and one in each of the following: Italy, Lebanon, Mexico, the Netherlands, New Zealand, Spain and the UK (See table 1). Six studies were interventions at the district/local level, four at a broader regional level and five at the national level. The interventions outlined in the included studies addressed mostly all genders and all age ranges with the exception of six that targeted vulnerable groups: two studies on mothers and children24 25; one on the elderly26; one on students27 and two on women and girls.28 29 Interventions targeting women and children in particular used alternative models of care such as mobile health clinics28 29 and school-based interventions.24 27 Seven studies applied qualitative approaches (primarily in-depth interviews) for evaluation,27–33 four studies used survey tools or standardised assessment tools25 26 34 35; four studies used descriptive and routine data24 36–38; and three studies were mainly descriptive analysis reporting on and looking at the outcomes of case examples and policies.39–41
Summary of included studies
{kind=link}
Scoping review flow chart.
To respond to research question 1, each of the interventions and summarised barriers and facilitators are described in table 1 and grouped by common themes in table 2. Common facilitators identified in programmes and approaches to protect refugee health through intersectoral approaches and integration of services include: strong communication of programme availability, tools and training for providers, colocation of services, transportation services to enhance access, clear role definitions, interprofessional team and relationship management across providers, appropriate allocation of budget and financing and coordinated refugee-specific policies.
Barriers and facilitators commonly discussed across studies
Barriers articulated include: lack of a participatory approach, poor communication leading to stigma and underuse of services, insufficient resources given to providers, absence of financing, unclear roles and insufficient coordination of interprofessional teams, exclusionary refugee policies, low availability and use of data and turf wars across governance stakeholders. Table 2 highlights the studies that expand on these themes as barriers or facilitators.
To respond to research question 2, this section will summarise common themes identified as enabling strategies that support intersectoral collaboration to promote refugee health. Strategies identified in this review include: establishing networks of service delivery through a combination of existing public and private services, establishing a system navigator role, engaging host communities to reduce stigma, ensuring availability of translation services, outreach, and advocacy and legislative support. Table 3 highlights the studies that address each of these strategies. In Italy, for example, networks were promoted among private and public authorities and service providers, including health, employment, vocational training and continuing education services.34 In this model, users moved through the pathways of integration and can receive support for any combination of health needs, access to education, housing support and legal assistance.34 Collaborative design and delivery of services was also demonstrated in Australia with support from multidisciplinary, intersectoral teams, but a lack of funding presented barriers to the potential success of this initiative.27 Similarly in the USA, the ‘Bridge Project’ faced insufficient funding in the coordination of care despite seeing promising results from use of a system navigator—or primary care nurse ‘bridge’—to connect primary care and mental healthcare services.37 A network of ‘gateway services’ was also tested in Canada using a ‘Reception House’ model.35 These services are characterised by being person-centred, interprofessional, communication-focused and comprehensive across the continuum of care.35 Relationship management between the Reception House, health professionals, translation services and social services was acknowledged as a key component for success.35 Input from international medical graduates in training also supported this work by enhancing culturally appropriate service delivery by this network of partners.35
Enabling strategies present across studies
Striking a balance between providing tailored, culturally appropriate care and integrating health and social services for refugees into existing services in the host community can be especially challenging. Policy reviews suggest that taking a ‘one-policy, one-level, one-outcome’ approach or focusing refugee management under one ministry is not sufficient in addressing the wide range of obstacles that both host and refugee communities are facing as a result of the current political climate.40 41 The Ethiopian government, for example, had success in reorganising ministries to incorporate refugee management into existing portfolios rather than a refugee-specific one, moving refugee assistance programmes out of camps and promoting more collaboration across government and non-governmental programmes.41
In terms of stakeholders involved (research question 3) in implementing, monitoring or facilitating the aforementioned strategies, studies did not always report on the parties involved in governance, financing, planning, service delivery, monitoring and evaluation or demand generation (elements drawn from the integration framework by Atun et al.21 Where they were mentioned, stakeholders responsible for the governance of interventions addressing refugee health were composed of primary care centres,35 37 municipal governments,30 38 departments of social services and/or public health,30 36 central services responsible for coordination of refugee services and provision of assistance to local services,34 35 national governments31 32 and international bodies.28 Stakeholders responsible for health financing consisted of individual fundraising by service providers,31 33 government30 31 35 38 41 and international bodies or donors.1 28 36 37Programme and policy planning stakeholders encompassed national governments,31 38 41 departments of social services and/or public health,27 30 36 central services responsible for coordination of refugee services and provision of assistance to local services,29 34 35 researchers,24 26 30 36 37 service providers27 28 35 37 and international bodies or donors.28 36 41 Service delivery stakeholders included national departments of social services and/or public health,27 30 33 36 38–41 networks of local service providers in health, education, socialisation, translation and/or employment,24 31 34 36 healthcare providers,27 33 35 37 38 central services responsible for coordination of refugee services and provision of assistance to local services,32 34 35 community health workers26 and international bodies.28 41 Stakeholders responsible for monitoring and evaluation were seldom explicitly mentioned. For demand generation, stakeholders included central services responsible for the coordination of refugee services and provision of assistance to local services,35 local media in the language of the target population,36 community leaders and/or community health workers,26 28 31 32 home health outreach services28 31 and healthcare providers.33 37
Discussion
The findings from the existing but scarce literature highlight critical factors necessary in facilitating intersectoral collaboration and the successful integration of refugee services within existing health systems. The three research questions studied demonstrated barriers and facilitators, enabling strategies recorded in the literature and the stakeholders involved. This section will summarise key themes across these topics and discuss implications for programme implementation, policy and future research.
Coordination of existing public and private services
A networked approach to service delivery during the initial reception of refugees can often mitigate some of the difficulties encountered by refugee communities. Some examples of coordination of services were seen in Italy,34 Australia,27 the USA37 and Canada.35 In Canada, where a network of ‘gateway services’ was tested using the ‘Reception House’ model, it successfully provided responsive and culturally sensitive primary care.35 By partnering community and translation services, as well as healthcare providers with the Reception House, it decreased wait times and improved healthcare access through referrals and coordination of services.35 Further analysis with costing studies on a tailored package of health services for vulnerable populations could help to support improved financing of efforts to coordinate services across sectors.
Introduction of a system navigator role
Integration works through establishing relationships across networks of local stakeholders and service providers. To coordinate this effectively, a system navigator role can be established—the evidence suggests that this role is most effective in the early stage of resettlement.35 The system navigation role can be played by an organisation or by people within the existing health or social systems. It connects incoming refugees to timely, culturally appropriate care in the community without creating parallel structures that either threaten host communities or further stigmatise refugees.30 35 The likelihood of success of a system navigator role is further strengthened when providers have access to the knowledge, tools and training needed to address the specific needs of refugees, including the more vulnerable subgroups (eg, the elderly, women and children). Providers need to understand the context in which they work and the available features and services, user needs, and legislation as it relates to refugees.34 Those playing a coordination or system navigation role should also be able to build strong networks with allied specialists, identify appropriate resources and reach out to users.34 35 The risk here, however, is that integrating refugee care may eliminate some determination procedures, potentially undermining the protection mandate and underestimate the tailored needs of refugees dealing with significant trauma.41 Future research on the required competencies of the system navigator role is needed to ensure that appropriate professionals are recruited and trained.
Advocacy and legislative support
Exclusionary immigration policies can play a considerable role in marginalisation and discrimination against refugee communities leading to decreased health-seeking behaviours and use of available integrated or intersectoral services.40 Effective advocacy needs to target the policy-making levels in order to counteract the negative impacts of exclusionary policies. Advocacy by healthcare providers can be influential at the institutional level to push for better allocation of services and funding.31 A multipronged approach may be necessary to continue to advocate for the right to health for refugees by addressing legal challenges, establishing timely and accurate data and information systems to capture needs, creating health promoting environments, investing in person-centred, culturally appropriate and easily accessible services, and evaluating coordination and service delivery efforts. Engaging policy-makers in knowledge translation and evidence-informed decision-making is one way to effectively advocate and provide legislative support in refugee health. In Lebanon, for example, where there are huge demands in meeting the health needs of a large Syrian refugee population, researchers engaged policy-makers in knowledge production (ie, research priority-setting), translation and uptake activities.42 This ultimately led to the hiring of a refugee health coordinator by the Lebanese Ministry of Public Health. The refugee health coordinator role functioned to support intersectoral collaboration, assisting in strategic planning and implementation of action plans to respond to the health needs of Syrian refugees including helping with the development of refugee health information systems at the Ministry of Public Health.42 The UCL-Lancet Commission on Migration and Health also supports knowledge translation by bringing together academics, policy-makers and health system experts to take an interdisciplinary approach to reviewing evidence, develop policy recommendations and disseminate these findings globally among policy-makers and institutions.43
Alternative models of care to reach vulnerable women and children
Among the studies that reported targeted interventions for women and children, alternative models of care were used. This included mobile health clinics, and programmes linked to schools to support screening and active case finding. These alternate models increased accessibility of essential health services, increased detection of health conditions and improved coordination of care, and reduced feelings of social isolation.27 28 This suggests that flexible service delivery and innovation in mode of delivery should be considered when attempting to reach at risk refugee groups. Better collection and use of evidence on the needs of vulnerable refugee subgroups and how to target them are essential next steps to design appropriate service delivery models.
Policy insights
From the available evidence, the following are policy insights to inform greater integration of services and/or intersectoral collaboration. These recommendations are based on consistent facilitators and barriers identified across studies included in this review. They are critical starting points in enhancing programmes to better serve refugees while promoting efficiency in health systems.
Strengthening the coordination between existing programmes through financing stronger referral systems and colocation of services.
Incentivising health and social service authorities to establish and finance formal system navigator roles that connect all relevant services–provision of information technology tools can help support this function and better manage the network of available programmes.
Engaging host communities to enhance understanding, reduce stigma and to create an enabling environment for policies that protect refugees and their rights to social determinants of health.
Communicating the availability of programmes and services through cultural mediators and establishing formal translation and transport services to improve access.
Establishing training and resources for providers to (A) better understand the needs of refugee communities, (B) be aware of available and relevant services for referral across sectors and (C) more efficiently manage cases.
Limitations and future directions
Our review was limited by the scarcity of evidence in this area. Due to this, all relevant studies were included, therefore, quality and rigour may vary. Some key programmes and approaches may be missing due to interventions occurring at the individual level instead of at the systems level, as well as not having been published in academic literature. Individual health providers or organisations will navigate barriers in health systems through tacit and experiential knowledge that is often not documented. Data will be further amplified by conducting key informant interviews in selected countries.
As others have noted, the literature on intersectoral collaboration disproportionately focuses on high-income countries.44 It is, therefore, no surprise that the evidence for this review largely came from high-income countries with only two studies conducted in upper-middle income and two in low-income countries. This may affect the generalisability of the findings reported here as low-income and middle-income countries have greater coordination challenges to overcome due to fragmented systems and weak governance.45 Additionally, according to the latest report from the United Nations Refugee Agency, approximately 85% of refugees are hosted in developing nations.46 More evidence and special consideration is needed in these contexts with respect to refugee health, particularly for those most at risk subgroups such as women, children and the elderly.
Although there exists reaffirmed enthusiasm in intersectoral approaches to achieving global health agendas such as the SDGs, it has been found that the lack of quality evidence represents an essential hurdle to evidence-informed decision-making for the development of cross-cutting policies and governance required for sustained intersectoral collaboration.44 This pattern of a dearth of evidence was seen in our review. Additionally, most of what has been written has not been grounded in relevant theories or frameworks.45 Our use of frameworks to structure our analysis is a step forward in addressing this issue. Generating high-quality data in health systems and policy research for migrant health and on intersectoral approaches has been identified as a research priority.44 47 Future research should, therefore, also consider the structured evaluation of evidence through a frameworked approach.
Conclusion
Refugees experience individual, institutional and system-level obstacles when seeking healthcare. To ensure adequate health services tailored to this vulnerable population, conducting research and gathering quality evidence on integrated and intersectoral approaches is a top priority. This scoping review has highlighted important gaps in current knowledge and made suggestions for future research relevant to key themes.
Our findings indicate that policies aiming at integrating services and fostering intersectoral action should consider system-level approaches such as the colocation of services, transportation support and establishing system navigator roles. Communication challenges due to language barriers should also be addressed with a view of providing culturally sensitive programmes. There is also a need to strengthen the capacities of front-line providers and managers, to improve their knowledge of available services as well as their ability to provide care to specialised vulnerable groups such as refugees. Engaging host communities around a human rights-focused strategy to the health of refugees is also fundamental to address discrimination and stigma. Current gaps in knowledge found in our study represent an untapped potential for improvements to financial and human resource efficiency in health systems. Given the limited evidence, we found in our scoping review, the momentum for continued research should be sustained.
Acknowledgments
The authors would like to thank Karolinska Institutet librarians, Magdalena Svanberg and Gun Brit Knutssön, for their contributions, specifically in running the search and identifying appropriate databases. We are also grateful to WHO Euro for their discussions and suggestions in the early stages of this project.
References
Footnotes
Contributors GT together with librarians at Karolinska Institutet identified databases and planned the literature search. SH and DJ drafted the paper and incorporated coauthor feedback, SH and DJ abstracted data from peer-reviewed literature. SC, EVL, GT and PF provided critical feedback and comments on the manuscript. SC and SH acted as secondary reviewers.
Funding No funding was obtained for this project. In-kind time contributions from staff at the Alliance for Health Policy and Systems Research and SIGHT have made this possible.
Competing interests None declared.
Ethics approval Ethics approval was not required for this scoping review as human subjects are not involved.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No data are available.
Patient consent for publication Not required.