Article Text

Abstract
Objectives To determine the role of central obesity (CO) in the onset and severity of joint pain and in predicting cardiovascular disease (CVD) in subjects affected with osteoarthritis (OA).
Design Retrospective analysis on the onset of OA joint pain and CO. Waist circumference (WC), Waist-to-height ratio andwaist-to-hip ratio (WHR) were measured at the interview and defined according to the WHO criteria. Cross-sectional analyses on the association of comorbidities, including CVD, pain severity (number of joints and pain score) and CO.
Settings and participants Medical records and interviews of a hospital cohort study of 609 patients with OA. Analyses included analysis of variance, mean differences (MDs), SE and logistic regression. Areas under the receiver operating characteristic curve (AUROC) compared the predictive value of the sex-specific CVD models.
Outcome measures Onset of OA joint pain (years) and severity according to body mass index (BMI) and WC categories. Predictive value of WC for CVD by sex. Education level, disability, smoking and alcohol use were used to adjust the analysis.
Results Subjects with OA and CO by WHR started 2 years earlier with pain symptoms and had more joints affected than those without CO (MD=1.96 years, SE=0.95, p=0.04 and MD=0.32, SE=0.15 and p=0.04, respectively). Age and hypertension were associated with CVD in both genders, and NSAIDs use only in males. In addition, respiratory disease, hypercholesterolaemia, stairs difficulty, a wider WC and obesity were significant risk factors in females, improving 12.7% in the prediction of CVD cases, compared with only age and BMI (AUROCC=0.793 and 0.666, respectively, p=0.03 for the difference between AUROCs).
Conclusion CO is associated with the onset of joint pain, and all pain analysed variables. CO has a role in CVD in women affected with OA and might help predict CVD cases.
- RHEUMATOLOGY
- EPIDEMIOLOGY
- Musculoskeletal disorders
- PUBLIC HEALTH
- Cardiac Epidemiology
- Hip
Data availability statement
Data are available on reasonable request. The data supporting this study’s findings and the program codes used in the analyses are available from the corresponding author (MCC-B) on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The study focused only on patients with hip and knee osteoarthritis, clinically and radiologically defined.
The results are generalisable only to patients with osteoarthritis and not all elderly.
Different definitions of abdominal obesity based on waist circumference were used, being these measures easy to reproduce.
The study presents cross-sectional associations between cardiovascular disease, pain and central obesity, representing a limitation.
Sex stratification was necessary; however, for some analyses, the power decreased.
Introduction
Osteoarthritis (OA) is characterised by joint pain, stiffness, loss of movement and a higher prevalence of women affected than men. OA is among the ten most disabling diseases in developed countries, a complex disease where local and systemic factors interact, increasing prevalence with ageing.1 The disease curse with significant pain and disability, producing a considerable loss of quality of life and impairment of locomotor function with the disease’s progression.2
Factors associated with joint pain are sex and body mass index (BMI), among others. Subjects with higher BMI is at increased risk of knee OA and pain. The risk of knee OA increases by around 35% with a 5 kg/m2 increase in BMI, and the pain score proportionally increases with the stage of obesity.3 4
However, BMI does not represent all the burden of adiposity on OA. BMI does not account for age, sex or body composition differences.5 In addition, BMI may not accurately predict actual fat mass if the value is below 30 kg/m2. Waist circumference (WC) and waist-to-hip ratio (WHR) reasonably estimate the visceral and subcutaneous abdominal adipose tissue.6 In addition, they are easier and cheaper to measure than the visceral or abdominal fat measured by DXA scans.
Central obesity alone has been less studied than metabolic syndrome in its association with OA. Despite the study of metabolic syndrome in OA, it is unclear whether the simple presence of the syndrome, all risk factors together, or a unique risk factor like excessive abdominal obesity more optimally quantifies and predicts the cardiometabolic risk in patients with OA.
Regarding the association of abdominal obesity with pain, recent evidence linked WC with low back pain (LBP) in all populations and visceral fat (measured by Dual-energy X-ray absorptiometry (DXA)) with worsening knee pain in patients with OA.7 8 Central obesity is only associated with OA symptoms, knee pain and LBP, not structural changes.8 9
Abdominal obesity is highly correlated with cardiovascular diseases (CVD) and mortality due to coronary artery disease.10 11 CVD is the leading cause of death in men and women; however, the prevalence is higher in women. Some authors consider that determination of the CV risk profile should consider differences in the impact of major CV risk factors leading to a worse outcome in women.12 The risk of CVD in patients with OA increases by 24% compared with the general population, and CVD is the highest cause-specific mortality in this population. A WC or waist-to-hip ratio measure and other risk factors might help predict the risk for CVD in patients with OA.13 14
Previous studies did not analyse the role of central obesity on the onset of symptoms in patients with OA and as an independent factor of BMI in all OA-pain-related phenotypes. We hypothesised that central obesity is associated with an early onset of joint pain and pain severity in patients with OA, independent of BMI.
Besides, the risk associated with CVD increases with age in men and women, compounded by additional factors, principally comorbidity. Central obesity is a significant risk factor for CVD, including myocardial infarction (MI) in both sexes. A higher WC and waist‐to‐hip ratio confer a greater excess risk of MI in women than in men.15 Therefore, we want to determine which sex-specific risk factors, including central obesity, are associated with CVD and their predictive value when compared with baseline characteristics, age and BMI. Clarifying the role of central obesity on pain and CVD might have implications for public health and prevention management strategies for patients with OA.
Materials and methods
Patients and data sources
This retrospective cohort study first examined medical records from 1290 patients who attended the orthopaedics outpatient clinic between 2016 and 2019, referred from other services (general practices and rheumatologists) with advanced hip or knee joint wear and persistent joint pain. Orthopaedic surgeons with a subspeciality in hip and knee diagnosed the joint disease (MASM and EM, with a subspecialty in the knee and hip joint, respectively).
Patients diagnosed with necrosis, fractures or osteomyelitis, and rheumatoid arthritis were excluded (n=214).
Definition of patients with OA, central obesity and CVD
Hip or knee radiographs of the patients with OA were graded based on ‘The American College of Rheumatology’ and the ‘European League Against Rheumatism’ or Kellgren and Lawrence score (KL). An orthopaedist made the diagnosis of definite OA during the consult. Seven hundred and seventy patients with a confirmed diagnosis of definite OA and willing to participate were interviewed.
Patients were asked for the age of onset of OA pain in years, which joint was first affected, which joints were currently affected by pain and in the last month using the Numerical Rating Scale (NRS) and whether they used painkillers and which type. In addition, height (cm) and weight were measured (90%) or self-reported (10%), and BMI was calculated. The waist (cm) was the smaller circumference at the level of the umbilicus, between the lower margin of the last pelvic rib and the top of the iliac crest. The waist-to-height ratio (WHtR) is calculated by dividing WC by height. The hip circumference (cm) measurement was taken around the widest part of the buttocks, with the patient in an upright position. We could not take these measures in a group of patients with motor impairment, morbidly obese or unable to stand, and some other few refused to perform the measurements (16%). The values of these variables were used as raw or standardised values. All analyses regarding WC, WHtR or WHR were performed on 609 subjects with those measures.
Central obesity is a waist hip ratio (WHR) of ≥0.90 in men or ≥0.85 in women, according to the WHO.6 Central obesity was considered by using the WC or the binary classification as a large circumference when men were ≥102 cm, and women were ≥88 cm. For WHtR, we used a cutoff ≥0.5 for binary classification. A WHtR cut-off of 0.5 can be used in different sex and ethnic groups and is generally accepted as a universal cut-off for central obesity in children (aged ≥6 years) and adults.16
We identified comorbidities and converted them to International Classification of Diseases, Tenth Revision (ICD-10) codes if needed. Comorbidity was defined as the prevalence of a chronic disease or condition with a diagnosis at the moment of the interview. We classified those as cardiovascular (we included only confirmed cases with a diagnosis of heart congestion, valvular disease, infarction and history of cardiac ischaemia or MI).
Other diseases included were arterial hypertension, hypercholesterolaemia, diabetes mellitus, self-reported anxiety or depression, infectious and respiratory diseases. The patients were asked about analgesic consumption and which type and to classify the ability to walk and climb stairs (without difficulty or some difficulty (0) vs significant difficulty or inability (1)). Smoking and alcohol use were classified as current/past versus ever used. Physical activity was defined as current or past, any sport at least three times per week versus never. Educational level, binary, as those without education or only primary school (0) vs others (1). We analysed the association of comorbidity with central obesity, considering they could be potential confounders in the relationship with pain. In addition, we determine their role in the association with CVD.
We used logistics, linear regressions and analysis of variance. Mean values with SD, mean differences (MDs) with SE or OR and 95% CI are presented. The bivariate Pearson correlation was used to determine if a statistically significant linear relationship exists between waist-derived variables (WHR, WHtR, WC). Multivariate logistic regression models (enter method) were used to estimate the association between joint pain, central obesity and BMI adjusted by age and gender. The role of comorbidity and central obesity as risk factors for CVD were analysed with logistic regression, the backward conditional method. We determined the final model using conditional backward elimination with alpha-to-remove equal to 0.2. The area under the receiver operating characteristic curve (AUROC) was used to calculate and compare the models containing only age, BMI and gender and models containing significant risk factors found through the backward logistic regression method for CVD. The ideal model would have an AUROC of 1, whereas a random guess would have an AUROC of 0.5. ROC analysis provides a valuable means to assess a model’s diagnostic accuracy and compare the performance of more than one variable for the same outcome. We used DeLong’s method (1988) to compare AUROC between the models, where a p<0.05 means that one model predicts a better outcome than the other.17 The probability of a type I error was set to 0.05 for all analyses. Analyses were done using SPSS (V.25.0) and MedCalc for Windows (MedCalc Software, Ostend, Belgium), V.15.0.
Patient and public involvement
Patients and the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Results
Baseline characteristics
The population consisted of 609 subjects with complete data, including BMI, waist and hip circumference measures. Fifty-nine per cent were females with a mean age of 65.3±11 (table 1). After the knee (50%), the lower back for both groups was the body region more affected by pain (36%). The population was obese (48%), with a mean BMI of 30.3±5.7 (kg/m2). Only 30% of the population had college or higher educational levels, and only 18% considered themselves physically active. Thirty-one per cent of patients had difficulty or were unable to walk. The most common comorbidity was hypertension (66%), followed by hypercholesterolaemia (36%) and diabetes (29%).
Baseline characteristics of the 609 participants included in the study*
There was a high correlation between the central obesity variables WC and WHtR (90%, p<0.001), WC and WHR (89%, p<0.001) and WHR-WHtR (98%, p<0.001).
Regarding pain, the mean pain score was 7.3/10 (±3), and the number of joints affected by pain was 2.7±1.5. The mean age to start with OA symptoms (pain) was 53±13. When classified by WHtR, only 5.3% of the population had a ratio below 0.5. Central obesity, when classified by WC, was present in 68% of the population (n=416). Obesity by BMI was prevalent in 48% of the population (n=293). Figure 1 shows the distribution of central obesity defined by WHR and obesity defined through the BMI in the population with OA. Only 88 subjects, 14% of the population (not included in the figure), were not classified as obese by BMI or WHR.

Distribution of obesity and central obesity in the population with osteoarthritis. Central Obesity was defined by waist-to-hip ratio (WHR), and obesity was defined through the body mass index (BMI ≥30 kg/m2). The total number of subjects was n=609, the 14% had no obesity (n=88).
Central obesity by WC was associated with age 60 years or older (OR 1.78, 95% CI 1.23 to 2.58), female sex (OR 4.8, 95% CI 3.38 to 6.7), BMI (OR 1;59, 95% CI 1.47 to 1.72), hypertension (OR 2.9, 95% CI 2.05 to 4.2), diabetes mellitus (OR 2.27, 95% CI 1.49 to 3.44), hypercholesterolaemia (OR 1.93, 95% CI 1.32 to 2.82) and low educational level (OR 1.49, 95% CI 1.03 to 2.16). Finally, WC was associated with alcohol intake (p=0.003) but, it was not significant after adjustment by gender (p=0.47). Similar associations were found between central obesity by WHR and these variables. However, central obesity, when categorised by WHR, was more prevalent in males than females (OR 1.77, 95% CI 1.19 to 2.63), and was less associated with BMI than WC (OR 1.05, 95% CI 1.02 to 1.09). There was no association of central obesity with all other demographic or comorbidity variables.
Associations of central obesity with pain severity
Central obesity by WC was associated with a higher pain score by NRS in the univariate analysis (table 2, MD=0.77, SE=0.26, p=0.005) and after adjustment for significant covariates age, BMI, gender, alcohol intake and educational level (MD=0756, SE=0.34, p=0.027). It was associated with a higher number of joints with pain (table 2, MD=0.45, SE=0.13, p=0.001).
Risk factors associated with joint pain in patients with osteoarthritis
Central obesity measured by WHtR was associated with a higher number of joints with pain (table 2, MD=0.60, SE=0.24, p=0.014); and age of onset of pain (table 2, MD=4.5, SE=2.0, p=0.02). After adjustment for age, gender and BMI (p=0.03 and p=0.38, respectively).
We classified the population according to obesity by BMI and central obesity by WC to analyse these factors’ independent and combined role on pain severity (figure 2). Male or female patients with both types of obesity had a significant increase in OA pain compared with only BMI obesity, central obesity or without obesity (figure 2, P trend=0.039). In general, subjects with both types of obesity had one point more in the NRS score than subjects without any obesity (MD=1±0.28). Central obesity, when categorised by WHR, was not significant concerning pain severity (table 2, p=0.64). Central obesity measured by WHR was significantly associated with an earlier onset of joint pain (2 years earlier) than subjects without central obesity (MD 1,96 years, SE=0.95, p=0.04). Obesity (BMI ≥30) was associated with pain onset in univariate analysis (table 2, p=0.05), but it was not after adjustment for significant covariates (p=0.33).
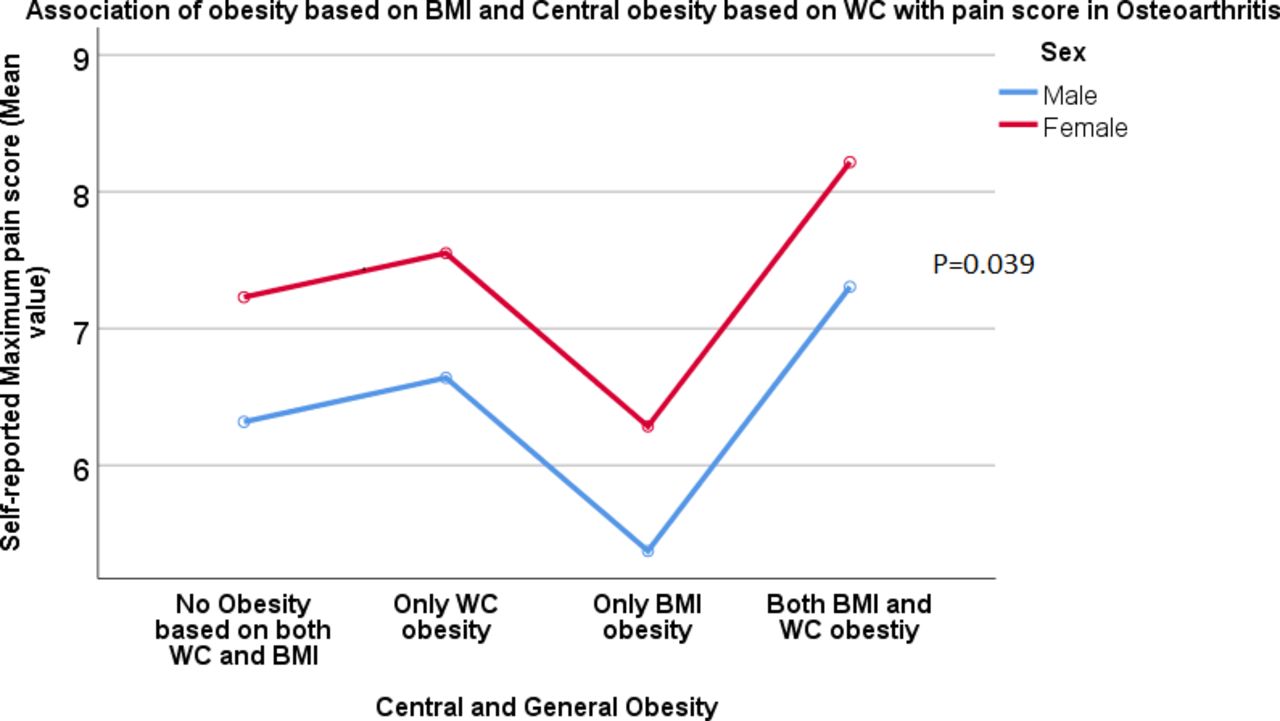
Association of obesity (BMI ≥30 kg/m2) and central obesity by waist circumference (WC) with pain severity defined by the maximum pain score registered in the Numerical Rating Scale. BMI, body mass index.
Central obesity (WHR) was associated with more joints affected by pain when compared with subjects without central obesity (MD=0.32, SE=0.15, adj-P=0.036). These analyses were adjusted by age, gender, BMI and educational level, which were significant in the relationship between central obesity and the onset of OA pain. Central obesity by WC was not significantly associated with the onset of joint pain (table 2, p=0.93). Subjects with central obesity and BMI obesity started with OA symptoms 3.4 years earlier (figure 3, P trend=0.033). They had approximately 25% more joints affected by pain than subjects without any type of obesity (figure 4, p=0.05). Sex, age and educational level were included in the model.

Association of obesity (BMI ≥30 kg/m2) and central obesity by the waist-to-hip ratio (WHR) with the onset of osteoarthritis pain in years of age. Y-axis represent the mean age. BMI, body mass index.

Association of obesity (BMI ≥30 kg/m2) and central obesity by the waist-to-hip ratio (WHR) with the number of joints affected with pain. Y-axis represents the mean number of joints. BMI, body mass index.
Finally, subjects with central obesity (WHR) had approximately two and half times higher odds of pain in the foot or ankle (OR 2.52, 95% CI 1.10 to 5.75) and borderline significant LBP (OR 1.44, 95% CI 0.93 to 2.21) than subjects without central obesity.
Cardiovascular risk in patients with OA
Eleven percent of patients with OA in this cohort had a CVD diagnoses. In order to investigate the effect of comorbidity, obesity and other risk factors on CVD risk, two separate logistic regression models were fitted for males and females. CVD was associated with age and hypertension in males and females with OA (table 3). From all pain variables, CVD was only borderline significantly associated with the onset of joint pain in females (p=0.07). Respiratory disease, hypercholesterolaemia, difficulty on stairs, wider WC and obesity were significant risk factors in females. In males, Nonsteroidal anti-inflammatory drugs (NSAID) use was the only other significant factor (table 3). These variables were part of the final model from the conditional backward logistic regression (table 3).
Results of separate backward regression models for women and men
The other two central obesity variables (WHtR and WHR) did not perform better than WC in the same model being excluded from the final selected model, except WHtR in males, which still was significant in a final model containing age, HTA and WHtR (p=0.04).
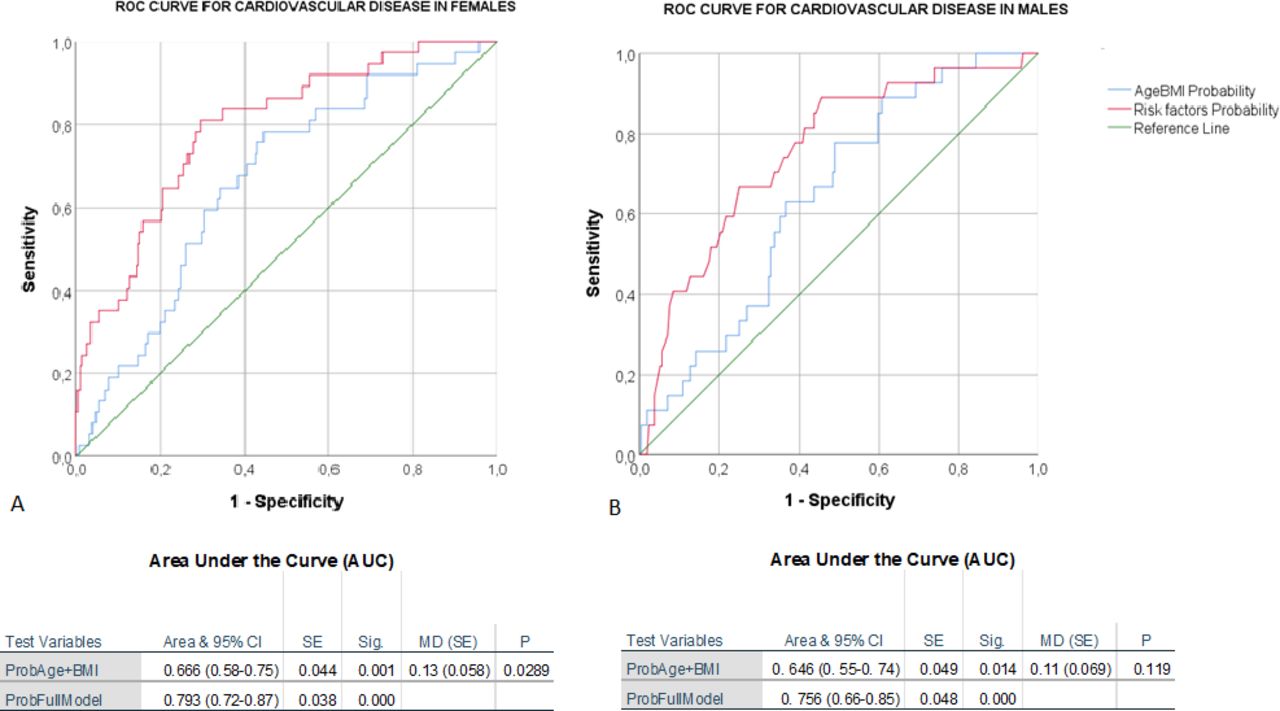
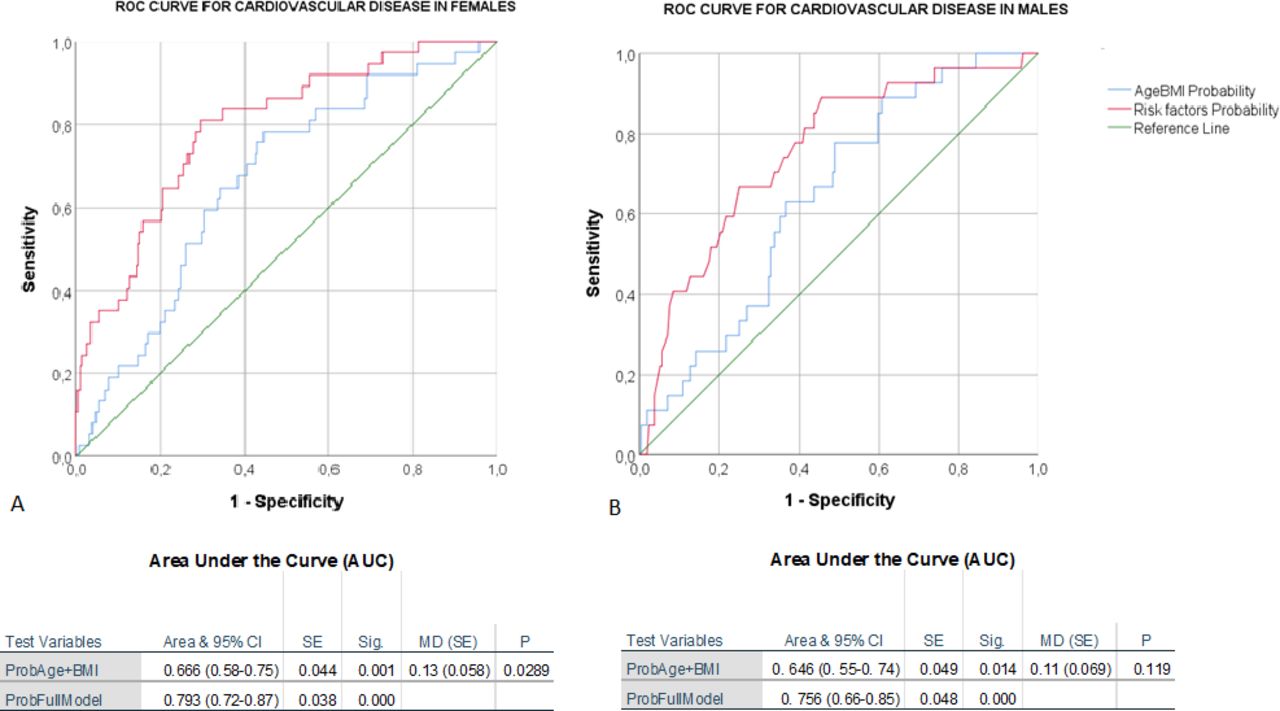
Regarding the predictive value of these factors, a model for males including age, hypertension and NSAIDs consumption increased the prediction of cases with CVD compared with a model with only age and BMI but did not achieve a significant statistical difference (figure 5, AUC=0.756 (SE=0.048) and 0.646 (SE=0.049), respectively, p=0.12 for the difference between AUROCs). In addition, the model for females included age, respiratory disease, hypercholesterolaemia, difficulty on stairs, WC and obesity. This model was better at predicting CVD cases than a model containing age and BMI only (figure 5, AUC=0.793 (SE=0.038) and 0.666 (SE=0.044) (respectively), p=0.03 for the difference between AUROCs).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Areas under the receiver operating characteristic curve for prediction of cardiovascular disease in females and males with osteoarthritis. The first model contained only age and BMI. full models contained the significant risk factors found through the backward logistic regression method for cardiovascular disease. BMI, body mass index.
Discussion
Pain is one of the most relevant aspects for patients with OA. Pain leads to decreased quality of life and increased disability, a risk factor for CVD in OA.18 According to the results of this study, central obesity is associated with pain severity, including the onset of joint pain in all subjects with OA and CVD in female patients with OA. These associations are independent of BMI. Obesity is a known risk factor for CVD and pain; however, these results show that central obesity is more relevant to pain and CVD in patients with OA than BMI. Altogether, central obesity and a high BMI were present in 39% of this population and had an additive effect significantly impacting joint pain. Subjects with a BMI of 30 kg/m2 or higher and central obesity had a 14% higher VAS score, 25% more joints affected and 3 years earlier onset of OA symptoms compared with subjects without central obesity.
Central obesity was one of the significant factors in predicting CVD in female patients with OA. A model containing age hypertension, respiratory disease, hypercholesterolaemia, stairs difficulty, obesity and wider WC was around 13% better than a model containing age and BMI to predict CVD cases. The model for males with OA contained only NSAID use, hypertension and age. These three factors were not significantly better than age and BMI alone. A previous study with 480 000 participants concluded that although excessive central adiposity has deleterious effects on the risk of MI in both sexes, a higher WC and waist-to-hip ratio conferred a greater risk of MI in women than in men.15 That could be a reasonable explanation for a more critical role of central obesity in the cardiovascular risk of female patients than males. In addition, the WHtR was only significant in males. WHtR could be a better predictor of CVD in males than WC, as previously discussed in literature.19
Patients with OA have comorbidities and a higher mortality rate associated with BMI, but the association with visceral fat is emerging as a more decisive factor. Visceral adiposity (measured by WC and waist-to-hip ratio) is considered superior to BMI as a risk factor for CVD.20 These factors, together with respiratory disease, hypercholesterolaemia and restriction in mobility, might explain the increased cardiovascular risk of female patients with OA compared with the general population. Abdominal obesity is considered a dominant MetS feature in women, whereas risk factor combinations are more varied in men.21 In addition, the considered metabolic type of OA seems to be female-specific.22
Previously, WC was associated with an increased risk of TKA for OA.23 We hypothesise that this relation is fully mediated by central obesity with joint pain, considering that visceral fat has been associated only with pain and not with structural outcomes.8 Visceral fat produces high interleukin-6 (IL-6) levels, resulting in increased systemic inflammation.24 Higher levels of IL-6 reflect synovitis and are associated with pain in early-stage and advanced-stage knee OA.25 IL-6 is considered a predictor of knee OA.25 26 In addition, adipocytes produce cytokines which contribute to the transition from acute to persistent pain and correlate with lower limb joint pain severity before arthroplasty.23 24
This study confirms the association of abdominal fat with the number of joints affected by pain and specific joint sites. One study reported a borderline association of visceral fat with the total number of joints affected by pain. In general, there is an indication that high body fat increases the risk of incident OA and worsening joint pain.8 9 Meta-analyses have confirmed the association of central obesity with LBP. Individuals with increased WC or WHR tended to have an increased risk of LBP, regardless of their BMI.7 27 The association of WHR with foot pain was significant in this study and other studies using visceral fat of total body fat (only in women).9 28 Identifying risk factors and their importance in different genders is essential to preventing, diagnosing and managing CVD properly in patients with OA.
Regarding the cardiovascular risk for subjects with OA, several studies have pointed to disability and, in general, the worsening function that the patients suffer as responsible for the increased risk.14 18 29 However, this is the first study that included a measure of abdominal fat as a risk factor for CVD in a population with OA. According to the results, not only disability and obesity but abdominal fat measured by WC might help predict CVD cases in females. Prospective studies will be essential to confirm these results.
There is evidence from observational studies regarding the association between chronic pain and CVD. We only found a trend for association between CVD and the onset of joint pain in females. Chronic pain has been associated with an increased risk for MI and cardiovascular death, independent of other risk factors.30 However, it might be mediated by disability.18 Subjects with disability produced by joint pain reduce their physical activity, social interaction and, in general, quality of life, in addition to the increased use of NSAIDs that has been mentioned as one of the responsible factors in this association31
Our study has some limitations. First, as mentioned, this study presents cross-sectional associations related to CVD-central obesity and retrospective regarding pain onset, which will be more valid when repeated with longitudinal samples. The participants determined the age of pain onset according to the first visit to the Hospital and their recall of events, which might introduce some errors. There were no available scores of KL to determine the association of structural parameters with central obesity, measures of the total truncal or visceral fat percentage or lab measures of adipocytokines, inflammatory cytokines or other markers such as CRP. Differences in the prediction models for CVD risk in males might represent a lack of power in the analysis, considering that the female group is more prominent than male patients. Finally, despite adjustment for important confounders, there might be other potential confounders in the association of central obesity with joint pain and CVD that were not included.
In conclusion, central obesity is a crucial factor (independent of BMI) regarding joint pain that might influence an earlier onset of OA symptoms. In addition, central obesity is a risk factor for CVD in female patients with OA. Central obesity is a modifiable factor that should be further studied using randomised clinical controlled trials to prevent and decrease joint pain and cardiovascular risk in patients with OA.
Cardiovascular comorbidity in patients with OA is crucial to be studied, considering that CVD is the leading cause of morbidity and mortality in the general population and the risk of CVD is 24% higher in patients with OA compared with the general population.14
Possible implications for clinicians include that controlling WC and visceral fat should be considered a target for any preventive programme and pain management for patients with OA. The medical community and guidelines should include the reduction of WC, not only weight or BMI, as a recommendation for patients with OA. Measures of abdominal fat, including WC, should be used to monitor the risk and progress in risk reduction for patients with OA. Finally, future research will analyse whether reducing and controlling abdominal fat at early ages will reduce the risk of developing OA and CVD in longitudinal population samples.
Data availability statement
Data are available on reasonable request. The data supporting this study’s findings and the program codes used in the analyses are available from the corresponding author (MCC-B) on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the medical ethics committee of the Faculty of Medicine of Jundiaí (FMJ), ethics approval numbers: 1.183.488 and 4.950.422. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We are thankful to all patients, residents, the Hospital's orthopaedic department, and the MSc students Catrine Rangel Maia and Caroline Larissa Morais, who helped collect data. The data supporting this study's findings and the program codes used in the analyses are available from the corresponding author MCB upon reasonable request.
References
Footnotes
Twitter @emachadodr
Contributors All authors approved the final version before submission. Conception and design (MCC-B, EM), analysis and interpretation of the data, drafting of the article (KRR, RFA, MASM, EGM, EM, MCC-B), critical revision of the article for important intellectual content (KRR, MCC-B), Provision of study materials or patients (KRR, MASM, EGM), statistical expertise and funding (MCC-B), administrative, technical, or logistic support (EM, MASM, EGM), collection and assembly of data (KRR, MCC-B). MCCB (castanomc@yahoo.es) takes full responsibility for the integrity of the work from inception to the finished article, has access to the data, and controlled the decision to publish.
Funding This work was supported by the São Paulo Research Foundation (FAPESP) grant N. 2016/21039-0.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.