Article Text

Abstract
Objective This study sought to evaluate the diagnostic performance of the 1-hour troponin algorithm for diagnosis of myocardial infarction (MI) without persistent ST-segment elevations (non-ST-segment MI (NSTEMI)) in a cohort with a high prevalence of MI. This algorithm recommend by current guidelines was previously developed in cohorts with a prevalence of MI of less than 20%.
Design Prospective cohort study from November 2015 until December 2016.
Setting Dedicated chest pain unit of a single referral centre.
Participants Consecutive patients with suspected MI were screened. Patients with subacute symptoms lasting more than 24 hours, new ST-segment elevations at presentation, or an already diagnosed or ruled-out acute MI were excluded. All enrolled patients (n=1317) underwent a full clinical assessment and measurements of high-sensitivity troponin, and were scheduled for an early invasive strategy if clinically indicated.
Main outcome measures Final diagnosis of MI according to the Fourth Universal Definition of MI.
Results The prevalence of NSTEMI in the present cohort was 36.9%. The sensitivity for rule-out of MI was 99.8%. The specificity for rule-in of MI was found to be 94.3%. However, in 35.7% of patients neither rule-in nor rule-out was possible. In 51.4% of patients diagnosed with MI, a primary non-coronary reason for MI was found (type 2 MI). Different receiver operating characteristic-curve derived cut-offs for troponin and its dynamics did not provide a sufficient differentiation between type 1 and 2 MI for clinical decision making (negative predictive value for rule-out of type 1 MI <70%).
Conclusions The 1-hour diagnosis algorithm for patients with suspected NSTEMI can accurately diagnose acute MI in high-risk cohorts. However, discrimination between patients needing an early invasive strategy or not is limited.
Trial registration number DRKS00009713.
- myocardial infarction
- troponin
- diagnosis
- acute coronary syndrome
- coronary heart disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This prospective cohort study evaluated the 1-hour troponin algorithm in a cohort of patients at high risk for acute myocardial infarction (MI) (prevalence of MI approximately twice as high as compared with previous cohorts).
All patients enrolled in this study underwent a comprehensive cardiac assessment including echocardiography and an early invasive strategy if clinically indicated.
This allows the use of this algorithm in further settings such as specialised heart centres and chest pain units.
The present analysis used one specific troponin assay, so findings cannot be extrapolated to different troponin assays
Introduction
The early and accurate detection of myocardial infarction (MI) is crucial for rapid initiation of treatment, which reduces risk in these patients.1–5 Together with a precise clinical assessment, 12-lead ECG, and imaging studies, testing of biomarkers of cardiac necrosis such as cardiac troponin is necessary for the rapid diagnosis of non-ST-segment MI (NSTEMI).2 5 The development of high-sensitivity cardiac troponin (hs-cTn) assays allows nowadays the measurement of very low concentrations of cardiac troponin with high precision.6 The better sensitivity for MI of these assays as compared with previous assays allowed the development of rapid diagnosis algorithms for patients with suspected NSTEMI, which can rule in or out MI already within 1 hour.7–13 The performance of this 1-hour diagnosis algorithm for patients with suspected NSTEMI was validated in independent cohorts,13 14 and is recommended by the current guidelines of the European Society of Cardiology (ESC).5
The cohorts used for development and validation of this algorithm enrolled unselected patients in emergency departments, which is also reflected by the relatively low rate of MI in these cohorts ranging between 11% and 19% (online supplementary table 1).13–16 However, it is standard of care in many countries that patients with suspected MI are directly transferred to chest pain units or other specialised centres. The use of such units has shown to improve outcome and to be cost-effective.17–19 The prevalence of MI of these selected patients is usually much higher than that of patients in general emergency departments. However, it is unknown so far if the diagnostic performance of the 1-hour troponin algorithm persists when used in cohorts with a much higher pretest probability, which might in particular affect the negative predictive value.
Supplemental material
Thus, this study sought to evaluate the hypothesis that the good clinical performance of the 1-hour diagnosis algorithm for patients with suspected NSTEMI prevails in a prospective high-risk cohort of patients admitted to a dedicated chest pain unit with all patients undergoing a comprehensive cardiac assessment and an early invasive strategy if clinically indicated.
Methods
Study design
The FAST detection of Myocardial Infarction (FAST-MI) study was a prospective cohort study enrolling patients with suspected acute MI. The majority of patients were directly sent to the chest pain unit of our tertiary care heart centre by the ambulance service following triage of an emergency physician (>98%) or were transferred from emergency departments of general hospitals in our region. An automated algorithm of the clinical data base identified continuously all patients with suspected acute coronary syndrome and available troponin test from November 2015 until December 2016. Patients were screened and enrolled by study physicians within 48 hours following presentation to our centre. Patients had to be at least 18 years old and had to present with either typical clinical symptoms suggestive of acute MI starting within the last 24 hours before enrolment, or new typical ECG changes or typical imaging findings. Key exclusion criteria were missing troponin test results, subacute symptoms lasting more than 24 hours, new ST-segment elevations at presentation, or an already diagnosed or ruled-out acute MI (eg, by troponin testing already in a referring hospital).
Routine clinical assessment
All patients underwent a comprehensive clinical assessment according to the treatment algorithms of our heart centre including physical examination, routine blood tests, 12-lead ECG, continuous monitoring and early echocardiography (within 3 hours). Levels of hs-cTnT were measured at presentation, after 1 hour, and thereafter if clinically indicated.5 All blood samples were immediately assayed in our central laboratory.
All patients were scheduled for an early invasive strategy if clinically indicated according to current guidelines.1 5 If no early invasive strategy was planned, patients were scheduled for cardiac stress testing if clinically reasonable and tolerable for the patient.
Endpoint definitions
The primary endpoint was the final diagnosis of MI according to the Fourth Universal Definition of MI.2 Key secondary endpoint was all-cause mortality and subsequent MI within 30 days.
Two independent cardiologists reviewed all available medical records including data from the standard follow-up for quality control of our heart centre (written contact at 30 days following index event). Key focus of this review was the determination of the primary reason for elevations of cardiac troponin. If the diagnostic criteria for MI were met, patients were classified according to the different subtypes of MI according to the Fourth Universal Definition of MI.2 An automated algorithm for comparison of results sent all potential endpoints with diagnostic disagreement for blinded review and adjudication to a third cardiologist. To determine the risk of patients, the Global Registry of Acute Coronary Event (GRACE) risk score for in-hospital mortality was calculated as previously described.20
Laboratory assessment
Hs-cTnT was measured with an immunoassay (Roche Diagnostics, Mannheim, Germany). This assay has a limit of blank of 3 ng/L, a limit of detection of 5 ng/L, a 99th-percentile of a healthy population cut-off point of 14 ng/L, and a coefficient of variation of less than 10% at 13 ng/L.21 22
Patient and public involvement statement
The study used routinely collected data; therefore, no patient or public involvement was required. The results will be disseminated to potential patients via the publications of the German Heart Foundation.
Statistical analysis
The size of the present study was selected to be in range with previous studies used for development and validation of the 1-hour troponin algorithm (online supplementary table 1). Differences between groups were tested by Fisher’s exact test for discrete variables, and by Kruskal-Wallis test for continuous variables. To assess sensitivity, specificity and Youden’s index for determination of optimal cut-offs, receiver operating characteristic (ROC) curves were constructed. Clinical events during follow-up were displayed as Kaplan-Meier plot and compared by log-rank test. Statistical analyses were run with IBM SPSS Statistics V.22.
Results
Patient characteristics
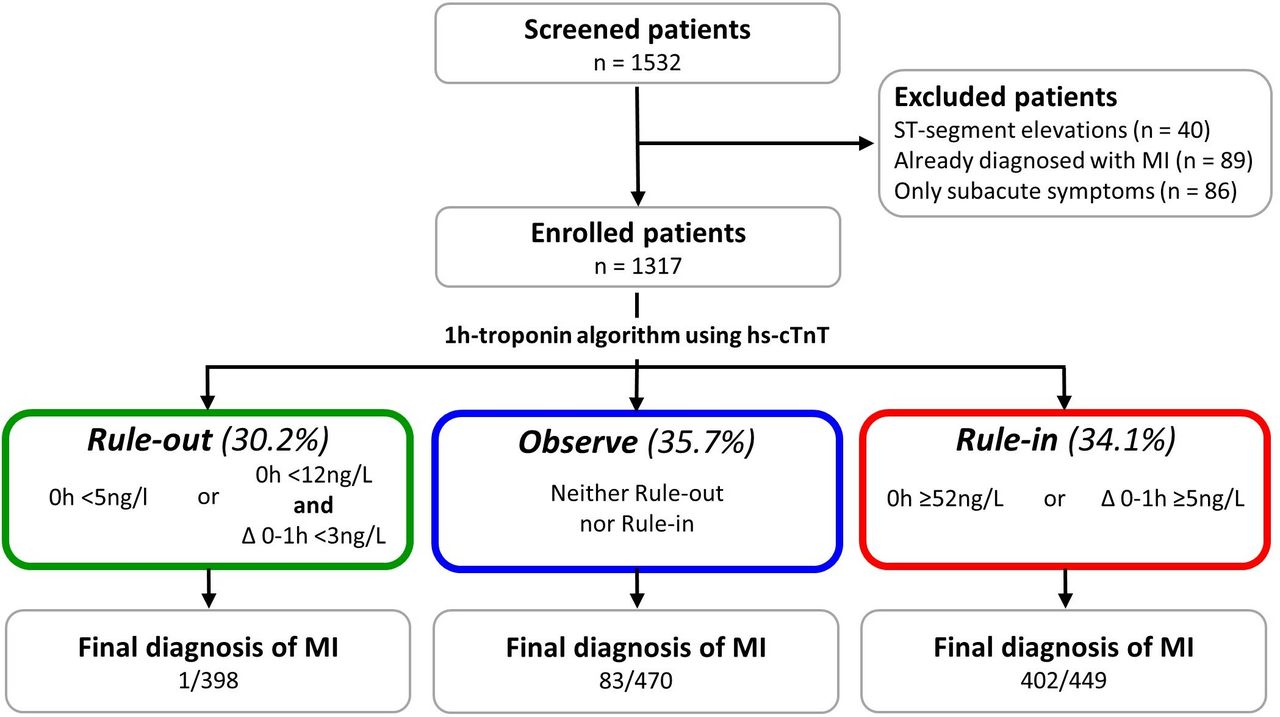
Altogether 1532 patients with suspected acute MI were screened for this study. Forty patients with presumably new ST-segment elevations and 175 patients with only subacute symptoms or already established diagnosis of MI before presentation were excluded, leaving 1317 patients for the present analysis (figure 1). When applying the 1-hour troponin algorithm, 398 patients were classified as ‘rule-out for MI’ (30.2%), 449 patients as ‘rule-in’ (35.7%) and 470 patients as ‘observe’ (34.1%) indicating that neither rule-in nor rule-out of MI was possible.

Study flow. hs-cTnT, high-sensitivity troponin T; MI, myocardial infarction.
The median age of enrolled patients was 72 years and 62% were male. 30.2% of patients presented within the first 3 hours of on-set of symptoms. There were significant differences for most variables between patients classified into the three groups of the 1-hour troponin algorithm (table 1). Patients classified as ‘rule-out’ were significantly younger, more often female, showed a lower prevalence for most cardiovascular risk factors or cardiovascular diseases, were less often on cardiovascular drugs, and had a lower GRACE Risk Score. Comparing patients in the ‘observe’ and ‘rule-in’ groups, we found a similar risk profile. Both groups showed a higher prevalence of common cardiovascular risk factors and a higher GRACE risk score as compared with patients classified as ‘rule-out’.
Baseline characteristics
Diagnostic workup
All enrolled patients underwent blood sampling, ECG and transthoracic echocardiography. The highest levels of cardiac biomarkers, the highest prevalence of ST-segment changes, T-wave inversions and impaired left or right ventricular function were seen in the ‘rule-in’ group, whereas haemoglobin and creatinine clearance was lowest in this group (table 2). The highest prevalence of supraventricular tachycardia, which was atrial fibrillation in 84% of cases, was seen in patients classified as ‘observe’.
Diagnostic workup
All patients with a high likelihood for an acute coronary syndrome were scheduled for an early invasive strategy according to current guidelines.1 5 Patients with a lower likelihood were planned for cardiac stress testing if clinically indicated and possible for the patient. Altogether, 858 patients (65.1%) underwent either stress testing or coronary angiography. 377 patients (28.6%) received a coronary intervention (table 2). 98.7% of patients diagnosed with type 1 MI underwent angiography and 95.3% percutaneous coronary intervention (PCI) or bypass surgery. The remaining three patients refused an invasive strategy. Patients without MI as final diagnosis received stress testing and/or coronary angiography in 62.0%. 16.8% of these patients needed coronary revascularisation. Altogether, 94 out of 250 patients diagnosed with MI type 2 (37.6%) and 312 of 832 (37.5%) without MI underwent coronary angiography.
The adjudicated final diagnosis was MI in 486 patients (36.9%). When stratified according to the Fourth Universal Definition of MI, 235 of MIs (48.4%) were classified as type 1 (spontaneous MI), 250 (51.4%) as type 2 (MI secondary to an ischaemic imbalance) and one patient died due to acute MI on admission before any invasive treatment or second blood sample could be drawn (type 3 MI). Patients in the ‘rule-in’ group were diagnosed with MI in 89.5% as compared with only 17.7% of patients classified as ‘observe’ (table 3). One patient classified by the 1-hour troponin algorithm as ‘rule-out’ was diagnosed with MI (type 1). This patient was presenting with typical chest pain lasting for several hours that stopped after administration of heparin, nitrates and morphine. The initial hs-cTnT was 11 and 13 ng/L after 1 hour. However, the pain-free patient developed within the next 5 hours a more than 70-fold rise in troponin. The coronary angiography showed a subtotal stenosis of the right coronary artery, which was treated by PCI.
Final diagnosis and clinical follow-up
Obstructive coronary artery disease was not an uncommon finding in the ‘rule-out’ group since 10.1% of patients were diagnosed with unstable angina as main diagnosis and underwent coronary intervention.
Performance of algorithm
The sensitivity for rule-out of MI of the algorithm was 99.8% (95% CI 98.5% to 100%) in our cohort (negative likelihood ratio of rule-out: 0.004; negative predictive value for rule-out: 99.8%). The specificity for rule-in of MI was found to be 94.3% (95% CI 92.6% to 95.8%; positive likelihood ratio of rule-in: 14.62; positive predictive value for rule-in: 89.5%; figure 1; online supplementary table 1). Four hundred and seventy patients (35.7%) were classified as ‘observe’ indicating that neither ‘rule-in’ nor ‘rule-out’ was possible. When including these patients into the calculation, the sensitivity of the 1-hour troponin algorithm for diagnosing MI was 82.7% (95% CI 79.6% to 85.6%) and its specificity 47.8% (95% CI 45.9% to 49.4%).
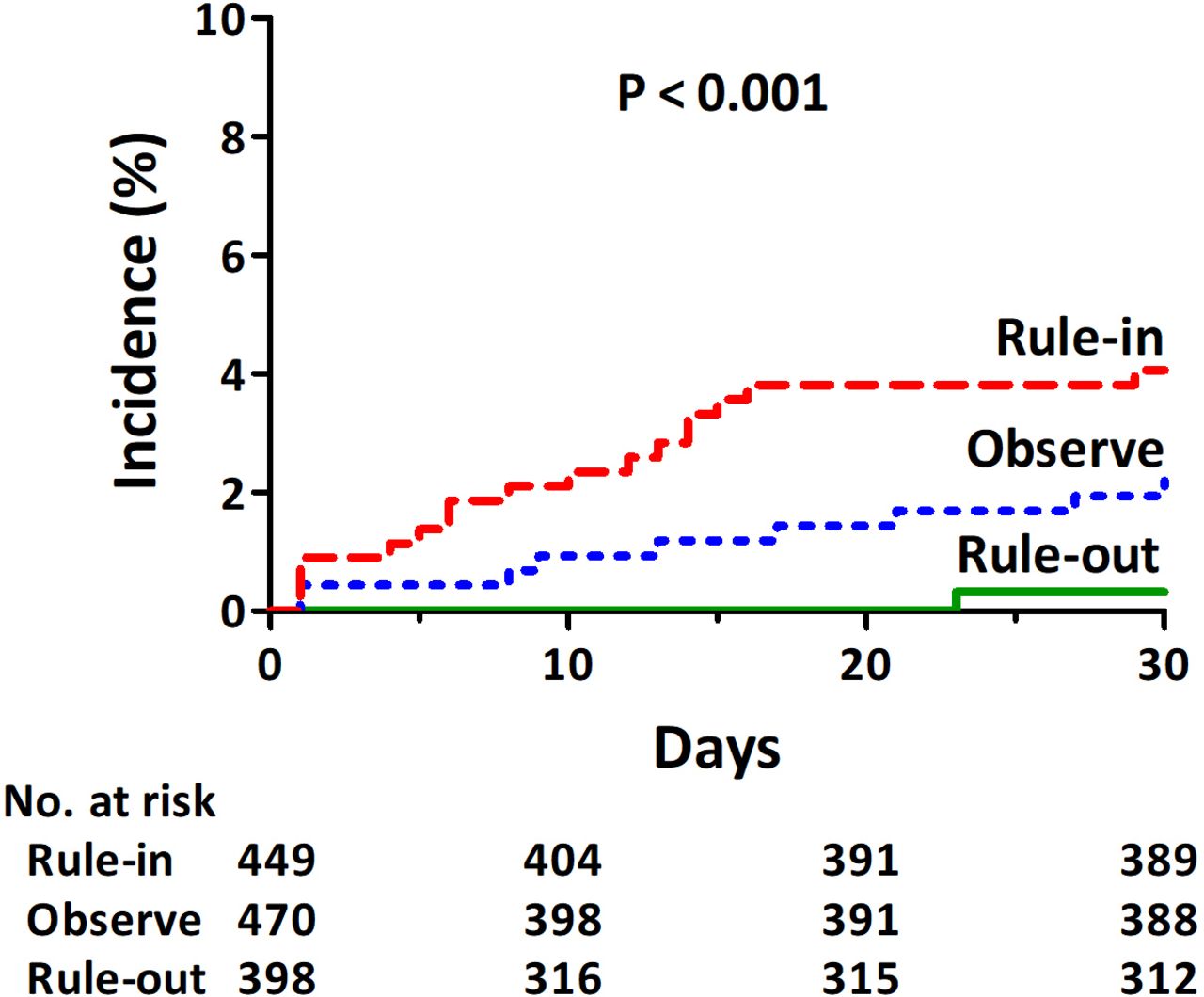
Clinical follow-up
A complete 30-days follow-up was available in 85% of patients (mean follow-up 25±10 days). Within 30 days following enrolment, 26 patients died, one patient developed a type 2 MI during an episode of acute heart failure and two patients were readmitted for acute chest pain and underwent unplanned percutaneous coronary intervention (table 3; figure 2). Mortality was significantly higher in the ‘rule-in’ group as compared with the two other groups. The most common reason for death was cardiogenic shock. One fatal event occurred in the ‘rule-out’ group. This patient diagnosed with a severe psychiatric disorder and non-cardiac chest pain committed suicide 2 weeks following discharge from hospital.
{kind=link}
{kind=link}
Incidence of death, myocardial infarction, or unplanned coronary intervention within 30 days. Plot of survival functions for subgroups stratified according to 1-hour troponin algorithm for patients with suspected NSTEMI. P by log-rank test. NSTEMI, non-ST-segment MI.
Type 2 MI
The majority of patients with MI in the present high-risk cohort were finally diagnosed with type 2 MI following complete work-up (250 of 486 (51.4%)). The most common final diagnosis in these patients were arrhythmia (mainly tachyarrhythmia), acute heart failure, hypertensive emergency and valvular heart disease (online supplementary table 2). During further clinical work-up, 12 (5.2%) underwent coronary revascularisation. None of these patients did show intracoronary thrombi or subtotal coronary lesions. The main diagnoses of these 12 patients were severe valvular heart disease (n=2), acute heart failure (n=4), or hypertensive emergency (n=6).
Baseline troponin and change in troponin within 1 hour were higher in patients adjudicated as type 1 as compared with type 2 MI. There was a wide overlap with many patients diagnosed with type 2 MI showing very high levels or changes of troponin (online supplementary figure 1). One hundred and forty (56%) of patients adjudicated as type 2 MI demonstrated a significant change in hs-cTnT of ≥5 ng/L within the first hour. In the present cohort, the optimal ROC-curve derived cut-offs for baseline troponin and change in troponin within 1 hour for differentiation between type 1 and type 2 MI were 109 ng/L and 9 ng/L, respectively. The negative predictive values of these cut-offs were only 64.7% (95% CI 61.0% to 68.2%) and 67.6% (95% CI 62.5% to 72.4%) for excluding type 1 MI, and the positive predictive values for diagnosis of type 1 MI were 67.9% (95% CI 62.4% to 73.0%) and 61.3% (95% CI 57.3% to 65.2%), respectively.
Discussion
The introduction of the 1 hour troponin algorithm has improved diagnosis of MI in patients presenting to emergency departments and become a class I recommendation in current ESC guidelines.5 However, it is uncertain if these results also apply to specialised chest pain units, which are nowadays established in many large hospitals given the higher pretest probability for MI and preselection of patients in such a setting. Since chest pain units are heavily reliant on diagnostic algorithms, the validation of this algorithm in such a unit appears to be important.
The present study sought to answer this question by enrolling a large cohort of patients, sent to a dedicated chest pain unit. The prevalence of MI was with 37% more than twice as high as compared with previous cohorts (online supplementary table 1).13–16 The key finding of this analysis was that the use of the 1-hour troponin algorithm was safe for rule-out of MI even in this high-risk setting as evidenced by the high sensitivity for rule-out of MI and the low short-term mortality. The proportion of patients with rule-in of MI according to the 1-hour troponin algorithm was twice as high as the mean proportion in previous studies. For these patients, the specificity for rule-in of MI was high, which also underscores the applicability of the algorithm for important clinical decision making. However, also the known limitations were seen in this analysis including that in more than one third of patients neither rule-in nor rule-out was possible when using the algorithm, and that a high proportion of patients identified with MI were diagnosed as type 2 MI. Even if mean levels and changes in troponin were different between patients with type 1 and type 2 MI, there was such a wide overlap of values that troponin as single parameter does not appear sufficient for the clinically important differentiation between these two entities—even when applying optimised cut-offs derived from the present cohort.
A major advantage of the present study is that all patients underwent a cardiac assessment including echocardiography and an early invasive strategy if clinically indicated as recommended by current guidelines.1 5 This comprehensive diagnostic work-up allowed a precise assessment of the origin of changes in troponin levels, which is essential for accurate differentiation between various types of MI. Further important features of the present study are: the design as all-comers study; the very early enrolment of patients following on-set of symptoms; and the testing of levels of troponin as part of clinical routine from fresh samples since there have been concerns that samples stored for long periods of time could bias results.23
The results of the present study are in line with previous results of mainly lower-risk cohorts describing negative predictive values for rule-out of MI of the 1-hour troponin algorithm of above 99%.13 14 16 24 The negative predictive value of 99.8% in this cohort is remarkable since the much higher pretest probability could have negatively affected this result. Taken together with the absence of any cardiovascular death in the rule-out group, this underscores the clinical utility for precise rule-out of MI. The positive predictive value for rule-in of MI of the present cohort was with 89.5% higher as compared with previous analyses with 37.0% to 87.1%, which might be an effect of the high pretest probability for MI.
An interesting finding of this analysis was that despite the large proportion of patients in the rule-in group as compared with previous studies, the proportion of patients that could be neither ruled-in nor ruled-out by the algorithm was with still roughly one third of patients. This number is approximately in line to previous lower-risk cohorts (online supplementary table 1),13 14 16 24 indicating that the level of uncertainty appears not to decrease with a higher pretest probability. This subgroup of patients, where a rapid diagnosis is not possible with the algorithm, is often challenging to diagnose in clinical routine. In the current study, it was associated with an increased 30-day mortality, which is also in line with previous findings.25 The latter finding might be explained with the relatively similar risk profile of this group as compared with the ‘rule-in’ group in our study. The proportion of patients in this subgroup that was finally diagnosed with MI was in the present study with 17.7% in the range of previous studies (8.7%–22.5%). Another important finding of the present study was that 10.1% of patients classified as ‘rule-out’ were finally diagnosed as unstable angina needing coronary revascularisation. Even if the 30-day risk for major cardiovascular events of these patients was low, this finding underscores the need for further work-up of these patients.
When diagnosing MI, it is not only important to get a fast diagnosis but also to discriminate between type 1 and type 2 MI given the entirely different therapeutic consequences.5 While an early invasive strategy can improve prognosis in patients with type 1 MI, this has not been shown for patients with type 2 MI, where detection and treatment of the underlying, usually primary non-coronary condition is essential.1 5 26 In the present study, more than half of patients identified with MI were diagnosed as type 2 MI. This proportion was higher than in many (but not all) previous cohorts.26 27 The finding that some patients finally diagnosed with type 2 MI have concomitant obstructive coronary heart disease, was not unexpected but underscores that often a more extensive work-up is needed before a type 2 MI can be reliably diagnosed. Establishing the diagnosis of a type 2 MI appears to be of clinical importance given the different prognosis of these patients as demonstrated by a recent meta-analysis revealing an even higher mortality rate in these patients as compared with patients with a ‘classic’ type 1 MI.28
Since the rapid differentiation between type 1 and 2 infarcts is often challenging in clinical routine, different approaches have been proposed including clinical scores or interpretation of biomarkers.27 29 Given the higher troponin levels in patients with type 1 MI as previously described in other cohorts,30 31 a differentiation between a coronary and non-coronary reason by interpretation of troponin dynamics was proposed.27 In the present study, the overlap of mean levels and changes in troponin different between patients adjudicated as type 1 and type 2 MI was wide. Even it cannot be excluded that this finding was biassed by misclassification, the present data do not support that baseline troponin or its dynamics are sufficient for the clinical important differentiation between these two entities.
Study limitations
Not all patients did undergo coronary angiography or dedicated stress testing because refused by patient or missing clinical indication. Therefore, it cannot be excluded that the classification of patients for type I MI vs. type II MI was always correct. The present analysis did use one specific troponin assay. Thus, these findings cannot be extrapolated to different troponin assays. According to current guidelines, no gender-specific cut-points for troponin were used. The distribution of pathologies causing type II MI in our study might be different to that in a general emergency department. Thus, it cannot be excluded that hs-cTn might perform better for differentiation between type 1 and type 2 MI in such an undifferentiated population. A complete follow-up was not available for all patients. Thus, it cannot be excluded that the true event rate might have been higher in particular in patients in the rule-out cohort. More than 10% of patients classified as rule-out underwent coronary revascularisation following diagnostic work-up. It cannot be excluded that the event rate during follow-up would have been higher in these patients if they would have been discharged without further work-up.
Conclusions
The 1-hour diagnosis algorithm for patients with suspected NSTEMI can accurately diagnose acute MI in high-risk cohorts. This allows the safe use of this algorithm in clinical settings such as specialised heart centres and chest pain units. However, in one third of patients neither rule-in nor rule-out of MI is possible, and discrimination between patients needing an early invasive strategy or not is limited. Further studies are needed to define how these limitations can be addressed.
References
Footnotes
Contributors MA and WH: main authors of the study, established the idea to study the performance of 1-hour troponin algorithm in a high-risk cohort. Writing main ideas for this research, main results and discussion of the findings. SIS, FR, RS and FG: interpreted statistical analysis and proved the main findings. F-JN contributed on editing this manuscript and giving advice for the main authors to organise the manuscript and ideas of the project. KM, MF and CMV: contributed with study methodology.
Funding This study was supported by the German Heart Foundation and the University Heart Center Freiburg-Bad Krozingen.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Our study was approved by the ethics committee of the Albert-Ludwigs-University Freiburg.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.