Article Text

Abstract
Objectives Japan is one of the largest markets for heated tobacco products (HTPs), and the number of HTP users, including dual users, is growing. However, it is not yet clear whether a telemedicine smoking cessation programme is effective for nicotine-dependent HTP users to quit smoking. We assessed the outcomes of a telemedicine smoking cessation programme in terms of continuous smoking cessation among smokers who had used HTPs compared with those who used exclusively cigarettes.
Design A retrospective cohort study to assess the outcomes of the telemedicine smoking cessation programme provided by Linkage, Japan, comparing the success rates of smoking cessation between exclusively cigarette group (as reference) and HTP user groups (exclusively HTPs or dual use of both cigarettes and HTPs).
Setting Linkage telemedicine smoking cessation programme database, covering programme participants in Japan.
Participants Programme participants from between August 2018 and October 2020.
Outcome measures Continuous abstinence rates (CARs) from 9 to 24 weeks (CAR9–24) and 9 to 52 weeks (CAR9–52). Adjusted ORs (aORs) with 95% CIs for CAR were calculated to compare the exclusively cigarette group with exclusively HTP and dual use groups.
Results We analysed 733 telemedicine smoking cessation programme participants. Exclusively HTP users had higher CARs than the exclusively cigarette group for CAR9–24 (aOR 1.12, 95% CI 1.02 to 1.23; p=0.02) and CAR9–52 (1.09, 0.99 to 1.19; p=0.08). Conversely, dual users had lower CARs than the exclusively cigarette group for CAR9–24 (0.85, 0.76 to 0.95; p=0.004) and CAR9–52 (0.88, 0.79 to 0.97; p=0.01).
Conclusions Exclusive HTP users achieved higher CARs, whereas dual users had lower CARs than exclusively cigarette users over short-term and long-term periods. A telemedicine smoking cessation programme may be a reasonable option for exclusive HTP users.
- telemedicine
- respiratory medicine (see thoracic medicine)
- toxicology
Data availability statement
Data are available upon reasonable request. The data that support the study findings are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
To our knowledge, this is the first study to assess the outcomes of the telemedicine smoking cessation programme among heated tobacco product users and dual users compared with exclusively cigarette users.
The endpoints of continuous abstinence rates were assessed by questionnaire-based self-reported abstinence, but not biochemically validated.
We excluded participants unavailable for follow-up surveys, which could potentially affect adherence and success rates of the telemedicine smoking cessation programme.
Introduction
Smoking is a major preventable risk factor for cardiovascular diseases, respiratory diseases and malignant neoplasms.1 2 Additionally, it is the leading cause of death from non-communicable diseases and external causes in Japan and other countries. In addition to conventional cigarette smoking, the number of heated tobacco product (HTP) users is increasing, especially in Japan, since 2014 when Philip Morris International first released an HTP, IQOS, in Japan and Italy.3 HTPs are electronic devices that heat tobacco leaves instead of combusting them to produce aerosols.4 One serious problem with HTP usage is that the exclusive or dual use of heated or e-cigarettes is misconstrued as an alternative to smoking cessation treatment,5 which can lead to nicotine dependence in cigarette smokers and hinder the promotion of smoking cessation.6 Since more than 20 million smokers in Japan use conventional cigarettes, HTPs or dual products,3 7 and there are up to 130 000 smoking-related deaths per year,8 smoking cessation is expected to significantly reduce the occurrence of the various diseases mentioned above, extend life expectancy, and ultimately reduce mortality rates and medical costs.8 9
In Japan, nicotine-dependent patients, including HTP users, are eligible for a 12-week standard smoking cessation treatment programme with clinic visits and an initial screening interview in which their exhaled carbon monoxide levels are checked.10 Moreover, some commercial telemedicine smoking cessation programmes are available for members of corporate health insurance societies (a public body that provides health insurance to corporation employees).11 However, biochemical check of smoking cessation status through exhaled carbon monoxide, which is currently measured at every visit in a standard smoking cessation programme, is not effective for HTP use.12 Moreover, it has not yet been assessed whether these smoking cessation programmes are effective to quit smoking for smokers who use HTPs since they were initially made for cigarette smokers.10 11
Here, we tested the outcomes of a telemedicine smoking cessation programme in terms of continuous smoking cessation among smokers who had used HTPs compared with those who used exclusively cigarettes.
Methods
Study overview
We conducted a retrospective study to assess the outcomes of the telemedicine smoking cessation programme provided by Linkage, Tokyo, Japan.13 Among participants in the programme, we compared the success rates of smoking cessation between smokers who had used conventional cigarettes and those who had used HTPs.
Participants
The present study was conducted between August 2018 and October 2020 and enrolled Japanese current smokers aged 20 years or older who applied for the telemedicine smoking cessation programme through the health insurance association. All the participants previously answered self-administered questionnaires on smoking status including their smoking period, cigarette and/or HTP use, smoking cessation history, reasons for this smoking cessation programme (eg, health consciousness, family or friend’s recommendations, financial burden, workplace smoking cessation policy and convenience of telemedicine), medical complications and treatments, marital status, job type and drinking habits. The participants were divided into three groups as (1) exclusively cigarette users, (2) exclusively HTP users, and (3) both cigarette and HTP users. We excluded smokers who had severe mental illness or severe physical comorbidities which required hospitalisation during the programme and those unavailable for the follow-up surveys. We included participants who agreed to the study’s privacy policy by providing an electronic informed consent form for health and medical data via a smartphone app (the D-CUBE telemedicine app) to be used in clinical analyses.
Outcomes
The primary outcomes were the participants’ continuous abstinence rates (CARs) from weeks 9 to 24 (CAR9–24) and weeks 9 to 52 (CAR9–52). The secondary outcomes were point abstinence rates that were defined as self-reported continuous abstinence from both cigarette and HTP smoking since latest follow-up survey at weeks 12 (equal to CAR from weeks 9 to 12 (CAR9–12)), 24, 36 and 52. Smoking cessation success was defined as quitting both cigarettes and HTPs and was confirmed with the structural interview performed by the telemedicine doctors at week 8 session and participants’ self-reports to the follow-up survey at weeks 12, 24, 36 and 52. CAR was defined as one or more consecutive weeks of smoking cessation successes since the telemedicine session finished at week 8. For example, if one participant answered that they had point abstinence at both weeks 12 and 24 via the follow-up survey, we considered that the participants achieved continuous abstinence from weeks 9 to 24 (CAR9–24). Participants who self-reported ‘relapse’ or did not respond to the follow-up survey (‘no reply’) were considered to have failed smoking cessation.
The Linkage telemedicine smoking cessation programme
The Linkage telemedicine smoking cessation programme is a 52-week (12-month) completely remote online programme through the D-CUBE telemedicine app made by Linkage (Tokyo, Japan) (figure 1). This programme consists of the 8-week (2-month) telemedicine programme provided by primary doctors and a 10-month follow-up period sending surveys and smoking cessation advice via the app at weeks 12, 24, 36 and 52. For the first 8 weeks, four telemedicine sessions were conducted in person through a videoconferencing system in the app, during which doctors evaluated participants’ physical and mental conditions, encouraged smoking cessation and offered advice on quitting smoking. Each telemedicine treatment time was about 15 min. Smoking cessation medications, such as varenicline or nicotine patches, were also prescribed by doctors’ discretion considering participants’ baseline characteristics and were directly sent to the participant’s home or office place. After completing the 8-week telemedicine programme, the D-CUBE app sent follow-up surveys and smoking cessation advice at weeks 12, 24, 36 and 52. Smoking cessation specialists created the smoking cessation encouragement and facilitation advice messages. All contents of the telemedicine smoking cessation programme referred to the standard procedure for smoking cessation treatment10 and the guideline for appropriate implementation of telemedicine in Japan.14
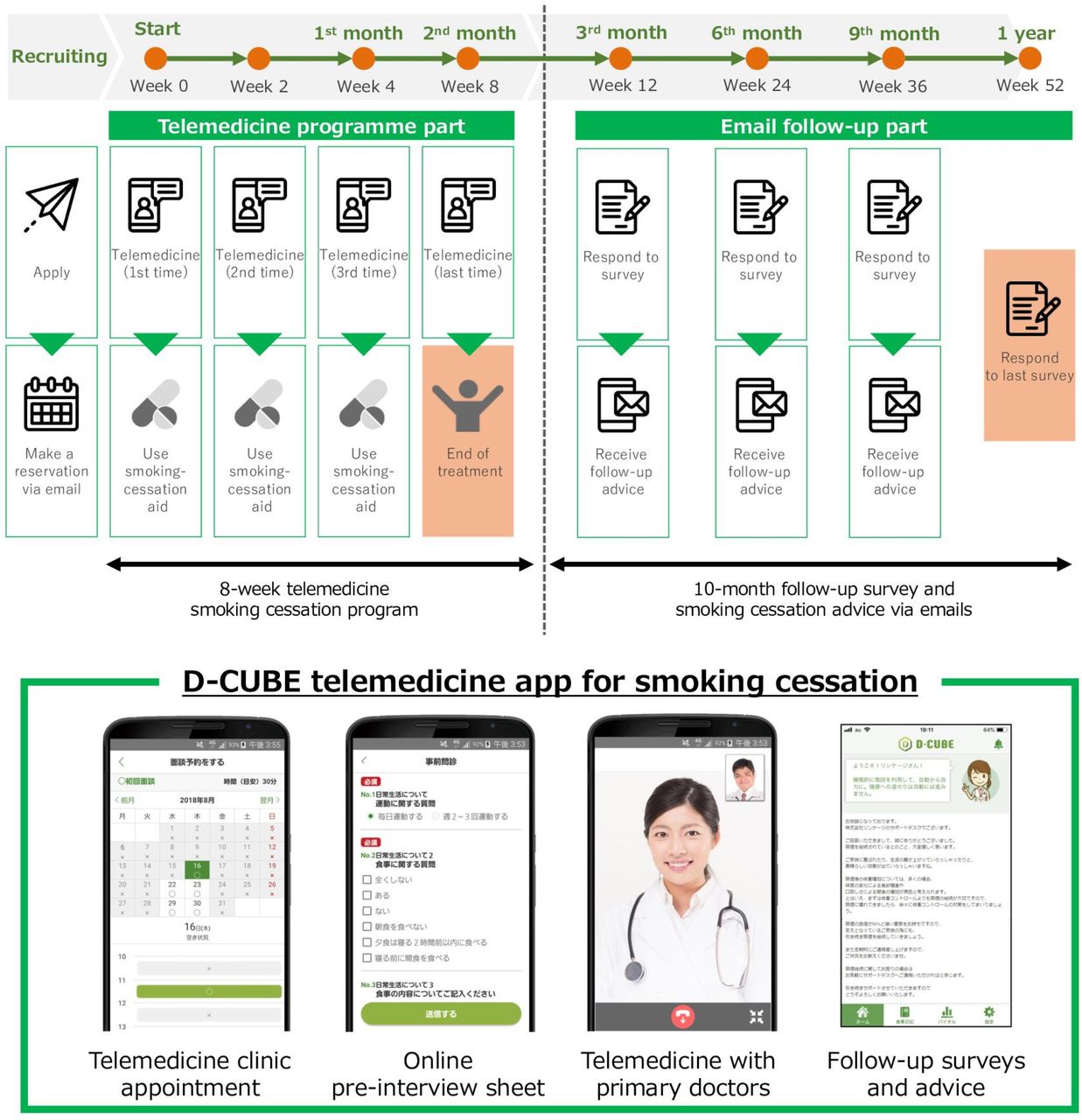
Overview of the Linkage telemedicine smoking cessation programme and the D-CUBE telemedicine app for smoking cessation. App images permitted by Linkage.
Data collection
We collected baseline information and follow-up surveys on each participant through the telemedicine app, including their age, sex, years spent smoking, number of cigarettes per day and tobacco dependence screening score using the Tobacco Dependence Screener (TDS).15
Statistical analysis
Continuous variables are presented as mean±SD or median (IQR) depending on distribution. Categorical variables are presented as numbers and percentages. A random forest imputation algorithm was used to deal with missing variables.16 For datasets with a mixture of categorical and continuous variables, random forest imputation enables imputation with less bias than other imputation methods, such as multiple imputations.16 We used all survey variables not missing more than 30% of values in each variable for the imputation. Random forest imputation was conducted using Python ver.3.8.3 with the MissForest package. We used Mann-Whitney U test for continuous variables or Fisher’s exact test for categorical variables to evaluate the baseline differences between exclusively cigarette group and HTP user group (exclusively HTP or dual use). In addition, we estimated inverse probability weights using generalised boosted models with 5000 regression trees.17 This model used the following parameters: age, sex, body mass index, years of smoking, past attempt for cessation, TDS score, regular alcohol intake, hypertension, diabetes mellitus, cardiovascular disease, mental disorders, varenicline use and nicotine patch use. We showed the standardised mean differences for each parameter to assess the balance of the three tobacco product groups. A maximum standardised difference of more than 0.2 indicated an imbalance among groups. After balancing the covariates among the tobacco product groups, we tested the differences in outcomes using logistic regression. Analyses for the inverse probability weighting method were conducted using R software ver.4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) with a twang package.17
Patient and public involvement
Patients and the public were not involved in the development of the research question, the design of this study, outcome measures, or the recruitment to and management of the study.
Results
We retrospectively analysed 750 participants of the Linkage telemedicine smoking cessation programme between August 2018 and October 2020. Of these, 17 participants were excluded due to unavailable smoking product usage data. Thus, we included 733 participants for further analyses (figure 2). Table 1 shows the baseline characteristics of the participants before inverse probability weighting. The mean age was 42.4±9.8 years, 94% were men and the median years spent smoking was 22. The types of smoking products included exclusively combustible cigarettes (52%), exclusively HTPs (31%), and dual use of combustible cigarettes and HTPs (16%). In terms of smoking cessation medication, varenicline was prescribed to 90% of programme participants. Compared with exclusively cigarette users, exclusively HTP users were younger, had smoked for fewer years and more attempts for smoking cessation. Additionally, dual users were younger and had smoked for fewer years compared with cigarette users. After inverse probability weighting, the maximum standardised differences among the tobacco product groups were all ≤0.15, indicating that the parameters were well balanced among the groups.
Baseline characteristics among exclusively cigarette smokers, exclusively heated tobacco product (HTP) users and dual product users

Study flow chart. HTP, heated tobacco product.
Overall success rates of the telemedicine smoking cessation programme
First, we evaluated the overall smoking cessation success rates of the telemedicine smoking cessation programme using all programme participants (figure 3). Point abstinence rates were 73.7% (95% CI 70% to 77%) at week 12 (equal to CAR9–12), 57.3% (95% CI 54% to 61%) at week 24, 50.3% (95% CI 47% to 54%) at week 36 and 54.4% (95% CI 51% to 58%) at week 52. Additionally, CAR9–24 and CAR9–52 were 55.8% (95% CI 52% to 59%) and 42.4% (95% CI 39% to 46%), respectively.

Point abstinence rates of telemedicine smoking cessation programme at weeks 12, 24, 36 and 52.
Smoking cessation success rates by smoking product types
Next, we assessed the smoking cessation success rates of the telemedicine smoking cessation programme by smoking product types standardised with inverse probability weights (table 2 and figure 4). For continuous abstinence, the exclusively HTP group had higher rates compared with the exclusively cigarette group in CAR9–24 (53.8% for cigarettes vs 67.0% for HTP; adjusted OR (aOR) 1.12; 95% CI 1.02 to 1.23; p=0.017) and in CAR9–52 (41.0% for cigarettes vs 50.9% for HTP; aOR 1.09; 95% CI 0.99 to 1.19; p=0.084). The point abstinence rates of the HTP group at week 24 were significantly greater than those of the cigarette group. Although the differences in abstinence rates between the groups were slightly attenuated at 52 weeks, the exclusively HTP group exhibited consistent higher abstinence rates over the exclusively cigarette group.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Continuous abstinence rates (CARs) from 9 to 12 weeks (CAR9–12) to 24 weeks (CAR9–24) and 52 weeks (CAR9–52) among exclusively cigarette smokers (cigarette), exclusively HTP (HTP) and dual users (dual). *P<0.05 compared with exclusively cigarette group. HTP, heated tobacco product.
Smoking cessation success rates of the telemedicine smoking cessation programme by smoking product types standardised with inverse probability weights
Conversely, the dual use of cigarettes and HTP group had lower CARs compared with the exclusively cigarette group in both CAR9–24 (53.8% vs 40.8% for dual use; aOR 0.85; 95% CI 0.76 to 0.95; p=0.004) and CAR9–52 (41.0% vs 30.8% for dual use; aOR 0.88; 95% CI 0.79 to 0.97; p=0.011) (table 2). The point abstinence rates of the dual use group at 24 weeks were worse than those of the cigarette group.
Discussion
This study, using inverse probability weighting, assessed whether the telemedicine smoking cessation programme was effective among nicotine-dependent adult patients using HTPs. We found that: (1) overall success rates of the telemedicine smoking cessation programme were 55.8% for CAR9–24 and 42.4% for CAR9–52; (2) exclusively HTP users had significantly higher smoking cessation success rates compared with the exclusively cigarette group in CAR9–24; and (3) dual users had significantly lower smoking cessation success rates compared with the exclusively cigarette group in CAR9–24 and CAR9–52. To our knowledge, this is the first study to assess the outcomes of a telemedicine smoking cessation programme for adult smokers using HTP compared with those using exclusively cigarettes.
This study provides several conclusions. First, overall smoking cessation success rates by the Linkage telemedicine smoking cessation programme were 55.8% for CAR9–24 (short term) and 42.4% for CAR9–52 (long term). Kato et al previously reported the effectiveness of the 6-month online smoking cessation programme in Japan for conventional cigarette smokers using online mentoring by trained smoking cessation experts, over-the-counter nicotine patches for medication and a unique smartphone app.11 They found that the CAR9–12 and CAR21–24 of patients who received the Ascure online program were 48.6% and 47.5%, respectively, which were almost consistent with our results. Additionally, the smoking abstinence rate was around 50% after completing the 12-week Japanese smoking cessation programme through outpatient services.18 19 Although the demographic characteristics and smoking cessation support medications were different, our telemedicine smoking cessation programme results might be reasonable compared with these data.
Second, smoking product types may affect the telemedicine smoking cessation success rates, especially among exclusively HTP users who had a higher smoking cessation success rate for up to 1 year than the exclusively cigarette group. Since HTPs have been promoted as a ‘switching’ product for quitting cigarette smoking by HTP manufacturers,6 20 HTP users may have considerable motivation to quit smoking. The lower quartile of smoking years in exclusively HTP users exceeded 15 years, indicating that most had smoked cigarettes before HTP emerged (~5 years), successfully quit cigarette smoking at some point and switched exclusively to HTPs. Additionally, Lau et al reported that exclusively HTP users had a lower nicotine dependence prevalence than daily exclusively cigarette smokers.7 This characteristic of HTP users could explain our results because the severity of nicotine dependence was strongly associated with smoking cessation success.21
Third, unlike exclusively HTP users, the smoking cessation success rates of the dual use group (using both cigarettes and HTPs) were significantly lower than those of exclusively cigarette users. This result might be reasonable because dual users needed to quit both cigarette smoking and HTPs, which could be more difficult than quitting individually. Moreover, this result was consistent with the report from Ryu et al that dual users of cigarettes and HTPs had a lower intention to quit smoking within 1 month than exclusively cigarette smokers.22 Furthermore, dual users might have a different clinical profile that could attenuate smoking cessation success compared with exclusively cigarette or exclusively HTP users. Our study indicated that dual users were younger and had shorter smoking duration than exclusively cigarette smokers. Since the age participants began smoking was one of the predictors of smoking cessation success,21 a younger age, more susceptible to a new tobacco product, might play a critical role in recurrence. However, we did not have data for dual users who quit cigarettes or HTPs during the study period. Since the definition of abstinence for dual users was more stringent than exclusively cigarette smokers or exclusively HTP users, abstinence rates for dual users could be different if we compared continuous ‘cigarette’ abstinence rates between exclusively cigarette smokers and dual users.
A strength of this study is that it is the first study to assess the outcomes of a telemedicine smoking cessation programme among HTP users and dual users compared with exclusively cigarette users. In the era of the coronavirus (COVID-19) pandemic, quitting smoking while minimising person-to-person contact could be essential to reduce the risk of COVID-19 infection and severe or critical COVID-19 symptom exacerbation.23 This study showed that the telemedicine smoking cessation programme may provide an option for both cigarette and HTP users to quit smoking regardless of social contact. The limitations of this study were as follows: (1) CARs were assessed by questionnaire-based self-reported abstinence, but not biochemically validated, which could misclassify smoking status or overestimate abstinence rates; (2) since our group previously reported that more than two-thirds of HTP or e-cigarette users simultaneously smoked cigarettes,3 some dual product users might mix in exclusively cigarette group or exclusively HTP group because they were grouped by the online questionnaire, which could influence the results; (3) we excluded participants unavailable for follow-up surveys in the 12 months, which could potentially affect adherence and success rates of the telemedicine smoking cessation programme.
In conclusion, exclusively HTP users achieved higher CARs over short-term and long-term periods than exclusively combustible tobacco users through the telemedicine smoking cessation programmes. Conversely, dual users had lower CARs in both short-term and long-term periods, which may be partly explained by the stringent abstinence definition in this study. A telemedicine smoking cessation programme might be a reasonable option for exclusively HTP users.
Data availability statement
Data are available upon reasonable request. The data that support the study findings are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was performed in compliance with the Declaration of Helsinki, Ethical Guidelines for Medical and Health Research Involving Human Subjects, and all other applicable laws and guidelines in Japan. The study protocol was approved by the Kanazawa University Institutional Review Board (2020-206 (3573)). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank all the participants and medical staff for this study.
References
Footnotes
Twitter @akihiro_nomuryn
Contributors AN, TIshizawa and TT contributed to the concept of this study. YM and TIshizawa acquired the data. AN, TIkeda, TF, CT and TT analysed the data and drafted the manuscript. All authors contributed to the interpretation of the results and critical review of the draft manuscript. All authors agree to the final version of the submitted manuscript. AN is a guaranter of this study.
Funding This study was supported by a KAKEN Grant-in-Aid for Scientific Research (A) (21H04856).
Competing interests AN received consulting fees from CureApp and is the co-founder of CureApp Institute. TIshizawa is the chief medical officer and a shareholder of Linkage. TT received consulting fees from Linkage.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.