Article Text

Abstract
Background There is broad consensus that disclosure of harmful medical errors is vital to improve safety and is ethically required. Although most physicians-in-training are taught ethics, there have been no empirical studies on whether ethical reasoning is related to disclosure. We examined whether scores on a test of ethical reasoning were associated with greater willingness to disclose errors.
Methods We conducted a cross-sectional survey of house officers in internal medicine at Johns Hopkins Hospital. Ethical reasoning was assessed using the Defining Issues Test, V.2 (DIT-2). Higher DIT-2 scores are associated with more sophisticated ethical reasoning, and scores tend to improve after formal ethical training. Respondents were then given a medical error scenario with multiple scripted disclosure options. Ethical reasoning scores were compared for different levels of disclosure.
Results A total of 29 out of 127 medicine residents completed the survey (response rate=22.8%). The 41% of residents who would explicitly tell a patient that, ‘an error happened’ had significantly higher DIT-2 scores than those who would not (51.1 vs 31.6, p<0.01). Higher DIT-2 scores were found in the 62% of residents who would give the most detail about the error (44.8 vs 31.2, p=0.04) and in the 71% of residents who would take personal responsibility (43.5 vs 27.9, p=0.03).
Conclusions Ethical reasoning scores were associated with acknowledging an error, providing more detailed explanations and taking personal responsibility. The low response rate may limit generalisability. Nevertheless, taken together with prior studies showing that ethical reasoning can be taught and measured, our findings suggest that ethical training may help to improve disclosure of medical errors.
- Graduate Medical Education
- Incident Reporting
- Medical Education
- Social Sciences
- Communication
Statistics from Altmetric.com
Introduction
Open communication with patients about harmful medical errors is an ethical obligation, and is important for error reduction.1 Despite this, universal disclosure of harmful errors remains elusive.2–4 Deciding to speak up about a medical error—especially one's own—is difficult to do.
A variety of factors influence the decision to disclose an error. For one, professional obligations stipulate respect for patient autonomy—which includes a duty to give patients information that they might reasonably want to know, and that might help them to make fully informed decisions about their care.5 System factors influencing error disclosure include aspects of medical culture, such as an ideal of error-free performance,6 ,7 and what Leape and Berwick described as the ‘well-entrenched hierarchical authority structure and diffuse accountability’ of medicine.2 Finally, despite some data suggesting that open communication is associated with lower malpractice claims rates,8 fear of litigation is an important impediment to error disclosure.9
Personal morality and ethical reasoning also may influence the decision to disclose. The Defining Issues Test (DIT) is a tool designed to measure individual variation in ethical reasoning.10 This test has been used for over 30 years in medicine; higher DIT, V.2 (DIT-2) scores have been associated with a variety of noteworthy outcomes including improved ratings of doctor–patient interactions by third-party observers,11 as well as lower rates of malpractice claims.12 Medical student scores generally improve in response to classes on medical ethics,13 as well as to small group case discussions.14 Some data also suggest that ethical reasoning may decline or stagnate during medical training—although the question of which aspects of medical training might be responsible remains open.15–17
Confirmation of a relationship between ethical reasoning and disclosure might suggest a new rationale for ethics training in medicine. We therefore undertook a cross-sectional study of medicine house officers to examine the relationship of scores on the DIT to decisions about disclosure of a hypothetical error to patients.
We chose to study medical residents for three reasons. First, they represent a group of physicians with a fairly homogeneous level of training and experience. Second, the decision to disclose an error may be particularly challenging for junior physicians, who have been shown in previous studies to be less likely than practicing physicians to admit their mistakes.4 Third, the educational nature of residency programmes provides an opportunity for future educational interventions even if an association between ethical reasoning and disclosure is found.
Methods
Population
The study population were members of the Johns Hopkins Hospital medical house staff who were recruited by email and in person between July and October of 2011.
Survey instrument
The survey included two elements: (1) The DIT-2 to measure ethical reasoning and (2) a standardised error scenario to measure disclosure attitudes. The Johns Hopkins School of Medicine IRB approved the survey instrument. Informed consent was obtained at the time of survey administration.
Defining issues test, V.2
The DIT-2 is an instrument developed to measure differences in ethical reasoning.10 It is an updated version of the original DIT, which has been in use since the 1970s. The test consists of a series of ethical dilemmas. We used an abbreviated version that included three dilemmas: (1) a father with a starving family contemplates stealing from the warehouse of a rich man hoarding food, (2) a newspaper reporter must decide whether to report a damaging story about a political candidate and (3) a school board member must decide whether to hold a contentious and dangerous meeting. The shortened version was approved by the developers of the DIT-2. (Personal Communication, Steven Thoma, June 2011).
Each dilemma is followed by a series of 10 issues that may be relevant in resolving that dilemma. In the first dilemma, two of the 10 issues are: ‘Would stealing [the food] bring about more total good for everybody concerned or wouldn't it?’ and ‘Does the rich man deserve to be robbed for being so greedy?’ After stating how they would resolve the dilemma, respondents must rate and then rank the relative importance of each issue in making their decision.
The issues fall into a hierarchy of three categories or schema: Personal Interest, Maintain Norms and Postconventional Reasoning. Personal Interest comprises issues relating to individual cost and benefit. Maintain Norms consists of issues relating to authority, hierarchy, rules and conventions. The Postconventional Reasoning is characterised by ‘primacy of moral criteria, appeal to an ideal, shareable ideals and full reciprocity’.13 The Postconventional Reasoning is considered the most mature form of thinking about moral dilemmas.18
Each respondent is given a percentage score called the Postconventional Reasoning score, (P-score) which represents the relative weight given to issues in the Postconventional schema. The highest P-scores are typically seen in populations with the most training in ethics. Political scientists, or moral philosophy PhD students, have been shown to have P-scores in the mid 60s. At the other end of the spectrum, junior high school students typically have P-scores in high teens—indicating that they tend to rate highly issues in the Personal Interest and Maintaining Norms schema. Most existing studies of physicians have shown P-scores ranging from the high 30s to low 50s.19
The P-score has evidence for construct validity including (1) differentiation between known groups based on age and educational attainment, (2) correlation with cognitive capacity measures, (3) significant linkage to prosocial behaviours, (4) significant linkage to political and social beliefs. There is also evidence for responsiveness to change including (1) measurement of individual longitudinal gains and (2) sensitivity to moral education interventions.10 The test demonstrates high test-retest reliability. The updated DIT-2 is shorter in length and has more contemporary scenarios, but has been validated against the original DIT and against independent criteria such as age, educational differences and political views. Cronbach's α was acceptable (0.81).
Completed responses to the DIT-2 were scored by the Center for Ethical Development at the University of Alabama.
Error scenario
Following the DIT-2 portion of the survey, respondents were given a story about a hypothetical error scenario. In the vignette, they are told to imagine that they recently started a patient on a new drug with a well known side effect of hyperkalemia. Two weeks later, the patient begins to feel palpitations, is taken to the emergency department and must undergo an emergency cardioversion. They are then told that on reviewing the case they see an overlooked lab result showing a dangerous increase in potassium. Had they noticed the lab result earlier they could potentially have avoided the life-threatening arrhythmia. Following this story, subjects are given definitions of ‘adverse event’ and ‘error’. They then must answer a series of seven questions. The first two questions asked respondents how responsible they felt for the error and how likely they would be to disclose. The remaining five addressed particular aspects of disclosure (stating that ‘an error happened’, taking responsibility, giving full details, apologising, providing a plan). Each had three scripted response options: full disclosure, partial disclosure and no disclosure (see online supplementary appendix A for text of questions and scripted response options).
The story, questions and scripted responses were based on a survey instrument developed and validated by Gallagher and colleagues.20–22 Both the scenario and questions were used with permission of the developers.
The survey was pilot tested with residents at Johns Hopkins Hospital and University of Pennsylvania prior to use in the study. Those who took part in the pilot were not asked to take part in the full study.
Recruitment
The project was presented at house staff meetings in August and October 2011 with email announcements sent before and after the meetings. Subjects were told that the team was conducting research on error disclosure, and how house officers think through difficult social situations. At the meeting, they were given paper copies of the survey, which could be filled out or returned in preaddressed, stamped envelopes. Additionally, all medicine residents were emailed a link to an online version of the survey, which they could complete at their convenience.
Data analysis
We hypothesized that those residents choosing the more complete disclosure for each question would have higher mean P-scores than those who chose the partial disclosure options; and that those more cognisant of complex ethical issues would be more likely to disclose. For each of seven disclosure questions we therefore compared the mean Postconventional Reasoning scores of those who opted for the highest level of disclosure with those who did not. For questions 1 and 2, there were four possible answers which were dichotomised as: extremely responsible versus the rest (1) and definitely disclose versus the rest (2) respectively. In questions 3–7 there were three possible answers each of which have been dichotomised in a similar fashion.
The decision to group responses in this manner was a response to the overall distribution of answers: For each of the seven items there were very few respondents (often 1 or 0) who chose the minimal disclosure options. The majority of respondents were therefore clustered within the two higher disclosure groups of full or partial disclosure. Given the very small numbers in these low disclosure groups, an ordinal regression analysis would not be statistically useful. When combined with the overall low response rate we felt that the most meaningful comparison would be achieved by analysing the difference in Postconventional Reasoning scores between those who chose full disclosure and those who did not.
We evaluated for statistical significant differences in ethical reasoning between these groups using a two-sample t test. A p value of <0.05 was considered statistically significant. Stata/SE 10.0 for Macintosh. (StataCorp 2007, Stata Statistical Software: Release 10, College Station, Texas, USA: StataCorp LP)
Results
Out of a total of 127 medicine residents at Hopkins, the final study sample included 29 residents (response rate=22.8%). Characteristics and P scores of the 29 residents who completed the full survey are shown in table 1.
Respondent characteristics
The mean Postconventional Reasoning score (P-score) for all respondents was 39.7 (SD=17.4, range 3.3–73.3). There were borderline significant trends for women to have had higher P-scores than men ( p=0.09), and for third years to have higher mean P-scores than first or second year residents (p=0.08).
P-score relation to error disclosure
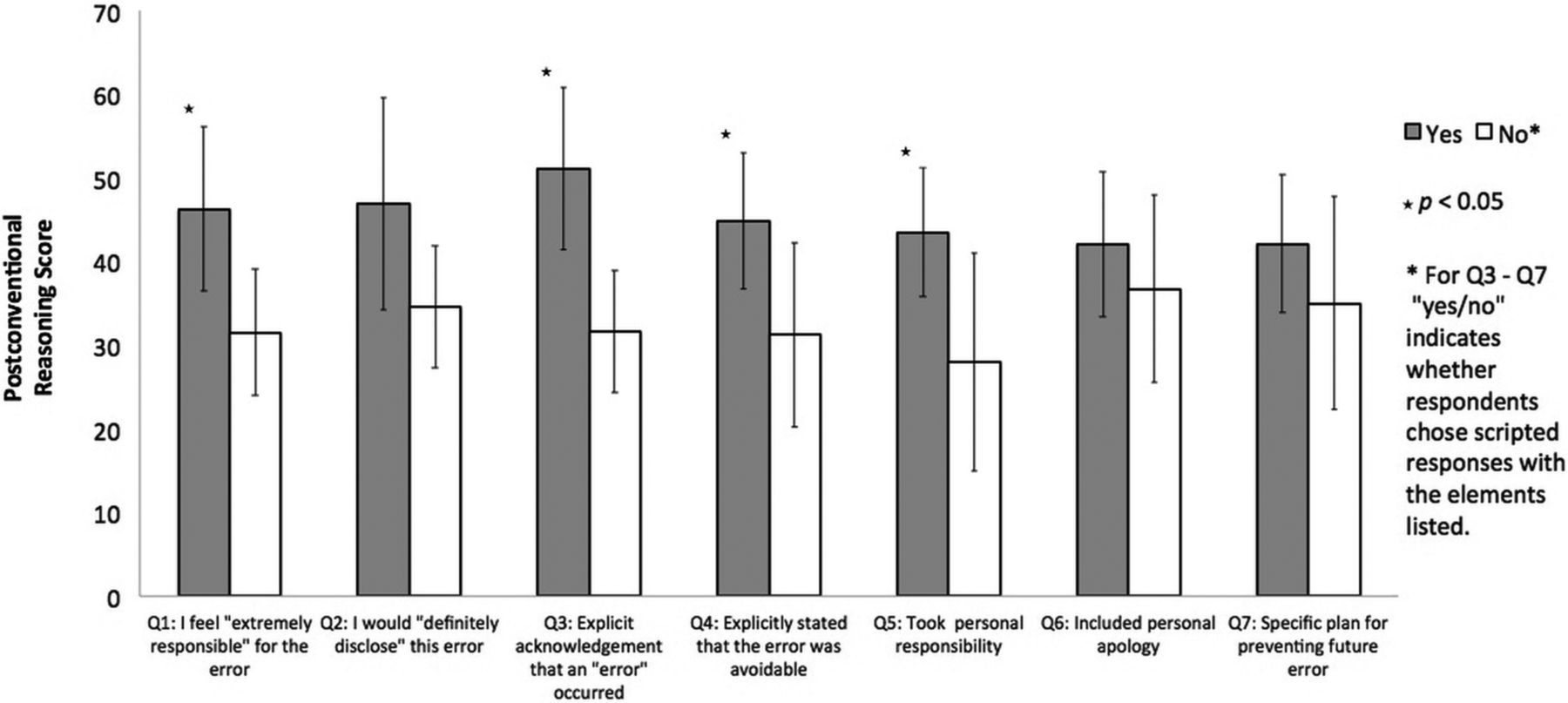
The 55% of respondents who stated that they felt ‘extremely responsible’ for the error had significantly higher P-scores than those who did not (46.2 vs 31.5, p=0.02) (table 2). The 41% of respondents who stated that they would ‘definitely disclose’ also had a trend towards higher P-scores than those who did not, but this was of borderline statistical significance (46.9 vs 34.5, p=0.06).
Postconventional Reasoning scores by disclosure preference*
In comparing the choice of scripted response options, the 41% of residents whose chosen statements included explicit acknowledgment that ‘an error happened and we did not notice that the new medicine had caused your potassium to become too high’ had higher P-scores than those who merely mentioned that the new medicine caused the high potassium (51.1 vs 31.6, p<0.01). The 62% who chose the statement with the most possible details about the error, why it happened, and that it was avoidable, had significantly higher P-scores than those who chose the more general statement that ‘we did not realise your potassium had gotten high until it was too late’ (44.8 vs 31.2, p=0.04). The 71% of respondents who chose the statement taking explicit personal responsibility: ‘I did not remember to check the results…’ also had significantly higher P-scores than those who did not (43.5 vs 27.9, p=0.03).
The 55% of residents who chose an explicit apology, ‘I am so sorry you were harmed by this error’ did not have significantly higher P-scores than those who offered only a general statement of regret or no apology at all (42.1 vs 36.1, p=0.41). Similarly, the 71% who provided a detailed plan for preventing the error in the future did not have significantly higher P-scores than those who offered no plan or only a vague and non-specific plan (42.1 vs 35.0, p=0.30). These results are summarised in table 2 and figure 1.
{kind=link}
Postconventional Reasoning scores by level of disclosure.
We estimated the internal consistency of the putative scale comprising the seven disclosure questions. We assigned a score of 1 to the highest disclosure choice in each question and a score of 2, 3 or 4 for the lower disclosure options (see online supplementary appendix A for scripted response text). Using these scores, the Cronbach's α for the scale was 0.79.
Discussion
In this study of ethical reasoning and error disclosure, residents with higher ethical reasoning scores were more likely to state that they would definitely disclose an error, and reported feeling greater personal responsibility for errors. In their selection of scripted responses, they chose to provide greater levels of details to patients, chose statements expressing more personal responsibility, and more readily used the word ‘error’ in their explanations.
Providing patients with a specific plan and explicit apology were not associated with higher scores of ethical reasoning—suggesting that these specific steps in the disclosure process may be more strongly influenced by other, non-ethical factors such as training, experience, notions of propriety and cultural mores.
Taken together, our results support an association between more sophisticated, principled ethical reasoning and important aspects of open, honest communication. We can conclude that aspects of disclosure such as explicitly admitting that an ‘error’ occurred, both feeling and expressing personal responsibility, and providing patients with the most possible details about an error may be more strongly related to personal ethics than others. Professional ethics clearly support being open about harmful errors. This is the first study we are aware of which has specifically focused on personal morality and its relationship with error disclosure.
While much has been written on the subject of systemic barriers to disclosure,1 ,2 ,4 our results suggests that personal morality plays an important role. Because our study was cross-sectional, we cannot conclude that improvements in moral reasoning will lead to improved disclosure. Nevertheless, our results can be taken within the context of existing research using the DIT-2, which shows that medical education can both positively and negatively affect how individuals think about ethical dilemmas,15–17 ,23 and that certain educational experiences may be better than others in terms of raising ethical reasoning scores of trainees.13–14 ,16 Taken together with this, our finding of an association between higher DIT-2 scores and more open disclosure suggests that ethical training may lead to more open error communication and improvements in patient safety.
Limitations
Our study had several limitations. First, our response rate was low. We only obtained usable surveys from 23% of the total medicine house staff at Johns Hopkins Hospital. A larger sample size would provide more precise results and would give us more confidence in the generalisability of the results. This low response rate may have been at least partially due to the fact that the survey was quite long, and fairly complex. An indication of this is the fact that seven residents started, but did not complete the survey.
Third, it is uncertain whether self-reported error disclosure corresponds with real-life practice. Several important impediments to disclosure mentioned above—for instance, worry for reputation, fear of litigation—are not readily reproducible in a written survey. However, even if the impediments to disclosure are greater in practice, respondents who opted for more complete disclosure in a survey might still be expected to practice more open disclosure in real life.
Further research with longitudinal follow-up is needed to test whether an educational intervention teaching ethical reasoning to residents can improve error disclosure in practice. If this study were to be expanded to a larger sample size we would modify our statistical model using a logistic or ordinal regression with disclosure as the dependent variable and reasoning score as the independent variable. In addition to answering the question of whether higher Postconventional Reasoning scores result in higher levels of disclosure, this would also allow for the consideration of other variables which may explain differences in disclosure (eg, age, sex and years of experiences).
Conclusion
There is broad consensus that problems in communications create and perpetuate safety hazards. It is also widely agreed that full disclosure of adverse events should be the norm in medicine.1 It is therefore vital to encourage policies that support disclosure of adverse events. If, as our results suggest, ethical reasoning can lead to more open communication, then emphasising ethics in medical training may be one avenue to do just that. Our results suggest a possible new tool for improving safety communication, while also recognising the importance of ethics and ethical training in shaping the conversations that are vital for safe and open medical care.
Acknowledgments
We acknowledge Dr Margaret Moon of the Berman Institute for Bioethics for reading and commenting on drafts, and Dr Joe Carrese and Dr Gail Geller for thoughtful and incisive support through the bioethics scholarly concentrations programme at Johns Hopkins School of Medicine.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Contributors AC conceived of the study objectives, designed data collection tools, recruited study subjects, organised and monitored data collection, wrote the statistical analysis plan, cleaned and analysed the data, and drafted and revised the paper. He is guarantor. AW designed the data collection tools, wrote the statistical analysis plan, monitored data collection and revised the draft paper. LB recruited study subjects, organised and monitored data collection and revised the draft paper.
-
Funding Research was funded in part by the Johns Hopkins University School of Medicine Office of Student Affairs Summer Research Award.
-
Competing interests None.
-
Ethics approval Johns Hopkins School of Medicine IRB.
-
Provenance and peer review Not commissioned; externally peer reviewed.