Article Text

Abstract
Objectives Compare gender disparities in ST-elevation myocardial infarction (STEMI) regarding first medical contact (FMC) and prehospital delay times and explore factors associated with prehospital delay in men and women separately.
Design Cross-sectional study based on medical records and a validated questionnaire. Eligible patients were enrolled within 24 hours after admittance to hospital.
Setting Patients were included from November 2012 to January 2014 from five Swedish hospitals with catheterisation facilities 24/7.
Participants 340 men and 109 women aged between 31 and 95 years completed the survey.
Main outcome measures FMC were divided into five possible contacts: primary healthcare centre by phone or directly, national advisory nurse by phone, emergency medical services (EMS) and emergency room directly. Two parts of prehospital delay times were studied: time from symptom onset to FMC and time from symptom onset to diagnostic ECG.
Results Women more often called an advisory nurse as FMC (28% vs 18%, p=0.02). They had a longer delay until FMC, 90 (IQR 39–221) vs 66 (28–161) min, p=0.04 and until ECG, 146 (68–316) vs 103 (61–221) min, p=0.03. Men went to hospital because of believing they were stricken by an MI to a higher extent than women did (25% vs 15%, p=0.04) and were more often recommended to call EMS by bystanders (38% vs 22%, p<0.01). Hesitating about going to hospital and experiencing pain in the stomach/back/shoulders were factors associated with longer delays in women. Believing the symptoms would disappear or interpreting them as nothing serious were corresponding factors in men. In both genders bystanders acting by contacting EMS explained shorter prehospital delays.
Conclusions In STEMI, women differed from men in FMC and they had longer delays. This was partly due to atypical symptoms and a longer decision time. Bystanders acted more promptly when men than when women fell ill. Public knowledge of MI symptoms, and how to act properly, still seems insufficient.
- adult cardiology
- coronary heart disease
- myocardial infarction
- ischaemic heart disease
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The present study is, to the best of our knowledge, the first published study of gender disparities and first medical contact in ST-elevation myocardial infarction (STEMI), using self-reported data covering symptoms, multiple time point measurements and actions, and self-reported reasons for delay and interpretation of symptoms as explanatory factors for prehospital delay.
With the use of wide inclusion criteria, approximately 1/10 of the hospitalised Swedish patients with STEMI during the inclusion period filled in the questionnaire within 24 hours of admittance, making the results generalisable and with limited risk of recall bias.
Regarding the observational study design, we can only report associations rather than causations, and there may be factors associated with prehospital delay times not covered by the questionnaire, such as health literacy and deeper knowledge about MI.
Patients not being pain free and haemodynamically stable were excluded from participation, but we do not have any demographic data on this cohort, making it impossible to compare those participating in the study with those excluded.
We have not collected data on all traditional risk factor variables (such as history of hypercholesterolaemia) which can be seen as a limitation.
Introduction
Myocardial infarction (MI) mortality has decreased substantially during the last decades in the Western world, because of more active prevention and better treatment.1 Still, outcomes in ST-elevation MI (STEMI) differ between the genders, with approximately two times as high in-hospital mortality in women,2 3 who receive reperfusion therapy less often than men.2 4 In STEMI, timely administration of reperfusion therapy is critical for improving survival.5 6 During the last decades, focus has mainly been on shortening system delay times where a clear association between longer delay and worse prognosis has been found.5 Consequently, STEMI guidelines strongly recommend that the diagnosis is made already in the prehospital setting.7 In Sweden, an ECG is taken by the Emergency Medical Services (EMS) paramedics in patients with symptoms indicating an evolving MI. The ECG is then transferred to the nearest hospital where the cardiologist/internist on call judges if the patient has a probable STEMI or not. Thus, in patients calling EMS, the diagnosis of STEMI can be made well in advance before admission to hospital and the patient can be directed straight to the catheterisation laboratory or could be given prehospital fibrinolytics.8
Less focus has been on the patient delay in the prehospital phase, which has been proven difficult to influence.9 10 The prehospital delay times have been unchanged over the past decades,11–13 but it is unknown whether the delay is due to difficulty with symptom recognition, symptom interpretation or decisions related to care seeking (including the mode of transportation to the hospital). In order to distinguish patient delay from system delay times, it has been suggested to also include the time point of first medical contact (FMC) in the analysis of prehospital delay times.14 However, previous studies have mostly focused on total prehospital delay times.11 12 15 Since patients with STEMI do not always call EMS as their FMC, studying the different phases of prehospital delay times as well as choice of FMC is imperative. Female gender has been found to be associated with prehospital delay times according to several studies,12 16–19 but measurements have been inconsistent20 and data on gender disparities on FMC in STEMI are very sparse. Consequently, further studies are needed to better understand the relation between gender and care-seeking behaviour in a STEMI population.
Aim of the study
We aimed to compare gender disparities in STEMI regarding: (1) FMC, (2) prehospital delay times from symptom onset to FMC as well as from symptom onset to diagnostic ECG and (3) factors associated with symptom onset to FMC in men and women separately.
Method
This Swedish multicentre study (SymTime) has been previously described.21 In short, it has a descriptive and comparative cross-sectional design of self-reported data. A previously validated self-administered questionnaire developed and tested in a Swedish chest pain population was used,22 with some minor changes and clarifications. The questionnaire covers 35 items including (1) baseline characteristics, (2) symptoms, (3) course of events including multiple time point measurements and (4) description of transport mode. We enrolled participants from five Swedish hospitals with diverged geographical locations, all with catheterisation facilities and primary percutaneous coronary intervention (PCI) enabled 24/7. Data were collected in the cardiac care unit in each participating hospital from November 2012 to January 2014. Eligible patients were planned to be consecutively included within 24 hours after admittance and were invited to answer the questionnaire after the primary PCI/reperfusion therapy had been given. Inclusion criteria were: (1) a confirmed STEMI diagnosis, (2) ability to fill in the questionnaire and(3) willingness to participate. Patients were pain free and haemodynamically stable when they were asked to participate and fill in the questionnaire. The staff nurse simultaneously obtained clinical data such as information on diagnosis, FMC, important time point measurements (eg, ECG and FMC) and comorbidities from the patients as well as from the medical records.
In this study, two parts of prehospital delay times were studied: (1) the interval between time of symptom onset to FMC and (2) the interval from symptom onset to diagnostic ECG. FMC was defined as the time point when contacting any healthcare personnel either by phone or in person and was divided into five possible contacts: (1) the primary healthcare centre (PHC) by phone, (2) the PHC directly, (3) the Swedish Healthcare Direct (SHD) by phone (ie, advisory nurses), (4) the EMS by phone or (5) the emergency room (ER) directly. All patients chose any of these five ways of contacting the Swedish healthcare system.
Ethical aspects
The study complied with the Declaration of Helsinki.23 Informed consent was obtained from all included patients.
Patient and public involvement
We originally involved patients in the development and the revision of the questionnaire used in this study when testing the user-friendliness and content in the modified questionnaire. The knowledge gain from this project will be disseminated to the public at different meeting and seminars at local patient organisations in Sweden. Participants interesting in the results have been advised to contact the study coordinator for information.
Statistical analysis
We used frequencies and proportions to describe the history of patients’ characteristics, the sociodemographic, clinical and contextual variables and their FMC. Categorical variables were reported by numbers and percentages and groups were compared with the use of the X2 test. Continuous variables were reported as mean±SD or as medians with IQR, and gender comparisons were made with the two-tailed Student’s t-test or the Mann-Whitney U test depending on if the variable was normally distributed or not. Multiple linear regression analyses were performed in men and women separately in order to sort out relevant predictors of patient delay. The time variable had to be log transformed in order to be normally distributed. Background characteristics, clinical presentation, context when falling ill, thoughts and actions as well as reactions from bystanders were included in five blocks in order to analyse the relevance of each block in terms of R2 change. Residual plots were run, and no violations of assumptions were noted. Included variables were chosen through literature research and/or deemed to be important by the research group. There were few missing values in the data collection— regarding the most important outcome measurements there were no (symptoms) or minor (FMC, 0.9% and delay from symptom onset until FMC, 3.8%) missing values. All tests were two tailed and a p value of less than 0.05 was deemed as indicating a statistically significant difference between compared groups. All statistical analyses were performed using IBM SPSS Statistics V.23.0 (SPSS) for Windows.
Results
Background characteristics and clinical presentation
In total, 449 patients with STEMI were included. Women were 5 years older than men, with lower educational status and more often living on their own. Women had a higher prevalence of hypertension as well as diabetes mellitus (table 1). Among chief complaints, chest pain/discomfort was prevalent in 92% of men compared with 73% of women, p<0.001. Pain in the throat/neck, back and/or shoulder was two times as common in women as in men, as well as a feeling of fear. Nausea was prevalent in half of the women compared with one-third of the men. There was no gender difference in pain intensity (table 2).
Baseline and clinical characteristics
Clinical presentation
Thoughts, actions and context when falling ill
When falling ill in STEMI, women were more often together with their children, relatives or friends, whereas men were more often together with colleagues. There was no gender difference in being alone or being at home at the time. Self-medication with aspirin was as common in both genders as well as nitroglycerine, whereas women took painkillers almost two times as often as men (27% vs 15%, p<0.01). The first person to talk to about the symptoms was the partner, which was the case in more than half of both men and women. Women more often than men informed their children first of all about their symptoms, whereas men more often than women first talked to friends or relatives. More than one-third of the women compared with one-fourth of the men spoke to the SHD before they went to the hospital (28% vs 18%, p=0.02) and less than one-fifth of both men and women talked to their PHC, with no difference between the genders. To a great extent both genders had heard of angioplasty or clot dissolving as treatment for MI.
The most common reason why patients with STEMI went to the hospital was severe symptoms, with no difference between the genders. Men went to hospital because of believing they were struck by an MI to a higher extent compared with women (25% vs 15%, p=0.04). There was neither any gender difference in hesitating going to the hospital, nor in reasons why hesitating. The most common reason for why hesitating was a belief the symptoms would disappear, with no difference between the genders (table 3).
Thoughts, actions and context when falling ill with STEMI
Reactions from bystanders
Men were more often recommended to call 112 by bystanders (38% vs 22%, p<0.01). Women more often had bystanders calling SHD (36% vs 25%, p=0.03), but also more often did not tell anyone about their symptoms (7% vs 2%, p=0.02) (table 4).
Reactions from bystanders when a person fell ill
Delay times and FMC
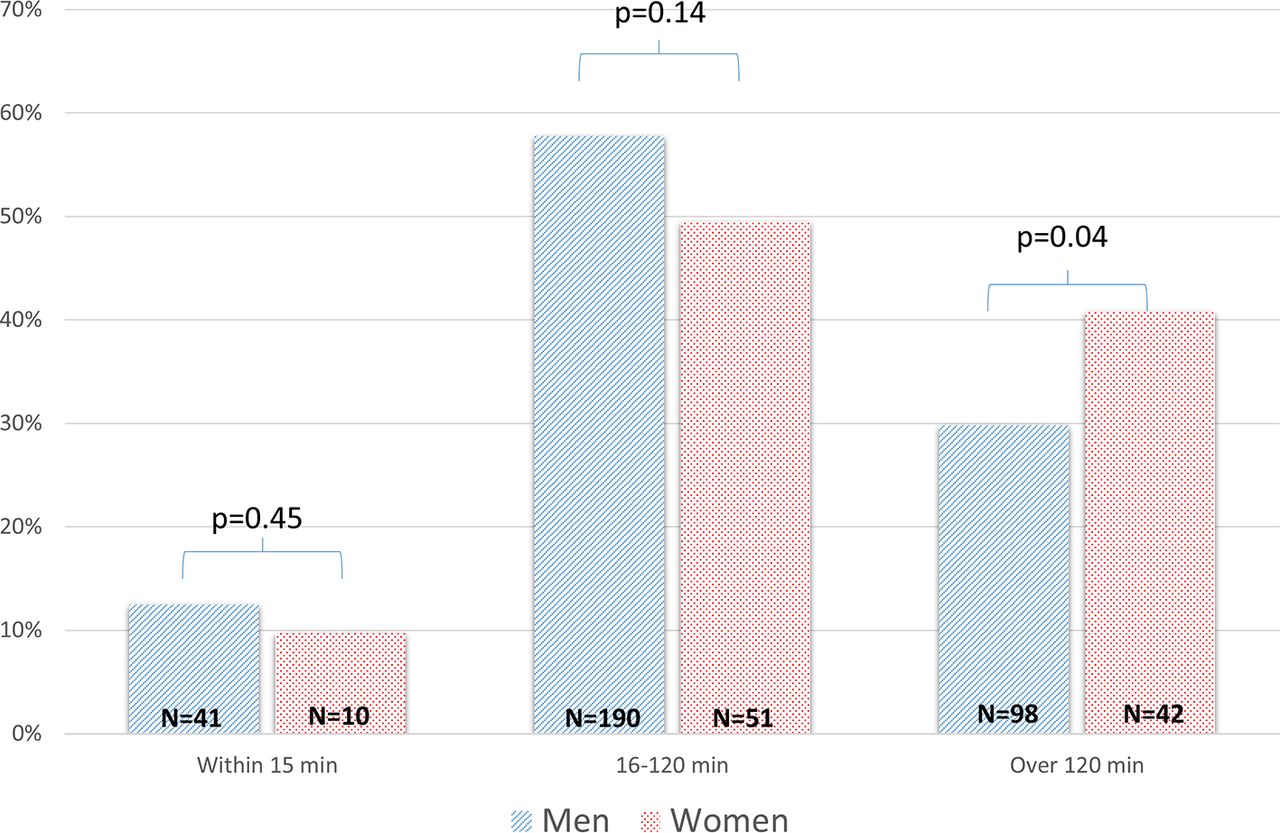
In the total study population, the median patient delay from symptom onset to FMC was 70 min (IQR 30–178) and to diagnostic ECG 110 min (IQR 64–238). The system delay from FMC to diagnostic ECG was 27 min (IQR 15–50). Women waited in median 90 min (IQR 39–221) before taking their FMC compared with 66 min (IQR 28–161) in men, p=0.04. EMS was the most common FMC used by approximately half of the patients regardless of sex, but women more often contacted SHD as FMC compared with men, 28% vs 18% (p=0.02) (figure 1). After being urged to contact the EMS by the general practitioner (GP) or the advisory nurse at the SHD, 83% of patients finally arrived at the hospital by ambulance while the remainder transported themselves directly to the ER. System delay time in form of FMC to diagnostic ECG did not differ between the genders, (25 (15–49) min in men vs 33 (15-61) min in women, p=0.09). Altogether, women had a longer delay from symptom onset to diagnostic ECG (146 (68–316) min in women, vs 103 (61–221) min in men p=0.03). Divided in subgroups on short, medium and long delay, women more often had a long delay compared with men, both from symptom onset to FMC, and from symptom onset to diagnostic ECG (figures 2–4).

First medical contact in men and women with ST-elevation myocardial infarction.
Delay times from symptom onset to first medical contact.

Delay times from first medical contact until diagnosis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Delay times from symptom onset to diagnosis.
Factors associated with delay in men and women
In women, sociodemographic, contextual, cognitive, behavioural and clinical factors included in the survey explained 53% of the variance of prehospital delay times from symptom onset to FMC compared with 26% in men (ie, the R2 for the complete model, men and women studied separately). In both genders, the clinical presentation explained most of the delay from symptom onset to FMC, followed by thoughts and actions when falling ill. In women hesitating to go to the hospital, stomach pain and pain in the back/shoulders were the variables most strongly associated with increased delay, while cold sweat and bystanders calling—or recommending calling—EMS were the variables most strongly associated with short delay. In men, believing the symptoms would disappear or interpreting the symptoms as nothing serious had the strongest association with increased delay, whereas bystanders calling EMS was the variable most strongly associated with reduced delay (table 5).
Predictions of patient delay times in men and women separately
Discussion
The main findings of the present study are the far longer delay times in women versus men among Swedish patients with STEMI, from symptom onset to FMC of 26 min and from symptom onset to diagnostic ECG of 43 min. This was due to primarily three factors: (1) more atypical symptoms in women and (2) a longer decision time in women and (3) a gender difference in choice of FMC, where women more often than men called the national SHD service number for advice.
Prehospital delay times account for the largest proportion of the total ischaemic time9 but have remained virtually unchanged over the last decades.12 This is important since only patients with STEMI with a short prehospital delay (<90 min) have a long-term benefit of shorter system delay to reperfusion.24 Although interventions aimed at shortening prehospital delay times have been discouraging,9 10 a more recent report from Denmark on patients with STEMI calling EMS services have found a temporal trend of decrease in prehospital delay times (symptom-onset-to-calling EMS) from 101 to 85 min between year 2003 and 2009. This was after introduction of primary PCI to all patients with STEMI, which the authors claim could have had potentially positive effects on public awareness.25 Still, further efforts are needed in order to increase public awareness and in the recent scientific statements from the American Heart Association, the authors emphasise improved methods to disseminate information about women’s risks, symptoms, and behaviours and necessary responses to symptoms of acute MI.19
Few studies have focused on delays to FMC in STEMI. The majority of previous studies have defined prehospital delay time as the time interval from symptom onset to hospital arrival, without separating the patient from the system delay, that is, before and after FMC.11 12 15 26 27 However, in a recent registry-based study, Bugiardini et al 28 report time lapses from symptom onset to calls to EMS or a GP’s office and found no significant time differences among men and women (50 min vs 60 min) while we did find a significant delay between genders (66 min delay in men vs 90 min in women). Still, the time lapses are not completely comparable since our FMC, beyond calls to the EMS and the GP’s office, also included in-office visits to the GP, a phone contact with an advisory nurse or a direct contact with the ER. Studies on gender disparities in prehospital delay times have shown inconsistent results and have limitations such as using restricted patient samples,26 or relying primarily on information from medical records26 or registries not specifically designed to study delay.11 26 27 Finally, many studies have included mixed patients with MI not restricting the inclusion to STEMI.11 22 26 In the current study focusing on patient delay from symptom onset to FMC and from symptom onset to diagnosis of STEMI, women delayed 1.5 hours until FMC compared with approximately 1 hour in men. In the total study population, the median delay from symptom onset to FMC of 70 min, and to diagnostic ECG of 110 min, is substantially better than reported in studies from other American and European countries18 28 29 but still exceeding the recommendations advised by guidelines by several minutes.30 A study based on the French eMUST registry, including patients with STEMI who have been taken care of by special mobile intensive care units, found in accordance with our data that women waited longer before calling the EMS. They also found a very similar delay until calling as we did to any FMC (78 min in women vs 54 min in men, p<0.0001).18 In the present study, more than 40% of the women compared with 30% of the men waited over 2 hours before seeking medical attention. Reducing patient-caused delay has a great potential to improve the outcomes of patients with STEMI, given that many deaths occur early after symptom onset.
It is important to analyse care-seeking behaviour in different regions of the world, as differences in medical insurance and healthcare systems do play a part as well as cultural factors and gender equality reflecting differences in awareness, interpretation and actions on MI symptoms. In Sweden, counted as one of the most gender equal countries in the world, with complete healthcare coverage for all citizens, only small gender disparities were found in context, thoughts and actions when falling ill. Men more often first talked about their symptoms with a spouse, relative or friend whereas women more often talked with their child/children. This probably reflects the fact that women are older than men when falling ill with STEMI, and thus more often living on their own because of being widowed.31 Older studies from other geographical regions have found that ‘not wanting to trouble anyone’ is a factor associated with prolonged delay in women, but not in men.32 In the present study, no difference was found as regards worries of disturbing or drawing attention.
Women and men differed in FMC in the current study. EMS was the FMC in only half of the patients (53% of men and 46% of women) and instead as many as one in three of the women and one in five of the men called SHD as the FMC despite suffering from a very serious disease. In Sweden, SHD—a joint service number—was launched in 2003 and is staffed by advisory nurses 24/7 in order to answer questions, determine the need for further care and provide advice and/or contact with other healthcare providers. SHD has become a very important way of contacting the healthcare system and gets around 500 000 calls every month. The use of SHD in STEMI is worrying as we have shown in a previous study that patients turning to SHD as FMC had a 38 min longer delay from symptom onset until first ECG compared with patients calling EMS.21 The reluctance to call EMS may be explained by several factors such as misinterpretation of symptoms, as well as women’s lack of perceived potential risk for acute coronary syndrome (ACS).33 The women in our study were less educated than the men and in the multivariable analysis, this variable tended to be associated with longer prehospital delay times in women (p=0.06). This could be attributed to low socioeconomic status and lack of ACS knowledge in women.19 Anyhow, it is reassuring that although far too few patients, both men and women chose EMS as FMC, 83% of patients finally arrived at the hospital by ambulance while the remainder transported themselves directly to the ER. We have previously shown that this was the case regardless of if the patient chose calling/visiting PHC, calling EMS or calling SHD as their FMC.21
A large gender disparity in chest pain prevalence—the most well-recognised symptom of MI presentation in society—was found. The fact that women are less likely to experience chest pain has also been noted in two recent scientific statements from the American Heart Association19 31 and is in accordance with a previous large registry study in a mixed MI population.34 At the same time less well-known MI symptoms such as pain in the neck, throat, back or shoulders or nausea were more than two times as common in women as in men. Previous studies have found that MI symptoms looked on as typical such as chest pain or pain in the left arm are most important for a correct attribution to the heart35 and that the prognosis is worse in patients with MI with atypical symptoms.34 In accordance, men more often than women responded that believing that they had an MI was the reason for going to the hospital in the current study. The importance of the clinical presentation for patient delay was shown in the multivariable regression with the presence of symptoms such as pain in the back, shoulders or stomach being associated with longer delay in women but not in men. Symptoms that are perceived as threatening have been described associated with shorter prehospital delay times.36 Accordingly, in the present study, cold sweat was associated with shorter delay in women and anguish/fear was associated with shorter delay in men.
Finally, bystanders can be crucial in obtaining appropriate care. In the present study, bystanders calling EMS was one of the strongest factors associated with short delay although a gender difference in bystanders’ responses to described symptoms depending on the patient’s gender was found—whereas men more often had bystanders recommending contact with the EMS, women more often had bystanders calling SHD for advice. A previous study has found that relatives are more dissatisfied with the information given by the hospital staff compared with the patient.37 This illustrates the need to involve the next of kin in secondary prevention education and care-seeking behaviour, as a well-informed bystander can help diminish the patients’ decision time.
Conclusion
In conclusion, this study showed that women differ from men regarding several self-reported symptoms, thoughts, actions and prehospital delay times—and partly also in reasons as to why delaying. Based on our findings, women may have different educational needs compared with men, which has to be considered when educating the public about how to recognise and act when an evolving MI emerges.
Acknowledgments
The authors hereby acknowledge all participating hospitals and their staff who included patients on a daily basis, making this project possible. We especially acknowledge Elisabeth Logander, a highly skilled research nurse at Linköping University Hospital, who supported the study group throughout the project.
References
Footnotes
Contributors SSL and IT contributed to the study planning, design, preparation, validation of the slightly modified questionnaire and data analysis. KHÄ, ME and SSL contributed to the data collection. KHÄ, ME, R-MI, SSL and IT contributed to the manuscript preparation and approved the final version of the manuscript.
Funding This work was supported by the Medical Research Council of Southeast Sweden (FORSS), the County Council of Östergötland and the County Council of Norrbotten.
Competing interests None declared.
Patient consent Not required.
Ethics approval Permission for the study was obtained from the regional Ethical Review Board, Linköping, Sweden (D-nr 2012/201–31)
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.