Article Text

Abstract
Introduction Data supports that motor skills are an underlying mechanism that influence physical activity along with perceived motor and physical competence, but the relationship between motor skills and physical activity during the early years is unclear. The goal of this study, Promoting Activity and Trajectories of Health (PATH) for Children, is to examine and compare the immediate (pre-test to post-test) and sustained (3-year follow-up) effect of an intervention on motor performance, physical activity and perceived physical competence to a control condition (ie, standard practice) in preschool-age children.
Methods and analysis The PATH study is a two-cohort, randomised cluster clinical trial. 300 children between the ages of >3.5 to 5 years of age will be randomised to the motor skill intervention (n=153) or control (n=147) condition. Each assessment involves a measure of motor skill performance; product and process, seven consecutive days of physical activity monitoring and perceived physical competence. These measures will be assessed before and after the intervention (pre-test to post-test) and then each academic year across 3 years, grades kindergarten, first grade and second grade (3-year follow-up). To assess the clustered longitudinal effect of the intervention on outcome measures, random-effects models (eg, mixed model regression, growth curve modelling and structural equation modelling) will be used. The PATH study addresses gaps in paediatric exercise science research. Findings hold the potential to help shape public health and educational policies and interventions that support healthy development and active living during the early years.
Ethics and dissemination Ethical approval for this study was obtained through the Health Sciences and Behavioral Sciences Institutional Review Board, University of Michigan (HUM00133319). The PATH study is funded by the National Institutes of Health. Findings will be disseminated via print, online media, dissemination events and practitioner and/or research journals.
Trial registration number NHLBI ClinicalTrials.gov Identifier, NCT03189862. Registered 17 August 2017, https://clinicaltrials.gov/ct2/show/NCT03189862
- community child health
- public health
- preventive medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study will include a strong investigative team with a vast amount of experience in intervention-based research, motor development and physical activity measurement in paediatric populations.
This study will use robust objective measures for motor performance, perceived physical and motor competence and physical activity.
This randomised clinical trial will capitalise on an evidence-based intervention (ie, CHAMP (Children’s Health Activity Motor Program)) that is theoretically-grounded in Achievement Goal Theory.
Limitations to this clinical trial include the inability to examine the effect of weight status or body mass index, inability to understand the children’s movement experiences after the intervention and established limitations associated with accelerometry.
Introduction
Childhood obesity has been a public health concern for the past 30 years and engaging in adequate physical activity is a way to counter the effects of childhood obesity.1 Approximately 24 per cent of US children and youth meet physical activity recommendations2 3 of at least 60 min of daily moderate-to-vigorous physical activity (MVPA).4 The percentage of children and youth meeting physical activity recommendations is even lower in ethnic minorities5 and appears to be related to generational status.6 The early childhood years mark a critical time in development.7 During this period, children establish healthy habits and behaviours to support growth and development across their lifespan. The American Academy of Pediatrics developed additional recommendations to support healthy development during early childhood (ages 3 to 5) that include engagement in gross motor activities.8 These recommendations align with specific physical activity guidelines for preschool-age children and include 3 hours of physical activity each day.9 Unfortunately, only 50% of preschool-age children may meet this recommendation.10
MVPA or ‘health-enhancing’ physical activity is one critical component that promotes children’s overall health and well-being. MVPA supports healthy weight maintenance, cardiometabolic health and mental health in children.11 Promoting the development of adequate physical activity habits from an early age has proven to be an arduous endeavour. Additionally, few physical activity clinical trials have been conducted in preschool settings. Some of these trials include Colorado LEAP,12 Hip Hop to Health Jr.13 14 and SHAPES,15 but their impact on MVPA are mixed.16 For example, the 2005 Hip Hop to Health Jr. trial did not see any improvements in the intervention participants’ total day physical activity, but in the 2011 trial significant increases were seen in minutes of total day MVPA when 1 day equated to 8 hours of wear time.13 14 At post-intervention, preschoolers in the intervention school engaged in about 7.5 more minutes of MVPA per day compared with preschoolers in the control schools.
The 2005 Hip Hop trial used parental reports to measure the physical activity while the 2011 trial used actigraphy. The differences in physical activity methodology used to assess physical activity could have contributed to some of the differences seen in the physical activity outcome. The 2005 trial also used trained early childhood educators to teach the physical activity intervention programme. The 2011 trial integrated the intervention into the preschool curriculum and was delivered by the classroom teachers. A commonality seen among Hip Hop for Health Jr. and the other clinical trials is the lack of focus on gross motor skill development, which is suggested to be a contributing antecedent for developing positive trajectories of physical activity behaviours.17
Based on the literature, an approach to address physical inactivity in young children is to intervene on an underlying factor that influences physical activity from a developmental perspective—the development of motor skills. Since 2008, there has been a growing interest in the intersection of physical activity and motor skill development as they are both precursors to promote children’s overall health and well-being. The acquisition of adequate competence in a variety of motor skills like locomotor, ball skills and stability skills are learnt behaviours that facilitate the promotion of health-enhancing physical activity across childhood.18–21 For example, a child, teenager or adult is less likely to engage in a recreational or sport-related softball game that could help them meet their daily physical activity recommendation if they do not possess proficient motor skills in catching, throwing, running or striking.
Motor competence is a global term that has been used to describe motor constructs. Specifically, motor competence refers to the ability to demonstrate a proficient and optimum level of motor skill performance in a variety of motor skills, along with the underlying mechanisms that affect movement patterns.22–25 Motor skills, motor performance, motor proficiency, motor coordination, and so on, are terms used to reference these movement patterns. Previous studies have linked motor competence to multiple aspects of health-related fitness and weight status.17 Even in industrialised or developed countries, children from low-income, disadvantaged/under-resourced environments and ethnic-minority populations demonstrate lower motor skill competence compared with their counterparts.26–30 There is a misconception that all children naturally develop motor skills. Still, evidence indicates sufficient opportunities that include developmentally appropriate instruction, practice and reinforcement are needed to promote adequate motor competence levels in children.28 31–41
Another important construct that contributes to motor skills and physical activity is competence in our physical and motor abilities.42 Competence relates to our beliefs, attributions and affect and aligns with the feeling that we experience when engaging in a behaviour.43 Competence evolves from Achievement Goal Theory and supports the theoretical base for the intervention used in this clinical trial (the intervention will be discussed in the Methods).44 Children’s perceptions of competence are critical for promoting positive and sustained physical activity across childhood and into adolescence.42 45 46 Perceived physical competence is the more global construct of self-efficacy which determines one's overall confidence in their abilities on physical tasks,47 while perceived motor competence is a psychological construct that refers to a person’s awareness and belief in their capability to perform both gross and fine motor tasks.48–51 Both perceptions appear to be important and have an effect on physical activity and may help in understanding physical activity patterns. Throughout this paper, perceived physical competence will be used to encompass both the perceived physical and motor competence.
Barnett et al used Harter and Pike’s perceived competence subscale to demonstrate the strong mediating role of perceived motor competence to actual motor competence and physical activity over the early childhood years.45 46 Barnett’s work also aligns with Stodden et al’s conceptual paper suggesting as children age, the relationship is stronger between perceived motor competence and actual motor competence.52 This conceptual model argues that the relationship is reciprocal and is driven by the development of children’s ability to perceive and understand that they are competent in various movement contexts. In turn, their perceived motor competence will lead to success and enjoyment in a variety of activities. It is essential to understand how perceived physical competence, physical activity and actual motor competence interact and influence one another across childhood. Only a few studies have examined these variables longitudinally and all were examined in samples outside of the USA (ie, Australia,18 Portugal19 and Denmark53). Additionally, causality has not yet been investigated regarding the role of actual motor competence, perceived physical competence and physical activity in a randomised control trial (RCT).
This proposed RCT will examine the mediating role of the perceived physical competence on actual motor competence and physical activity over time. Preschool interventions that focus on physical activity (eg, aims to increase the number of minutes of physical activity as the treatment modality) to address physical inactivity have resulted in mixed findings regarding physical activity promotion (ie, Colorado LEAP,12 Hip Hop for Health Jr.,13 14 SHAPES,15 MAGIC,54 Youp’là Bouge,55 PAKT56 Walk57). There have also been studies that used an educator-led physical activity and motor skills intervention that were effective.58 59 Even though research supports the positive effect of motor skills on physical activity, motor skills are often not the focus of the treatment modality in physical activity intervention studies. Bellows et al found that the intervention dose did improve preschoolers’ motor skills performance but did not have a positive effect on reducing body mass index or increasing physical activity.60 This proposed clinical trial, Promoting Activity and Trajectories of Health (PATH) for Children, expands on previous work and addresses the following aims and hypotheses:
Aim 1: To examine and compare the immediate (pre-test to post-test) effect of a motor skill intervention, CHAMP (Children’s Health Activity Motor Program), on motor performance, physical activity and perceived physical competence to a control condition (ie, standard practice) in preschool-age children.
Hypothesis 1: Children in the motor skill intervention, compared with control condition, will demonstrate higher levels of motor performance, physical activity and perceived physical competence at post-intervention.
Aim 2: To examine and compare the sustained (3-year follow-up) effect of a motor skill intervention, CHAMP, on motor performance, physical activity and perceived physical competence to a control condition (ie, standard practice) in preschool-age children.
Hypothesis 2: Children in the motor skill intervention, compared with control condition, will demonstrate higher levels of motor performance, physical activity and perceived physical competence over the 3-year follow-up period.
Aim 3: To test the immediate and long-term mediating effect of perceived physical competence on the relationship between motor performance and physical activity among preschool-age children.
Hypothesis 3a: Perceived physical competence will not mediate the relationship between motor performance and physical activity at baseline. Perceived physical competence will mediate the relationship between motor performance and physical activity immediately post-intervention and across the 3-year follow-up period.
Hypothesis 3b: Group differences will be present in the mediation between the treatment and control condition immediately post-intervention and across the 3-year follow-up period.
Methods and analysis
Study Design. The PATH Study will consist of a two-cohort, randomised cluster clinical trial with 16 to 19 weeks of intervention during preschool and a 3-year follow-up for each cohort. To reduce contamination between intervention and control classrooms, recess periods will be monitored to ensure that no motor instruction takes place. Teachers in the intervention classrooms will be instructed not to discuss research activities with other classrooms and teachers will not be present for CHAMP instruction. However, it is impossible to control for treatment children’s behaviours and actions with control children. Follow-up assessments will be conducted at the start and end of each subsequent academic year in kindergarten, first grade and second grade. The Institutional Review Board at the University of Michigan approved the study (HUM00133319) and the RCT is registered in the Clinical Trials Registry. The school administration (school principals/directors) agreed to participate in this study and the Principal Investigator (PI) obtained approval to conduct the study by the District’s Board of Education. Informed written consent will be obtained from children’s parent/guardian(s) along with verbal assent from each child. The reporting of this research follows the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT61;). Figure 1 depicts the PATH study timeline in the SPIRIT diagram.

StandardProtocol Items: Recommendations for Interventional Trials diagram for the schedule of enrolment, interventions and assessments. X1=Cohort 1; X2=Cohort 2 **See detailed description of collected variables in main protocol. - Motor performance will be evaluated using the TGMD-3 (process measures) and product measures of motor skills. - Physical Activity will be measured for one full week (ie, 5 weekdays and 2 weekend days) with accelerometers. - Perceived Physical and Motor Competence will be assessed with physical and motor competence subscales – Harter and Pike pictorial scale of competence and social acceptance and the digital-scale of perceived motor competence. CHAMP, Children’s Health Activity Motor Program; TGMD-3, Test of Gross Motor Development-third edition.
Study Context. This study will take place in three federally funded early learning centres located in the Midwestern US. The centres will provide free quality preschool programmes to children who come from a household with an income that is at least 100% below the federal poverty level. These centres were chosen due to the number of enrolled preschool-age children that could potentially serve as participants and because the centres were located on the same campus as the elementary schools, where the preschoolers would likely enrol for their formative education following preschool. Classrooms (n=32) will be randomly assigned to receive either the motor skill intervention or the control condition (ie, outdoor recess) by computer-generated random numbers. Researchers will not have any decision or control in the assignment of students to specific classrooms, as this will be determined by each individual school. Each classroom teacher's name will be placed in a sealed envelope and will be randomly selected to either a treatment or control in an alternating sequence by a person external to the investigative team.
Participants and protocol
Inclusion/exclusion Criteria
Preschoolers ≥3.5 years will be eligible to enrol and participate in this study. Children will be considered ineligible if any of the following apply: exhibit characteristics or are diagnosed with syndromes or diseases that would affect physical activity participation, or have a previous diagnosis of any major illness, developmental and/or physical disability since birth. If a child that is deemed ineligible to participate in the study due to an above condition has parental consent, they will be able to participate in the treatment but no data will be collected on these individuals.
Recruitment
After receiving human subjects approval, parent(s)/guardian(s) will receive an information letter and consent letter from the PI notifying them of the PATH study at the beginning of the year, preschool school welcome letter. The letter will give a brief description of the study along with a statement from the schools indicating that parent(s)/guardian(s) are not obligated to participate. Parents will be instructed to return the consent letter to the teacher in a sealed envelope that will later be retrieved. All parents/guardians who return a consent form, regardless of whether they agree to participate in the PATH study, will receive a one-time cash incentive of US$5.00. A copy of the consent letter will be provided to parents who agree to participate in the study. In addition to parental consent, verbal assent will be obtained from each preschooler. Data for the longitudinal study will be collected during kindergarten, first grade and second grade and parental re-consent will only occur if there are changes to the protocol, but child re-assent will be obtained at each assessment period (eg, baseline, post-test, and so on). Parents will receive reminder letters for each upcoming PATH assessment and a developmental report of their child’s anthropometric measurements, motor performance and physical activity engagement every year. Each school and the school district will be provided with aggregated data of the findings. Figure 1 provides a representation of the population N and the breakdown of participants into treatment and control. A model consent form can be found as a online supplementary file to this protocol.
Supplemental material
Patient and public Involvement
The PATH study will be done without patient/participant involvement. Patients/participants will not be invited to comment on the study design and will not be consulted to develop patient/participant relevant outcomes or interpret the results. Patients/participants will not be invited to contribute to the writing or editing of this document for readability or accuracy. The PATH study is a low-to-minor risk research study. A safety monitoring committee (SMC) will be used to provide oversight for the project to ensure the safety of the participants, monitor the study and oversee the clinical trial. Specifically, the SMC’s role is to serve in a consultative capacity to inform Co-PIs, the IRB and, ultimately, the National Institutes of Health regarding the conduct of the trial.
Children’s Health Activity Motor Program
Intervention. The original work for this intervention was conceptualised and initially tested the effect on object control skills and perceived competence (physical and motor) for the PI’s dissertation work at Ohio State University. The PI continued to investigate the effect of this intervention on various outcome measures from 2007 until present.28 31 33–35 37 39–41 62–65 The programme was officially named the Children’s Health Activity Motor Program (CHAMP) in 2015. CHAMP is a theoretically-grounded intervention and preliminary work supports that the intervention enhances motor skill performance,28 33–35 37 39 40 64 65 physical activity,41 62 65 perceived physical competence31 33 35 and maintains delay of gratification37 in preschool-age and/or school-age children. Preliminary data indicate that CHAMP is effective in preschool-age and school-age children.28 31 33–35 37 39–41 62–65
Theoretical Underpinnings. Achievement Goal Theory originates from educational psychology and focusses on the motivation to learn66 since goals of learning are the key factors that influence the level of intrinsic motivation. Achievement Goal Theory refers to the beliefs, attributions and affect that contribute to one’s behaviours and represents how they approach, engage and respond to various activities.44 67 Individuals can take either a mastery- (task-) orientation or performance- (ego-) orientation.67 68 Performance- (ego-) individuals focus on ensuring that their performance is successful and superior to others while mastery- (task-) individuals engage in learning for the sake of learning and are less threatened by failure. Mastery- (task-) oriented individuals often have higher intrinsic motivation.44 67
The CHAMP creates a learning environment that supports a mastery approach to learning motor skills. CHAMP will adhere to six TARGET structures (task, authority, recognition, grouping, evaluation and time; table 1) and provide children the opportunity to self-navigate, a developmentally appropriate movement environment, with instruction and lessons to accommodate a wide range of skills and abilities.68 69 This approach will encourage the children to learn and develop new skills, increase their level of competence and achieve a sense of mastery based on their perceptions. Three theoretical tenets of Achievement Goal Theory are crucial to CHAMP. The tenets are; (1) a positive, reciprocal relationship between effort and personal progress, (2) learners’ self-selection of tasks (ie, practice) and (3) the instructional climate.
Description of the TARGET structures and CHAMP strategies
From an instructional standpoint, CHAMP will incorporate pedagogical strategies from physical education and principles from motor learning/development research. These strategies and principles include the use of developmentally appropriate cue words to promote motor skill acquisition, effective modelling and demonstration, timely feedback (ie, knowledge of performance and knowledge of results), scaling of the learning equipment, appropriately designed tasks and task presentation, practice variability and repetitive cycling of motor skills and tasks. Newell’s constraints model will be used to change the developmental components of a motor task by manipulating environment and task constraints within each motor skill lesson to ‘encourage’ or ‘discourage’ specific movement action.70 These physical education pedagogical and motor learning principles will be used to scaffold—move the learners progressively toward a better understanding of motor skills and promote motor skills learning.
Intervention delivery and training
The CHAMP motor skill intervention will have an intervention dose of 2155 min. Cohort 1 will receive the intervention 3 days per week for 45 min across 19 weeks (ie, 16 weeks of the CHAMP intervention plus 3 weeks in between for winter and spring breaks) and Cohort 2 will receive the intervention 4 days per week for 35 min across 20 weeks (ie, 17 weeks of the CHAMP intervention plus 3 weeks for winter and spring breaks). This difference in the number of weeks and weekly minutes in each cohort is due to schedule changes in the academic calendar. Cohort 1 CHAMP session consists of three parts: (a) 3 to 5 min of introductory activity, (b) 35 to 38 min of motor skill instruction and practice and (c) 3 to 5 min motor skill closure activity and review. Cohort 2 CHAMP session consists of: (a) 3 to 5 min of introductory activity, (b) 23 to 25 min of motor skill instruction and practice and (c) 3 to 5 min motor skill closure activity and review. CHAMP will be implemented by two motor development researchers that are PhD students. The lead instructor has 6 years of experience implementing the CHAMP intervention. The second instructor is a certified K-12 Physical Education teacher and has a Master’s degree in Health Education. The PI will serve as a substitute intervention instructor when needed. Additional research personnel (one to two) will assist with other managerial tasks for the intervention (eg, ensure that the cameras are recording, record attendance, equipment set-up and breakdown, collecting and returning of children to classroom, and so on).
All instructors and personnel are PhD students in the motor development programme or currently employed within the research laboratory and have a knowledge base of the motor skill intervention. All research personnel will undergo training before the start of and during the intervention. The training will include: (a) a theoretical understanding of CHAMP that entails Achievement Goal Theory and mastery climates, (b) reviews of previous recorded instructional sessions of the CHAMP intervention, (c) sessions on how to use cues and prompts to promote skill learning, (d) practice implementing CHAMP followed by a reflection session, (e) lessons on how to transition and pace the intervention session to ensure safety and (f) giving feedback on motor performance.
Intervention fidelity
Intervention fidelity refers to the extent to which the intervention is implemented as intended and the following strategies will be used. The movement instructors will be provided with detailed intervention material including: the intervention protocol that specifies the amount of content for each session (eg, dosage), intervention adherence checklists, skill instruction/cue words for each motor skill taught and detailed lesson plans. Furthermore, the instructors will meet at the end of each intervention week to discuss the various aspects of the intervention (eg, the progression of skill development in the children, additional strategies to support learning and to ensure proper implementation of the intervention). Fidelity checks on the TARGET structures and instruction will be completed at every session to ensure that the intervention adheres to the protocol. Checks will record the start and finish time for each section of the lesson, observe if both verbal and physical feedback are provided, confirm that the students receive clear instruction that incorporates a demonstration and cue words, ensure that the lessons follow the plan and each session ends with a review and note any modifications. All sessions will be digitally recorded to serve as a record of the intervention and enable any session to be reviewed if needed. If there are any concerns, the instructors and PI will meet for a discussion and additional training.
Control condition
The control condition will be the early learning centres’ standard practice for what is quantified as their motor programmes for accreditation purposes: outdoor recess/free play. The outdoor recess/free play programme will be implemented according to the existing procedures within the centres. Each class will receive two, 30 to 45 min outdoor recess (free play) sessions each day. For PATH participants, the control group will receive two, 30 to 45 min per day outdoor sessions, whereas the treatment (CHAMP) group will receive one, 30 to 45 min outdoor session per day after their nap, as the morning recess session will be replaced with the motor skill intervention. The centres’ outdoor programmes consist of outdoor free play activities on a large playground area with a variety of play structures (swings, slides, ladders) that will promote physical activity, gross movement skills and body management skills. No planned instruction or activities will be provided to the preschoolers during outdoor recess. Classroom teachers and research personnel will confirm that the daily outdoor recess sessions are completed with a check-off sheet.
Measures
Data will be collected by a trained research team. Outcome measures will be collected for all participants (Cohort 1 and 2) in both the treatment and control groups at baseline (ie, before the start of the intervention), post-test (ie, the week following the conclusion of the intervention) and follow-up during kindergarten, first grade and second grade . Baseline measures will occur in September/October and post-tests will occur in late April/May. On average, it should take each child about three to four, 25 to 30 min sessions across 3 days to complete all the assessments. All perceived physical competence data will be collected before students complete the motor skill assessments. Motor skills will be assessed in small groups of four to five children. Typically, the order of completion will be as follows: Session 1: anthropometrics (eg, height, weight, and so on.) and perceived physical competence; Session 2 and 3: motor skills—process and product measures; Session 4: make-ups. Physical activity will be assessed for 7 days after the other measures have been collected and will not occur during a week where the intervention is provided. Follow-up assessments will be conducted at the start and end of each academic year for kindergarten, first grade and second grade (ie, follow-ups will be noted as follows: T3/T4 for kindergarten, T5/T6 for grade 1, T7/T8 for grade 2). Figure 1 illustrates the PATH study timeline for the collection of outcome measures.
Primary outcomes
Motor performance
Motor performance will be evaluated using process and product measures of motor skills that are assessed concurrently. Assessing both types of measures of motor performance increases its predictive validity for PA.
Process measures
The Test of Gross Motor Development-third edition (TGMD-3) will assess process measures of motor skills.71 72 The TGMD-3 is a valid and reliable criterion-based assessment that measures fundamental motor skill competence in children aged 3 to 10 years. It consists of six locomotor (run, jump, gallop, slide, hop and skip) and seven ball skills (throw, catch, dribble, underhand throw, kick, one-handed forearm strike and two-handed strike off a tee). The TGMD-3 is a valid and reliable scale. It has excellent internal consistency overall (α=0.96, total; α=0.92, locomotor; α=0.95, ball skills73) and for children between the ages of 3 to 5 years (α=0.98, total; α=0.96–0.97, locomotor; α=0.97, ball skills73). The assessment also has excellent test-retest reliability for the total TGMD-3 (intraclass correlation (ICC)=0.97) as well as for locomotor (ICC=0.97) and ball skills subscales (ICC=0.9573).
The TGMD-3 will be completed according to the test manual and procedures. Raw scores for the two TGMD-3 subscales, locomotor (0 to 46) and ball skills (0 to 54) will be summed to derive the total score (0 to 100) that will be used for data analyses. The TGMD-3 assessments will be digitally recorded and coded by a motor development expert who will serve as an external consultant to the project and will be blind to the randomisation. Intra-rater and inter-rater reliability was previously established between the consultant/coder and the two members of the research team. All coders underwent a 2-hour training prior to coding any data. Then all coders reviewed a small subset of children prior to the onset of coding the full sample. Inter-rater reliability was determined using a two-way mixed ICC with absolute agreement. Results support that inter-rater reliability was high overall (ICC=0.99) as well as for both locomotor (ICC=0.98) and ball skills subscales (ICC=0.95). Reliability will be established on a randomly selected 30% of the assessments and will be completed every year.
Product measures
Product scores are developmentally valid and sensitive discriminators of motor performance.74–76 Ball velocities will be measured with a radar gun (Stalker Inc, Richardson, Texas, USA). A tennis ball (6.54 to 6.86 cm diameter) and a playground ball (8.5 inch diameter) will be thrown and kicked, respectively, with maximum effort from 20 feet for five trials. Jump distance (cm) will be measured for the standing long jump. The average speed (throwing and kicking) and distance (jumping) of the best three out of five trials will be used for data analysis. Children will attempt to catch an all-ball (Sportime, School Specialty, Greenville, Wisconsin) five times with a research staff member (thrower) tossing the ball from 9 feet away with a standardised procedure (throws to chest, head, waist and right and left sides) according to age. The number of catches out of five will be used for data analysis. Product scores of hopping and running across a distance of 22 feet will be analysed from videotape through video motion capture processing with Dartfish software (Dartfish Inc, Fribourg, Switzerland). The average hop stride length (from heel to heel) for four consecutive hop cycles of each leg will be calculated by digitising stride length using motion capture (Dartfish, Inc). Running speed will be calculated from four consecutive stride cycles using motion capture (Dartfish, Inc). A 22 feet straight line will be used to complete the hopping and running tasks. Hopping, running and jumping data will be normalised to a per cent of standing height.74 75 See figure 2 for a part of the motor skill assessment setup.

Product measures setup for kicking, throwing and catching motor skills.
Physical Activity. Participants will wear ActiGraph accelerometers (model wGT3X-BT; ActiGraph, Pensacola, Florida, USA) secured by a hospital band on their non-dominant wrist for one full week (ie, 5 weekdays and 2 weekend days). The devices will be placed on the participants during the school day and set to start recording at midnight of the following day. The devices will be removed after seven full days of recording. The devices will be set to collect data at 30 hz. Time spent in intensity categories will be based on vector magnitude minus the value of gravity (g) (ie, (x2 + y2 + z2)1/2 – 1) referred to as ENMO (Euclidean norm minus one). The primary outcome will be minutes in MVPA per day but additional measures of physical activity will be analysed based on the current physical activity recommendations.4 77 Hildebrand cut points will be applied to physical activity data78 79 with the MVPA defined as activity over 201 mg. To be considered a valid wear, participants will need to have at least 12 hours of valid accelerometry data per day for at least 4 days (3 weekdays and 1 weekend day80 81). Non-wear time will be defined as when either the SD is less than 13 mg for two of the three axes or when the value range of each accelerometer axis is less than 150 mg, calculated for moving windows of 60 min with 15 min increments.82
Before the onset of each physical activity data collection, a research staff member will explain the purpose of the accelerometer and will demonstrate its use and placement. Compliance with wearing accelerometers will be facilitated by; (1) a letter to the parents which explains placement and provides a simple diagram, (2) use of parent-teacher conference night or open house events, and so on to physically show the parent how to place the accelerometer on the child if needed (both teachers and parents were provided with spare bands), (3) stickers on the accelerometer to indicate correct placement, (4) introduction of the devices to preschoolers and teachers before formal data collection, (5) text messages, phone calls and flyers as prompts and reminders, (6) checking the placement of the accelerometers each day of data collection and (7) an incentive gift card (US$10) on the return of the device.
Secondary outcomes
Perceived physical competence
Perceived physical competence will be assessed with the Harter and Pike Pictorial Scale of Competence and Social Acceptance - physical competence subscale47 83 and the Digital-Scale of Perceived Motor Competence.84 Harter and Pike’s physical competence subscale measures children’s perceived physical competence. It consists of six items that are presented in static pictures and each child selects a picture that is more like him/her. The six items are swinging, climbing, tying shoelaces, skipping, running and hopping and different age-appropriate pictures are used in first/second grade.47 83 Internal consistency reliability for the total assessments (all four subscales) range from 0.66 to 0.89 and reliability for the physical competence subscale is 0.66.47 83 The Digital-Scale of Perceived Motor Competence is a video-based assessment that allows individuals to see the entire motor skill executed rather than a static picture.84 The scale has the identical layout and item structure to Harter and Pike’s Scale of Competence and Social Acceptance but aligns with the fundamental motor skills of the Test of Gross Motor Development.71 72 The Digital Scale of Perceived Motor Competence demonstrates excellent test-retest reliability (ICC=0.83, total; ICC=0.77, locomotor; ICC=0.79, object control/ball skills) and acceptable/good internal consistency (α=0.62, total; α=0.57, locomotor; α=0.49, object control/ball skills).84 The ICCs for the data collected in the PATH study will be reported in papers that discuss the research findings.
For both assessments, children (1) will select the picture/video that is most like him or her (a competent/skilled or not competent/skilled) and (2) will focus on the designated picture/video and indicate whether the picture/video is just a ‘little bit’ or ‘a lot’ like them. Separate pictures/videos for girls and boys will be used following the procedures manual. The range of scores for each item on the subscale is 1 (low competence) to 4 (high competence). Both assessments are established tools and standardised test protocols will be used.47 83 84 For analysis, these two measures will be examined separately since one is a measure of physical competence and the other is a measure of fundamental motor skills competence.
Anthropometrics
Height, weight and waist circumference will be measured according to the standard procedures.85 86 Waist circumference will be measured with a non-elastic tape measure (Seca 201; Seca North America, Chino, California, USA) at the umbilicus.87 The measurement will be taken as the children complete a breath (ie, exhaled). Height will be measured to the nearest unit in bare feet with the child standing upright against a portable stadiometer (Charder HM200P PortStad, Taiwan ROC). Weight will be measured to the nearest unit with heavy clothes removed (ie, wearing pants and shirt) using a portable electric weight scale (Seca 813; Seca North America). All scales will be calibrated before testing. Body mass index (BMI) will be calculated based on age-specific and sex-specific CDC (Centers for Disease Control and Prevention) growth charts and transformed into BMI z-scores for analyses. Inter-rater and intra-rater reliability of data collection staff will be assessed at baseline data collection and monitored throughout data collection.
General family and behavioural factors
Parents/guardians will complete a survey to obtain an understanding of the child’s demographic, family, and home environment to help inform data. This information is not a main outcome variable for the PATH study. The survey includes questions about the child: race/ethnicity, spoken language, family structure, parental educational level, parental and child physical activity habits/behaviours and child’s sleeping habits and access to media. Questions from previously established and valid surveys such as the Preschool-age Physical Activity Questionnaire88 and Tayside Children’s Sleep Questionnaire89 will be used.
Sample size (sample size and power calculation; randomisation and allocation; blinding; implementation; data management)
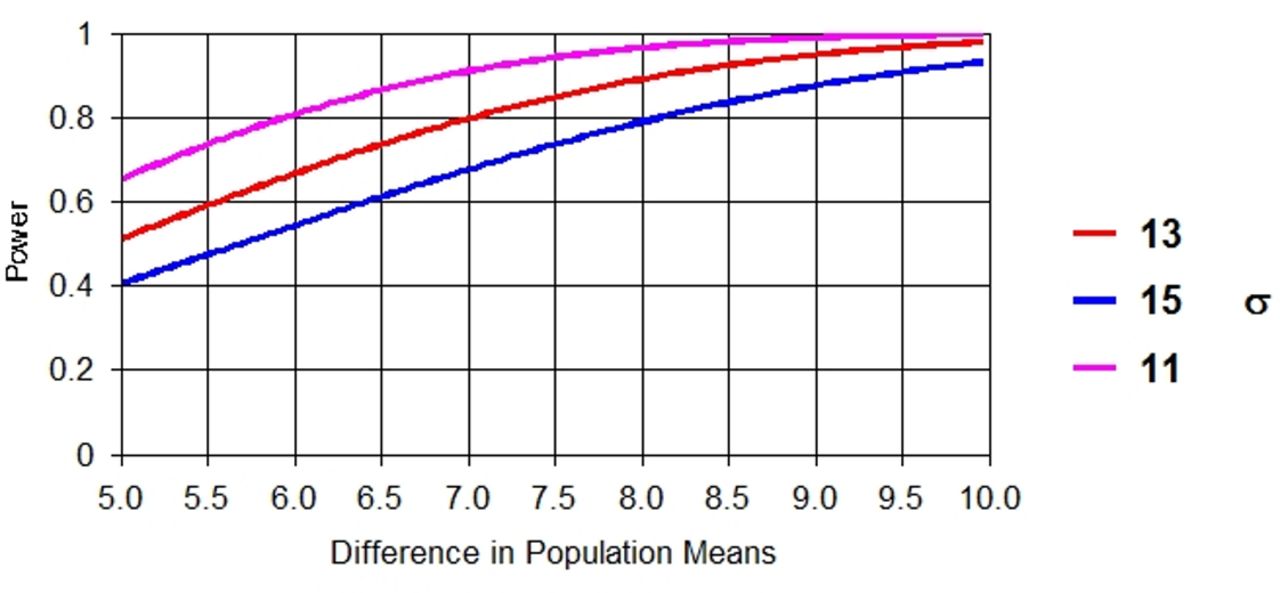
The sample size calculation will be based on the change in physical activity between baseline and immediate follow-up, our primary endpoint. According to previous literature90 we anticipate a change score of 12.1 min of MVPA per day for the intervention group after 1 year, with a conservative estimate of the SD as 27 min MVPA per day. Such a change is accepted as a clinically meaningful change in improving physical activity among preschool children. To detect an adjusted 12.1 min (SD=27) difference in physical activity after 1 year between intervention and control groups with 90% power at an alpha level of 0.05, a total of 212 subjects (106 subjects per arm) are needed. To account for a total of a 30% loss to follow-up, 298 participants is the target recruitment enrolment number (149 subjects per arm). To maintain the statistical power as 90%, the needed sample size and the detectable differences in change of physical activity scores are summarised in figure 3.91 Cohort feasibility data supports no difficulties in identifying subjects who meet the initial inclusion criteria for this study. With the proposed sample size, the relationship between the power we can achieve for analysing the mean change of motor performance and perceived physical competence score and their corresponding expected mean difference and SD appears in figure 4.91 Given expected larger effects on motor performance and perceived physical competence, the power to detect differences across groups is larger for motor performance and perceived physical competence than that seen with the physical activity.

Sample size to achieve 90% power for physical activity.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Power to detect changes in motor performance and perceived motor competence.
Measures will be taken to retain all participants overtime. However, we do expect to lose participants in both the intervention and control groups over time. A conservative estimate of this attrition rate is 30% during the study period. We plan to implement the intent-to-treat analysis.92 We will make every effort to collect follow-up data at each time point from individuals who have not withdrawn from the study. Our approach will include rewards and incentives to gather follow-up data.
Data analyses
Analyses of primary outcomes
Before conducting outcome analysis, we will examine the range and frequency distributions for all variables and will transform variables when appropriate. Preliminary analyses will assess each outcome cross-sectionally at baseline and at all follow-up time points. We will compare study groups (ie, CHAMP vs Control) for comparability and change in variables over time. To study both the short-term (immediate) and long-term (sustainable) effects of CHAMP, we will assess all longitudinal outcomes by both summary statistics and descriptive data figures over the baseline, post-intervention and the start and end of the academic year during Years 2, 3 and 4. Since the samples will be collected in different classrooms and different preschools, our data will have a clustered structure, which means within-cluster correlations likely exist.
For such clustered longitudinal data, we will use primarily random effects in the following models to account for multilevel correlations among the measurements: Mixed Model Regression, Growth Curve Modelling and Structural Equation Modelling.93–96 Random effects are appealing here to account for some latent mediating factors that may exist in the study. We will use the Mixed Model Regression to determine the effects of our proposed intervention on primary and secondary outcomes (Aim 1 and 2). Growth Curve Models will be used to understand if, and how, time-course changes in motor performance, perceived physical competence and physical activity differ between the intervention and control groups and Structural Equation Modelling for mediation analysis (Aim 3).
More specifically, in Aim 1, the immediate post-intervention effect of CHAMP (compared with control participants) on each outcome variable will be evaluated at post-intervention (Month 9). We will examine descriptive statistics on both pre-intervention and post-intervention measures of the outcome variables for each group. The change in motor performance, perceived physical competence and physical activity (ie, physical activity refers to time spent in MVPA) will be compared between two groups using regression models, adjusting for other confounding factors (eg, age and sex). Random effects will be included in the model to accommodate the potential within-cluster correlation coming from the nature of how the data are collected. We will investigate the amount of attrition from pre-intervention to post-intervention, and attempt to identify the baseline predictors of the likelihood of dropping out (as an indication of possible bias in the change estimates).
In Aim 2, we will use Mixed Model Regression to analyse the clustered longitudinal data from our RCT to assess the long-term effects of the CHAMP intervention on improving the three outcome measures: motor performance, perceived physical competence and physical activity. In this analysis, we can obtain the estimates of the long-term longitudinal intervention effect by adjusting for confounding factors that include sex and age. For physical activity and BMI, we will test for a possible delay before any significant change because of the difficulty of achieving health behaviour change by adding time-lagged covariates related to behaviour changes in the regression analysis. We will also conduct exploratory analyses to test interaction effects to understand potential modified intervention effects by different levels of behaviour changes. The intervention is designed to promote a positive trajectory of children’s motor performance, perceived physical competence, and physical activity, and we will specifically test interactions between intervention and time and between baseline motor skills, perceived physical competence, and time to see which baseline measure is a stronger driver of increasing physical activity.
In Aim 3, we will apply the Growth Curve Models to understand if, and how, time-course changes in motor performance, perceived physical competence and physical activity differ between the intervention and control groups. This model is also used to determine a time window over which the intervention effect appears stronger. We will use Structural Equation Models to determine which hypothesised constructs might be responsible for the intervention effect on longitudinal physical activity. Based on the results of our previous work, for example, we hypothesise that perceived physical competence will not mediate the relationship between motor performance and physical activity at baseline, but perceived physical competence will mediate the relationship between motor performance and physical activity immediately post-intervention and across the 3-year follow-up period. We will use Mplus software to fit Structural Equation Models, and the goodness of fit of Structural Equation Models will be assessed using multiple criteria such as χ2 to df ratio (<2) and the root mean square error of approximation (<0.05).
Our goal is to have limited missing data but there is a potential for missing data. Assuming that data are missing at random, multiple imputation techniques will be used to replace missing data.97 Missing data will be assumed to be missing at random if no participant demographics or primary outcomes are correlated with missingness. Mixed-effects models allow for partial information to be included for individuals who may dropout before any post-intervention data collection periods. Missing values will be multiply imputed using available covariates by sequential imputation. This approach allows optimal use of the available data in analysis involving change measures.
Data management
Extreme care to ensure high-quality and secure data will be exercised. All data will be stored securely at the University of Michigan and partial data (product measures) at the University of South Carolina. All data will have only a numerical identifier so that individual respondents, except for video data, cannot be identified. All data will be reported as aggregate statistics and no individuals will be recognisable from the data reported. All data will be perused for consistency, errors of omission and appropriateness of the response. Once a coded and cleaned data file has been prepared, frequency distributions and descriptive statistics (means, SD and ranges) for each of the measured variables will be used for consistency checks and to verify the comparability of the groups. Logic check programmes will be run to ensure that each data point falls within the expected range or corresponds to possible values in the codebook. These tracking system files will be maintained on a secure server at the University of Michigan. Data will be analysed using SAS 9.3.97 98 All members of the study team will be required to complete the web-based National Institutes of Health University of Michigan Responsible Conduct of Research training programme. The investigative team will engage in the ongoing data management training, data monitoring and measurement training throughout the investigation.
Study status
The PATH study is ongoing and currently conducting follow-up assessments. The intervention phase of the study has been completed for Cohort 1 and Cohort 2. Cohort 1 has follow-up assessments for T6, T7 and T8 and Cohort 2 has follow-up assessments for T4, T5, T6, T7 and T8 remaining. Data collection for this project will conclude in 2022.
Discussion
Research suggests that physical activity has numerous health benefits, but only half of preschool-age children are meeting the current physical activity guidelines.9 10 We addressed the low levels of physical activity in children with a movement-based approach. Children need to acquire a level of competency in motor skills and these behaviours contribute to an active lifestyle and physical activity engagement.17 19 52 99 Data supports that an optimal level of motor competence is needed in the early childhood years to support adequate levels of physical activity.19 99 This study examined the immediate and sustained effects of a motor skill intervention, CHAMP, on motor performance, physical activity and perceived physical competence. The study also tested the immediate and long-term mediating effects of perceived physical competence on motor performance and physical activity.
This study addresses the underlying mechanism of physical activity from a developmental perspective. Specifically, the developmental perspective outlines two important facets of children. First, motor skills are cumulative and not transient like physical activity,100 and second, developing a foundation for these skills along with high perceived physical competence will influence a child’s physical activity engagement17 19 52 99 along with other factors that include their cumulative success, intrinsic motivation and enjoyment in movement experiences. Based on previous work, the theory-driven approach used in CHAMP is specifically designed to address these facets. CHAMP uses a mastery-climate instructional approach, and does not equate to a ‘one size fits all’ approach. Children are in a movement environment that promotes opportunities to develop based on their specific individual needs and choices regardless of their skill ability. The CHAMP intervention allows each individual child to be successful and learn while promoting intrinsic motivation and autonomy.
In this investigation, we aim to use an evidence-based intervention, CHAMP, that focusses on developmentally appropriate, context-specific movement activities that promote motor performance and perceived physical competence along with the potential immediate and long-term impact on physical activity. The literature identifies a consistent correlate between perceived physical competence and physical activity, but most studies have only examined a ‘snapshot’” of these constructs. Few, if any investigations, have focussed on intervention strategies or ways to enhance perceived physical competence in parallel with developing motor performance and examine these changes over time. Trained movement specialists will deliver CHAMP and if this work is shown to be effective, key elements related to the implementation of a mastery-climate school-based motor skill intervention will be identified. This knowledge could be organised and used to train classroom and/or physical education teachers in the intervention approach and then used to test the feasibility of dissemination and implementation. Consequently, the intervention could be scaled to a larger number and impact more children.
Ethics and dissemination
Informed parental written consent will be required from participants before conducting this study and all children will be asked to assent prior to their participation in data collection. All participants will be given a unique identification number. The study results will be used for the future development of motor skill intervention programmes while improving implementation quality and effectiveness for school-based intervention studies. Dissemination will be targeted at multiple levels and will include yearly project research reports for the funder and circulation of findings and reports to parents, teachers and principals at the public schools. The National Institutes of Health (NIH) only requires applications that request a direct cost of US$500 000 or greater in any single year to have a resource sharing plan. Disseminating findings is critical to the transparency in science and an important contribution to the scientific community. Findings will also be disseminated through publications in peer-reviewed journals and attendance at conferences and events for those working within the field of physical activity and public health. Once the investigative team has completed all analyses, a final de-identified data set will be made available for analyses for future PostDoctoral fellows and PhD students at the University of Michigan and University of South Carolina. Data would be available to students outside of these universities on request and after signing a data usage agreement with the PI. Potential users of the data must agree to conditions of use, including but not limited to: restrictions against attempting to identify study participants, reporting responsibilities and proper acknowledgement of the data resource. No data on individual persons will be published, only group data will be reported. Following current NIH policies, investigative findings will be made public through PubMed Central and appropriate research resources.
Acknowledgments
The study is funded by a 5-year grant from the National Heart, Lung and Blood Institute (NHLBI) at the National Institutes of Health (NIH); R01-HL-132979 $2 564 256. The Principal Investigator (PI) is Leah E Robinson, PhD, School of Kinesiology and Center for Human Growth and Development at the University of Michigan. The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of NIH. The PI thanks the CMAH Laboratory students and staff for their commitment to the PATH Study: Kara K Palmer, PhD, Katherine M Chinn (Research Technician), Katherine Scott-Andrews (PhD Student), Indica Sur (Project Manager), Carissa Wengrovius (PhD Student), Emily Meng (Research Assistant), Marcia Wallin (Laboratory Coordinator) and all of the Undergraduate Research Assistants (Jacob Kamm, Annalise Lane, Sarah Rock, Samantha Darmon, Brooke Perras, Emma Fellows, Jacquelyn Farquhar, Michael Nunu). The project could not be completed without you and words cannot express how much I am indebted to you. Drs Cathy L Antonakos and Karin A Pfeiffer provided assistance with physical activity, analysis and methodology. The PI also thanks Adam Pennell and Bryan Terlizzi of the University of South Carolina and Sanne Veldman.
References
Footnotes
Contributors LR is the Principal Investigator for this project and LR, NC, DS, DU and LW contributed to the study conception. LR wrote the first draft and final version of this manuscript. NC and LW made substantial contributions to drafting this manuscript and LW is responsible for the statistical analyses section. All authors performed at least one review/critique of the manuscript and approved the final version.
Funding This work is supported by the National Institutes of Health (NIH): National Heart, Lung and Blood Institute grant number R01-HL-132979. NIH has no role in the design of the study, data collection, data analysis and/or data interpretation and writing.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.