Article Text

Abstract
Introduction Rhabdomyosarcoma (RMS) management depends on risk stratification at diagnosis and treatment response. Assessment methods include CT, MRI, bone scintigraphy, histological analysis and bone marrow biopsy. Advanced functional imaging (FI) has potential to improve staging accuracy and management strategies.
Methods and analysis We conducted a systematic review (PROSPERO 2013:CRD42013006128) of diagnostic accuracy and clinical effectiveness of FI in histologically proven paediatric RMS. PRISMA guidance was followed. We searched 10 databases to November 2013. Studies with ≥10 patients with RMS which compared positron emission tomography (PET), PET-CT or diffusion-weighted imaging (DWI) MRI to conventional imaging at any treatment stage were included. Study quality was assessed. Limited, heterogeneous effectiveness data required narrative synthesis, illustrated by plotting sensitivity and specificity in receiver operating curve (ROC) space.
Results Eight studies (six PET-CT, two PET) with 272 RMS patients in total were included. No DWI-MRI studies met inclusion criteria. Pooled estimates were not calculated due to sparseness of data. Limited evidence indicated initial PET-CT results were predictive of survival. PET-CT changed management of 7/40 patients. Nodal involvement PET-CT: sensitivity ranged from 80% to 100%; specificity from 89% to 100%. Distant metastatic involvement: PET-CT sensitivity ranged from 95% to 100%; specificity from 80% to100%. Data on metastases in different sites were sparse. Limited data were found on outcome prediction by PET-CT response.
Dissemination and ethics PET/PET-CT may increase initial staging accuracy in paediatric RMS, specifically in the detection of nodal involvement and distant metastatic spread. There is a need to further assess PET-CT for this population, ideally in a representative, unbiased and transparently selected cohort of patients.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first systematic review of the use of advanced functional imaging in the management of rhabdomyosarcoma (RMS) in children and young people.
No studies of diffusion-weighted imaging-MRI in managing rhabdomyosarcoma of sufficient quality for inclusion were identified.
Rigorous methodology identified the limitations of the existing research supporting this use of positron emission tomography (PET)/PET-CT in the staging, prognosis development and outcome assessment of diagnosed RMS.
Paucity of evidence prevented meta-analysis of sensitivity and specificity and contributed to considerable uncertainty around the true value of PET-CT, including whether it should be considered as an additional or a replacement diagnostic tool.
Potential benefits of PET-CT in increasing staging accuracy were identified: specifically identification of nodal involvement and metastatic spread. Clear research recommendations for incorporation of PET-CT into future treatment trials are presented.
Background
Rhabdomyosarcoma (RMS) accounts for over 50% of sarcomas in children and young people.1 ,2 Incidence is 4.6 per million aged <20 years. RMS frequently presents as a soft-tissue mass. The commonest sites of origin are head and neck, genitourinary tract, and limbs. Treatment is based on a multimodality approach including neoadjuvant chemotherapy, surgery where possible, radiotherapy and adjuvant chemotherapy. Overall outcomes have improved but remain suboptimal, with 3-year event-free survival (EFS) rates for patients with localised disease of around 60% in Europe and a corresponding overall survival (OS) of 80%.3 ,4 Patients who present with metastatic disease have much poorer prognoses and should be considered for novel treatment strategies. Correct staging is imperative.
Current treatment protocols rest on decisions at several points during therapy. Full initial staging employs cross-sectional imaging of the primary tumour (often with MRI); further cross-sectional imaging of the chest, abdomen and pelvis; a radiolabelled bone scan; and pelvic bone marrow biopsies. These methods are also used to assess disease response for treatment modification and at the end of treatment as ongoing surveillance.3 The usefulness of assessment methods is under ongoing evaluation; a recent European paediatric Soft tissue Sarcoma Group (EpSSG) analysis showed that otherwise low-risk patients are unlikely to have isolated bone metastasis; in future bone scans may be omitted for these patients.5 Current assessment methods give discordant results at postchemotherapy evaluation, highlighting the potential importance of functional imaging (FI).6
FI has been incorporated into management of other malignancies (eg, staging non-small-cell lung cancer (NSCLC) and assessing treatment response in Hodgkin's lymphoma) after extensive reviews found strong evidence for positron emission tomography (PET)-CT.7 It was found to be cost-effective for assessment of recurrent colorectal cancer,8 but was less useful than non-nuclear technologies (eg, functional MRI and nodal biopsies) in regional node evaluation in breast cancer.9 Previous systematic reviews with meta-analysis of sarcomas generally have found uncertain and heterogeneous results.10 ,11
This is the first systematic review of FI in children and young people with RMS diagnosis. FI has potential as an additional imaging technique or replacement for current imaging modalities for initial staging and/or response assessment.
Objective
To assess the role of FI (PET/PET-CT and diffusion-weighted imaging (DWI)-MRI) in the management of RMS in childhood and adolescence and to consider its potential as a tool for improving both diagnostic (staging) and prognostic evaluation. Assessment of FI for treatment response and end of treatment evaluations were secondary aims. The review was not designed to assess the differential diagnosis of RMS in patients with suspected sarcoma.
Methods
We undertook a systematic review of the diagnostic accuracy and clinical effectiveness of PET, PET-CT and DWI-MRI for assessment of histologically proven RMS in children and young people. The protocol was registered on PROSPERO (2013:CRD42013006128)12 and PRISMA guidance adhered to. We consulted three public patient (PPI) representatives while writing the protocol and they contributed to the selection of outcomes assessed.
We searched 10 databases (including MEDLINE, EMBASE and Cochrane Central Register of Controlled Trials) from inception to November 2013 without restrictions on publication status, date or language (see online supplementary appendix 1 for full list of databases and complete search strategies).
The following prespecified inclusion criteria were applied:
Participants: Children and young people aged 0–24 years of age who are diagnosed with histologically proven RMS of any type. Studies with mixed tumour types will be included if outcome data for RMS patients are reported separately for at least one outcome. Studies with mixed populations of children/young people and adults were included where it was clear that a majority of patients were children/young people.
Interventions: FI: PET±CT, or DWI-MRI used at any point in the management of RMS.
Comparator: Conventional imaging (one or more of contrast-enhanced CT or standard MRI, technetium-99m bone scintigraphy).
Primary outcome: EFS or OS at any time point.
Secondary outcomes: Relapse rates, quality of life, adverse events or acceptability of the technology (by patient, carer or health professional), histological confirmation via lesional biopsy, or independent imaging or comparative classification of staging and risk classification of disease and treatment alteration in the light of imaging tests performed.
Study design: Prospective and retrospective studies of any design with at least 10 patients with RMS for whom separate data are available for at least one outcome (following a protocol amendment due to lack of data; originally studies were required to include ≥20 patients with RMS).
Studies were assessed for inclusion and appraised for quality by two independent reviewers. We used a tool adapted from previous Health Technology Assessment (HTA) reviews13 ,14 for quality assessment of case series. We also assessed the reliability of the processes followed in carrying out PET and the degree to which accepted guidelines for the semiquantification using standardised uptake values were followed.15
Data were extracted onto a prespecified form using the package EPPI-Reviewer 4 from the UK EPPI-Centre by one researcher and checked by a second (forms were piloted by two independent researchers). A third researcher was consulted where necessary. Patient-level data were extracted to enable construction of 2×2 tables for detection of nodal involvement and distant metastases. Sensitivity and specificity of PET and conventional imaging were calculated for each study and plotted in receiver operating curve (ROC) space using the METANDI package in STATA. There were insufficient data to calculate pooled sensitivity and specificity.
At all stages of the review process, we attempted to contact study authors about uncertain, missing or incomplete data.
Owing to the limited and incomplete nature of the data reported, data at the level of individual primary, nodal or metastatic sites were summarised in a narrative synthesis. Data on survival, tumour response and treatment modification were very limited and heterogeneous so were also summarised narratively.
Results
Quantity and quality of evidence
We identified 1725 unique records and assessed 300 as full-text papers. Six studies of PET-CT16–21 and two of PET22 ,23 were included; these were reported in a total of 15 publications16–30 and the most up-to-date data were used in the review (see online supplementary appendix for flow diagram). All studies had a full primary English publication; in one case, survival data were available only in abstract.29
Seven studies included only patients with RMS;16–19 ,21–23 one included a minority of patients with RMS with separate data.20 Data were reported on a total of 272 patients with RMS. Two additional studies reported in abstract included >10 patients with RMS but were excluded as, despite author contact, we were unable to obtain separate RMS patient data.31 ,32 One study reported separate RMS data only for the subset of patients with a primary tumour in the extremities and was included because of these data.20 Three studies included one or more adults aged ≥25 years; these studies were included because it was clear that the great majority of patients were children/young people; median ages were 11 and 13 in two studies17 ,23 and the mean age in the third was 19.8.19
No studies of DWI-MRI met inclusion criteria (even after protocol amendment from >20 cases to >10 cases); only studies that assessed it for differential diagnosis with very few RMS cases were found.33–39 These studies of DWI are discussed elsewhere.40 A full list of excluded studies is available on request.
All studies used fludeoxyglucose (fluorodeoxyglucose, 18F) as the radiopharmaceutical for PET. Most studies reported using all possible conventional imaging techniques as a comparator to PET or PET-CT (see table 2). The reference (gold) standard (as distinct from the comparison with conventional imaging) was typically a mixture of histopathology, clinical examination and follow-up.
Included studies often involved more children with unfavourable prognoses than would be expected in clinical practice: 52% of the patients in the series had an unfavourable, alveolar histology compared with 20–30% in clinical practice.1 Histology was generally not well described and information on genetic predispositions was limited to one study which noted that no patient had a history of familial cancer syndrome.21 Where reported, large numbers of patients had stage III or IV disease compared with around 15% with stage IV disease in clinical practice.41 Several studies included higher numbers of patients with primary tumours of the extremities. Study characteristics are summarised in table 1.
Participant characteristics
All studies were opportunistic case series. Most were retrospective and did not comprise consecutive series of patients. It was often unclear how representative of the eligible population the included patients were. Details of FI procedures were often not reported. See online supplementary appendix 2 for a summary of quality assessment results. Outcome reporting was inconsistent and often incomplete. In some cases this was remedied by contacting authors.
Survival and related outcomes
Only one study (N=41) reported data on OS.22 This found that metabolic activity of the primary tumour on PET-CT had prognostic significance for survival (p=0.007). Also predictive of survival were PET-CT detection of nodal involvement (p=0.016), PET-CT detection of metastases (p=0.002) and a composite outcome (PET group; p=0.002). Dichotomisation around the point SUVmax/SUVliver=4.6 was also predictive (p=0.002). Nodal and metastatic involvement retained statistical significance in a multivariate analysis; primary tumour intensity did not.
Three studies reported data on EFS.17 ,22 ,29 One (N=41) found similar results for EFS as for OS, with prognostic significance for primary tumour intensity (p=0.005), lymph node detection (p=0.008) and metastases detection (p=0.01). Dichotomisation around the point SUVmax/SUVliver=4.6 did not predict EFS.22 Another study (N=94) reported trends towards prognostic significance for PET-CT results dichotomised by SUVmax=7.0 at initial staging (p=0.08) and by pre-radiotherapy (RT) PET-CT-positivity (after median 15 weeks chemotherapy; p=0.06).17 At post-RT assessment PET-CT-negative patients were significantly less likely to relapse than PET-positive individuals (p=0.02). The third study (N=38), available as an abstract, reported no prognostic significance of PET-CT at any point.29 None of these reports demonstrated an additional prognostic value of metabolic activity indices above conventional prognostic criteria.
One study reported tumour response.16 In a subset of 13 patients PET-CT was more likely than conventional imaging to show complete response to treatment; most of these patients were assessed by conventional imaging as having a partial response and 12 were in remission at follow-up.
Treatment alteration
PET-CT changed the management or treatment course of 7/40 patients in studies that reported this outcome.16 ,20 ,21
Quality of life and acceptability
There were no data on quality of life or acceptability of the technology. All three PPI representatives considered that additional scans (and their associated requirements of time, travel and additional procedures) were worthwhile if they could provide additional information to inform the treatment plan and/or prognosis.
Diagnostic data
Lymph nodes
For nodal involvement, PET-CT or PET showed sensitivity of 80% (one study)18 or 100% (three studies)19–21 and specificity of 89–100% at the patient level. This is compared to sensitivity of between 67% and 86% and specificity of 90% or 100% for conventional imaging (table 2 and figure 1). The ROC space ‘cross-hairs’ plots show each study’s estimates of sensitivity and specificity as a marker at the point estimate, with 95% CIs demonstrated by lines. In reading such graphs, tests with better discriminatory ability fall in the top left corner of the plot, and non-discriminatory tests fall on a 45° line between the bottom left and top right.42
Summary of patient-level diagnostic data: detection of nodal and distant metastatic involvement

Sensitivity and specificity of positron emission tomography-CT versus conventional imaging in detection of nodal involvement plotted in ROC space.
Nodal level data from three studies also indicated that PET-CT was able to detect more positive nodes than conventional imaging with very few false positives.16 ,18 ,21 One study with fully reported data found sensitivity and specificity of 100% for PET-CT compared with 75% and 94% for conventional imaging.16 Where reported, PET-CT generated many fewer indeterminate results (1 vs 18/35) and more true negatives than conventional imaging.18
Distant metastases
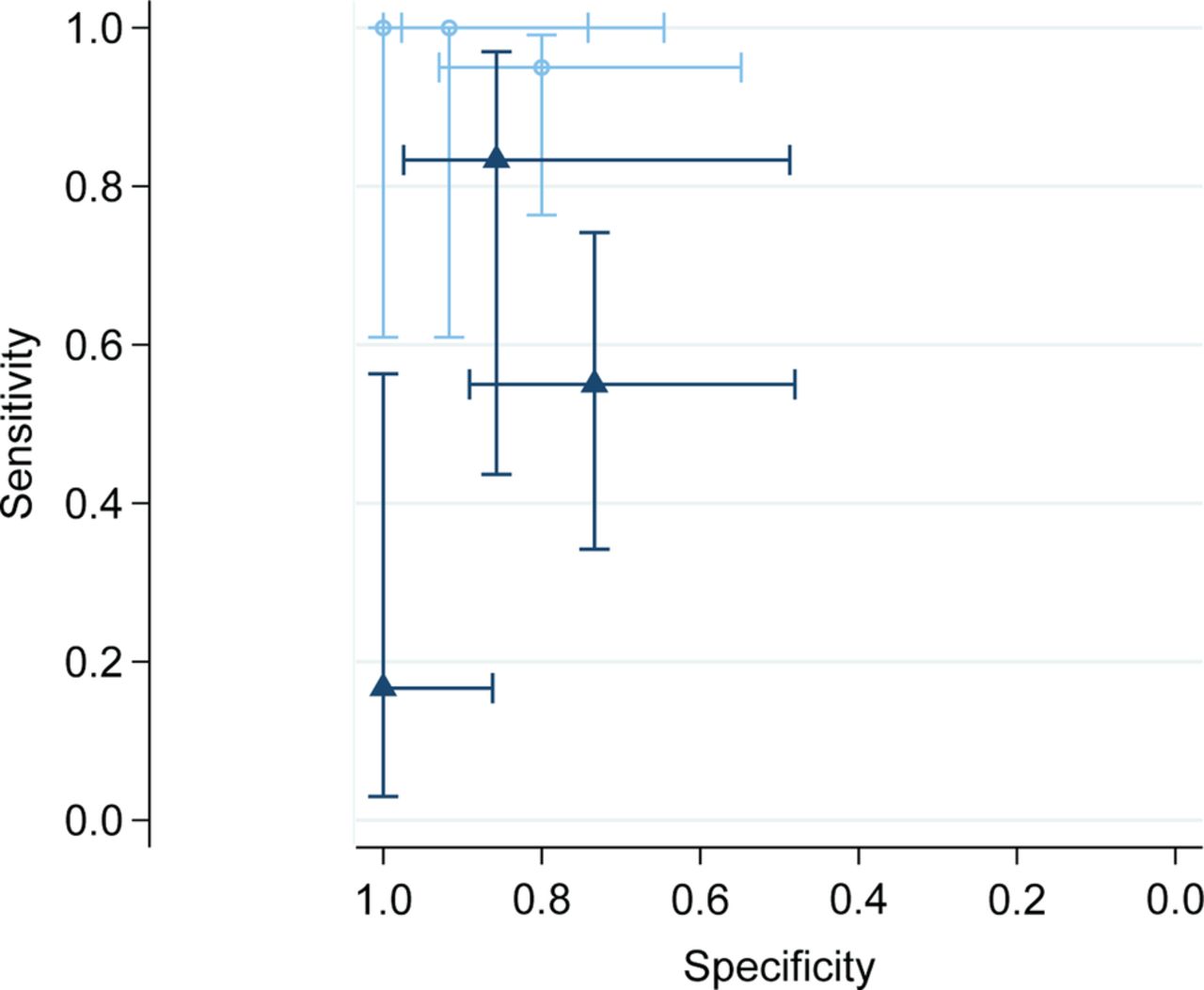
For detection of distant metastatic sites, PET-CT had a sensitivity of 95% (1 study)19 or 100% (2 studies)18 ,21 and specificity of 80–100% at the patient level. This is compared to sensitivity of between 17% and 83% and specificity of between 43% and 100% for conventional imaging (table 2 and figure 2).
{kind=link}
{kind=link}
Sensitivity and specificity of positron emission tomography (PET)-CT versus conventional imaging in detection of distant metastatic involvement plotted in ROC space.
Site level data from another study also found higher sensitivity and specificity (100% and 96%) for PET-CT compared with 66% and 91% for conventional imaging.16
Information on detection of metastases in different sites was extremely limited and reported at the level of individual cases (table 3).16 ,18 ,19 ,21 There were indications from this very limited evidence base that PET-CT may be superior to CI for detection of bone lesions, in that both additional lesions and patients with otherwise undetectable bone involvement were identified.16 ,18 ,19 ,21 The number of false positives was low. PET-CT may also have potential to specifically identify marrow involvement in some patients but this finding is unclear and based on tiny numbers of patients; sensitivity appeared limited.18 PET-CT appeared poor for detection of lung metastases.18 ,21 There were indications that PET-CT may perform better than conventional imaging in detecting soft-tissue lesions in non-pulmonary locations,18 ,19 possibly including distal nodal involvement.21
Summary of detection of metastatic sites
Discussion
We identified eight studies (272 patients) of PET or PET-CT in children and young people with RMS and no eligible studies of DWI-MRI.
The studies identified had multiple limitations. All studies were opportunistic case series open to a range of biases. As such they addressed multiple aspects of the use of PET in RMS management. Patients already had a diagnosis of RMS, so the studies were not diagnostic in the conventional sense; rather they were concerned with accuracy of staging, determination of prognosis and, in some cases, evaluation of treatment outcome. The review was not designed to assess the value of PET-CT in imaging primary tumours, as the requirement for histologically proven RMS diagnosis meant that almost all patients had a known tumour site. This makes comparison to earlier reviews that included all sarcomas unhelpful.10
The studies included a higher proportion of more challenging cases than expected in clinical practice. Imaging methodology was not well reported. Duplicate blinded evaluation of the FI results relative to the conventional imaging results or reference standard was often absent or unclear. Results were often not clearly or fully reported and data remained inconsistent and incomplete even after contacting authors. Our findings are therefore tentative and require confirmation by further research.
PET-CT was consistently somewhat better than conventional imaging at identifying patients with nodal involvement at initial staging and was clearly more sensitive to individual positive nodes, with fewer indeterminate results. PET-CT appeared to improve sensitivity in identification of distant metastases including identifying patients in whom distal metastatic involvement was not otherwise indicated. There is a suggestion of a role for PET-CT in detection of bone involvement but a great deal of uncertainty. Data for lung lesions are sparse and do not suggest utility. These results accord with reviews of PET-CT in staging of osteosarcoma43 and PET in general diagnosis of pulmonary nodules.44
There is very limited evidence on use of PET-CT for treatment response and end of treatment evaluation. Only three studies investigated the primary outcome of survival and one evaluated tumour response. PET-CT at initial staging may have predictive value for OS and EFS. The role of PET-CT in the assessment of treatment response before and after radiotherapy is unclear. PET-CT may be superior at ascertaining complete response to chemotherapy but this is based on one small study. The tentative findings of this review suggest that the performance of PET-CT in RMS may be closer to that in Hodgkin's lymphoma, NSCLC7 and colorectal cancer8 than in breast cancer.9
None of the studies reported data on the impact of FI or conventional imaging on quality of life or acceptability to any identified stakeholder group. Our PPI representatives indicated that potential additional information was highly valued and mattered more than a need for additional procedures and the resource implications of additional scans. They were particularly supportive of FI in further research with potential to clarify possible benefits of additional or alternative imaging procedures.
This systematic review represents the first thorough evaluation of the international evidence on FI in the management of childhood and adolescent RMS. Extensive searching without language restrictions ensured the inclusion of all relevant studies. We made substantial efforts to obtain supplementary data from authors. Although some studies contained patients aged >24 years, we are confident from the mean/median ages reported that these were a small minority of the populations and that the relevance of the studies to the paediatric population was not significantly impacted. Excluding these studies would have resulted in the loss of data on a significant proportion of documented PET use in paediatric RMS. Studies were quality assessed and synthesised to provide an unbiased comprehensive assessment of the evidence.
The key limitation was our inability to obtain all relevant data despite contacting authors. In particular we are aware of two case series in sarcoma patients which included >10 patients with RMS that we could not include as authors were unable to provide separate data on RMS cases. The lack of complete patient-level data from all included studies meant we were unable to calculate pooled estimates for the sensitivity and specificity of FI and conventional imaging. However, even had we acquired full data on all known patients with paediatric RMS, the total number would have remained under 300. Any answers to the review questions would have remained tentative and uncertain. There is an urgent need for more reliable disease assessment at all stages of RMS management. PET-CT may be an option for this with sufficient prospective testing through incorporation into any future trials of RMS treatments.
Conclusion
This review highlights potential from PET-CT in imaging of children and adolescents with RMS but there is a high level of uncertainty in these data and their relevance to clinical practice. Limited evidence suggests that PET/PET-CT has potential to increase initial staging accuracy, specifically detection of nodal involvement and distant metastatic spread. There is little evidence on the impact of PET-CT in assessment of therapeutic response or post-treatment assessment. The ultimate impact of FI with PET-CT on treatment outcomes could not be addressed and it remains unclear whether and how increasing accuracy at initial staging might alter patient management and survival. It was impossible to determine whether PET-CT could replace any current imaging tests or should be used as an adjunct.
DWI-MRI has been insufficiently researched to answer questions of utility in RMS; the very limited evidence base for this is discussed elsewhere.40
Recommendations for further research
A representative, unbiased and transparently selected cohort of patients (entering a treatment randomised controlled trial (RCT)) should be identified. All patients should be evaluated using PET-CT as an adjunct to conventional techniques at initial staging, treatment response and end of treatment.
The protocol should specify interim data analysis, potentially enabling PET-CT to replace one or more conventional staging techniques or substantially modify treatment delivery by response assessment.
Results should be fully reported and individual patient data made available.
Methodology of the PET-CT process should be standardised and reported fully. This should include independent reading of scans by multiple assessors blinded to conventional imaging and clinical/histological results.
Appropriate qualitative methodologies should be used to assess the additional burden of treatment to patients and healthcare system, and resource use prospectively evaluated.
Further comparative research on DWI-MRI in RMS is needed; researchers using this technology in patients with RMS should be encouraged to publish case series in the first instance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Contributors BP designed concept for study, wrote initial draft of protocol, supervised review, undertook analysis, reviewed and edited manuscript. GN contributed to protocol, screened and assessed all papers, developed and conducted data extraction, wrote initial and edited later drafts of manuscript. DF contributed to protocol, screened and assessed all papers, developed and conducted data extraction, reviewed and edited the manuscript. KLL designed and undertook the search strategy, managed the study database and reviewed and edited the manuscript. JC, MJ, SG, DL, HM and KM contributed to the protocol, provided clinical advice to the review, reviewed and edited the manuscript.
Funding This review was funded by the Children's Cancer and Leukaemia Group (UK).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No primary data were collected for this study. Full data extractions for all included studies and a full list of excluded studies are available on request from the authors.