Article Text

Abstract
Objective To provide a brief overview of the Needs and Provision Complexity Scale (NPCS) and report its first application to describe the level of ‘met’ and ‘unmet’ health/social care needs, and to estimate their costs in community-based patients with complex neurological disability.
Design A multicentre prospective cohort analysis.
Setting Consecutive discharges to the community from the nine tertiary specialist inpatient neurorehabilitation units in London over 12 months (2010/2011).
Participants Patients responding at follow-up (n=211). Mean age 50.2(SD14) years, males:females 127/84. Diagnosis 157(74%) brain injury, 27(13%) spinal cord injury/peripheral neuropathy; 27(13%) other.
Primary outcome measure The NPCS is a brief, pragmatic, directly costable instrument for measuring both an individual's needs for rehabilitation and support (NPCS-Needs) and the levels of service provided (NPCS-Gets) within a given period.
Methods The ‘NPCS-Needs’ was completed by the treating clinical team at discharge. Patients and/or their carers self-reported ‘NPCS-Gets’ after 6 months by a postal/online questionnaire supported by a follow-up telephone interview.
Results Needs for medical/nursing care and accommodation were generally well met. Significant shortfalls in provision were identified in the subscales of Rehabilitation (paired t test: t −9.7, p<0.001, effect size (ES)=−0.85), Social support (t −5.8, p<0.001, ES=−0.48) and Equipment (t −5.6, p<0.001, ES=−0.44). Item-level analysis demonstrated that the frequency of Personal care received exceeded predicted needs (Wilcoxon z=−3.3, p<0.001). In 80% of cases, this care was provided/paid for by families. Translated into mean costs/patient/year, the estimated underspends on Rehabilitation (−£2320) and Social support (−£1790) were exceeded >3.5-fold by excess costs of Personal care (£10 313) and Accommodation (£4296).
Conclusions The results identify underprovision of community-based rehabilitation and support services compared with needs, which may contribute directly to excess care burden and costs to family carers. The NPCS requires further evaluation but has potential use as a simple, directly costable tool to inform both clinical decision-making and population-based service planning and delivery.
- Rehabilitation
- Health care
- Social support
- Measures
- Cost Analysis
- Needs and Provision Complexity Scale
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Article summary
Article focus
-
The epidemiology of need for healthcare and support is not fully understood, and the methodology is hitherto lacking for routine-costed evaluation of the level of services provided, in relation to individual needs.
-
The Needs and Provision Complexity Scale (NPCS) is a simple, pragmatic tool to describe the level of met and unmet needs for health and social care, and to estimate their cost, for the purpose of integrated care planning.
-
This article represents its first application to evaluate community-based service provision in comparison with the needs of a cohort of patients with complex neurological disability.
Key messages
-
Significant shortfalls were identified in the provision of rehabilitation, social support and equipment, while provision of personal care (mainly provided by families) exceeded the predicted needs.
-
The underprovision of community-based rehabilitation and support services may contribute directly to excess care burden and costs to family carers which was calculated to average >£10 000/person/year in this study.
Strengths and limitations of this study
-
The NPCS requires further validation and exploration in different settings before our findings may be considered generalisable—however, they resonate with other published studies.
-
The low rate of response (49%) to follow-up evaluation is a weakness. Although no significant differences were detected between respondents and non-respondents, the possibility of selection bias cannot be excluded.
-
The NPCS has the potential to inform both clinical decision-making and population-based service planning and delivery. Methods for future application are discussed.
Introduction
Long-term neurological conditions (LTnC) affect not only the individuals concerned but also their family and carers. The UK National Service Framework (NSF) for LTnC sets out standards for rehabilitation and social support for patients living with neurological disability.1 It emphasises a holistic approach, addressing all stages in the ‘care pathway’ from diagnosis to death,2 and it highlights in particular the need for lifelong access to services in the community.
For effective planning and delivery, health and social services developers require information about the service needs of the local population and the current capacity to meet those needs—as well as the likely costs of addressing any identified gaps in service provision. The NSF for LTnC was published in 2005, with a 10-year implementation plan, but without dedicated funding or defined service targets.3 This posed a challenge for implementation, as service commissioners and providers lacked a clear reference point to determine when the standards were and were not met.
LTnC represent a diverse group of conditions, encompassing people with widely different needs for services, against which the adequacy of service provision must be judged. Unfortunately, these needs are largely unreported through current information systems, so the epidemiology of ‘need’ for healthcare and social support is not fully understood.4
To support implementation of the NSF, the UK Department of Health commissioned the National Health Service Information Centre to develop an LTnC dataset for monitoring implementation and for benchmarking performance against the NSF standards.5 The Needs and Provision Complexity Scale (NPCS) was developed as part of this process, as an aid to routine integrated care planning for people with LTnC.
The NPCS is a brief, pragmatic tool to measure both the needs that an individual has for rehabilitation and support—and the extent to which those needs are met through service provision. Although other tools, such as the Southampton Needs Assessment Questionnaire,6 have been used to explore met and unmet needs for rehabilitation services,7 ,8 the NPCS is the first tool designed to be used both as a measure of the ‘metness’ of need in routine practice and to estimate the cost of meeting unmet needs.9 The NPCS may be used at an individual level to monitor the changing needs of a given patient over time and the services that are provided to support them at different stages along the care pathway. It may also be used at the population level to identify gaps in service provision and to estimate the likely costs of addressing those gaps.
This analysis forms part of a larger study, funded by the UK Department of Health, to pilot a register for patients with LTnC to examine their needs for ongoing services, and to determine how well these are provided for in the community following discharge from postacute specialist rehabilitation.9
Aims
The aim of this article was to provide a brief overview of the NPCS and report its first application in a cohort of patients with complex neurological disability to describe their needs for health and social care. We determine the extent to which these were met, and examine the impact of any overmet or undermet needs in terms of costs (to the individual or society).
Methods
Needs and Provision Complexity Scale
The NPCS is a 15-item measure with six subscales and a total score range 0–50. It has two parts:
-
Part A (NPCS-Needs) is completed by the treating clinician(s) to evaluate each patient's needs for health and social care in any given period.
-
Part B (NPCS-Gets) is a mirror image of the same tool, completed at the end of that period, to evaluate the levels of service that have been provided in relation to those needs.
NPCS development was initiated in 2008 by the LTnC Dataset Development Group. As well as service users and carers, the group consisted of commissioners and healthcare professionals from a range of disciplines, all of whom were experienced in care and planning of services of people with LTnC. The instrument evolved through an iterative process of testing and refinement before publication in 2010.5 Figure 1 shows an exemplar NPCS score sheet, rated for ‘Needs’ and ‘Gets’. In its original form, both parts of the NPCS were designed for completion by clinicians. A patient-report version of the NPCS-Gets was subsequently developed and tested for completion by patients and/or their carers.9

In this example score sheet, the level of need (‘Needs’) for each service is highlighted in yellow on the left, and the corresponding level of provision (‘Gets’) is highlighted in green on the right. Summary scores for each subscale are given at the bottom of each of the two domains.
Psychometric evaluation of the NPCS conducted as part of the larger study9 has provided evidence for its utility, reliability and validity10 which is summarised briefly as follows:
-
Factor analysis identified two principal domains (Health and personal care and Social care and support), accounting for 66% of the variance, but also suggested a single general factor underpinning the full NPCS with good overall internal consistency (Cronbach's α=0.94).
-
Test–retest repeatability for the patient-reported version (as used in this study) was acceptable with intraclass correlation coefficients for domain scores ranging from 0.66 to 0.84, and linear-weighted κ coefficients for item-by-item agreement ranging from 0.42 to 0.83.
-
Concurrent validity was demonstrated through the expected relationships with other measures of dependency, community integration and family caregiver burden.
In addition to the ordinal NPCS scale, an algorithm is used to express the impact of met and unmet needs directly in terms of cost. The costing algorithm was also developed as part of the larger cohort study.9 In the absence of an accepted gold standard for activity and costing this area, intuitive assumptions for annualised activity within each scoring level were drawn up on the basis of clinical experience, and tested through discussion with a peer group of clinicians experienced in the planning and provision of community services. Costs were computed with reference to Curtis 2011,11 adjusted where necessary to reflect the costs of specialist care (see Acknowledgements section). A version of the Client Services Receipt Inventory (CSRI),12 adapted for neurological disability,13 was used alongside the NPCS to collate information on the number and duration of contacts for each type of service.9 As the content of the tools differs and as service provision varies widely, the CSRI could not be used directly to derive the costings, but CSRI data were analysed within each of the NPCS items to ‘sense-check’ the activity and costing assumptions. Significant associations were expected, and indeed found, between the CSRI-estimated and NPCS-estimated total costs (Spearman r 0.59, p<0.0001) and across all domains. Further details regarding the NPCS and its development, together with a summary of the costing assumptions and estimated annualised costs (in 2011) attributed to each item level, are available on our website.14
Design
In this prospective cohort study, the NPCS was used to record:
-
Individual needs for health and social services (NPCS-Needs), as assessed by the treating team at the point of discharge to the community after specialist inpatient rehabilitation.
-
The extent to which these needs had been met through service provision and informal care at 6 months postdischarge (NPCS gets), self-reported by patients/their carers.
We examine the NPCS-estimated mean annual costs of needs and provision, to estimate the likely costs of addressing the identified gaps in service provision for the sample population.
Participants and setting
Consecutive patients discharged from each of the nine tertiary specialist neurorehabilitation units within the London area were recruited over a 12-month period in 2010–2011. All patients with LTnCs were considered eligible to participate. Written informed consent was obtained by the treating team. If the patient was unable to consent or to complete questionnaires due to cognitive and/or communication problems, a family member or carer was identified to give assent and to respond on their behalf.
Data collection
As noted above, data collection was achieved as part of a larger systematic longitudinal cohort study to examine community-based support for patients with LTnC.9 At recruitment, the discharging clinical team completed a summary report which included (1) the Neurological Impairment Scale15 as a measure of severity of impairment and (2) the NPCS-Needs. Teams were instructed to complete the NPCS in accordance with their recommendations to community services for ongoing care/support at discharge.
Patients/carers were contacted at 1, 6 and 12 months after discharge and asked to complete a follow-up questionnaire either online, on paper or through a telephone interview according to their preference. At least 3–5 attempts were made to contact at each time-point. In this analysis, we compare service needs and provision during the critical first 6-month period after discharge from inpatient rehabilitation.
In addition to self-report versions of the NPCS and the CSRI, the questionnaire included measures of dependency (Northwick Park Dependency Scale, NPDS16), community integration (the Community Integration Questionnaire17) and carer burden for those with a family carer (Zarit Caregiver Burden Interview, ZBI18). Copies of the full questionnaire booklet are available on request from the authors.
In their response to the NPCS, patients/carers were asked to report the level of care they had received within the last 6 months and to comment on whether they felt this was the right amount for them, too much or too little (a free text box was provided for elaboration). Following the receipt of the questionnaire, trained research assistants checked the questionnaires for any missing data or ambiguous responses and contacted respondents by telephone to clarify their answers and to confirm their experience of met/unmet needs. The information was then transcribed onto the score sheet in figure 1. If the level of services received had varied during the 6-month period, the maximum level was recorded.
Analysis
Missing data: The NPCS item score data were missing in<5% cases except for one item (Advocacy). No missing data were imputed in this analysis. Cases were excluded pairwise where data were missing.
Descriptive statistics were calculated for needs and provision within the various domains and subscales of the NPCS, as well as for measures of impairment, dependency, community integration and family caregiver burden.
Met and unmet needs were assessed at a case-by-case level for each of the 15 items, and were identified by dichotomising the item difference scores as follows:
-
Met (or exceeded) Needs: NPCS-Gets ≥ NPCS Needs.
-
Unmet Needs = NPCS-Gets < NPCS Needs.
Statistical analysis was undertaken using SPSS V.19. There is debate over the use of parametric or non-parametric statistics for data of this kind. Some argue that non-parametric statistics should always be used for analysis of ordinal data. Others note that summation of ordinal data already assumes numerical value. According to Altman and Bland 2009,19 rank methods are sometimes useful, but parametric methods are generally preferable as they provide estimates and CIs and generalise to more complex analyses, especially where data may have many possible values (ie, long-ordinal data) and samples are large. In this study, we used a combination of parametric and non-parametric techniques as follows:
-
Short-ordinal data (eg, item scores with just four possible values) were summarised by medians and IQRs. ‘Needs’ and ‘Gets’ were compared using non-parametric techniques (Wilcoxon Signed Rank tests).
-
Interval data and long-ordinal data (eg, costs and summed NPCS subscale and domain scores) were summarised by mean (SD) and compared using parametric statistics (paired t tests) with 95% CI. Effect sizes (ES) were calculated as the mean difference between ‘Needs’ and ‘Gets’ scores ÷ SD of the ‘Needs’.
To allow for multiple tests, the threshold for significance was taken as 0.05 ÷ the number of tests.
Power calculation
A post hoc power calculation for comparison of paired means (GPower-4), based on a 0.001 two-sided significance level, showed that an ES of 0.4 in a sample size of 203 provides a statistical power of 99%.
Results
Of a total of 576 discharges, 499 (87%) were assessed for eligibility, of which 428 were recruited. Full details of recruitment, reasons for non-recruitment and flow chart are reported elsewhere.9 A total of 211 (49.3%) returned follow-up questionnaires at 6 months postdischarge and formed the sample for this analysis. The demographic and baseline characteristics of those who did and did not respond at 6 months are shown in table 1. There were no significant differences in age, gender, diagnosis discharge destination, level of impairment or NPCS-identified needs at discharge.
Demographic and baseline characteristics of those recruits who did and did not respond to the follow-up questionnaires at 6 months
There was no significant change in dependency for the respondent group between 1 and 6 months (mean difference in NPDS 0.45, 95%CI −0.51 to 1.47, p=0.34) or in the carer burden (mean difference in ZBI 0.13, 95%CI −2.26 to 2.01, p=0.91). If anything, their levels of community integration worsened slightly (Mean difference 0.88, 95%CI 0.27 to 1.50, p=0.005). These findings suggest that they still had ongoing needs for care and support six months after discharge.
Table 2 shows the differences between NPCS-rated needs identified at discharge and provision during the first 6 months for each subscale and domain, and table 3 provides an item level analysis. Overall, levels of provision were significantly lower than needs for both principal health and social care domains, but subscale and item analysis revealed some notable differences between service types:
-
Within the ‘Health and personal care’ domain, needs for medical, nursing care were relatively well met; whereas needs for rehabilitation were significantly undermet (t −9.7, p<0.001, ES −0.85).
-
Within the ‘Social care and support’ domain, there were significant unmet needs in both the social care (t −5.8, p<0.001, ES −0.48) and equipment (t −5.6 p<0.001, ES −0.44) subscales, while accommodation needs were largely met.
-
Item level analysis showed that, within the personal care scale, needs for a personal enabler were significantly undermet (Wilcoxon z=−6.3, p<0.0001), but the frequency of personal care for activities of daily living was provided at a level significantly above predicted need (z 3.3, p<0.001; see table 3). In 80% of cases, these needs were met by family members (52%) or paid for privately (28%).
Differences between NPCS-rated needs and provision reported during the 6 months (n=211): subscales and domain scores
Differences between NPCS-rated needs and provision at 6 months (n=211): item level analysis
Met and unmet needs at case level
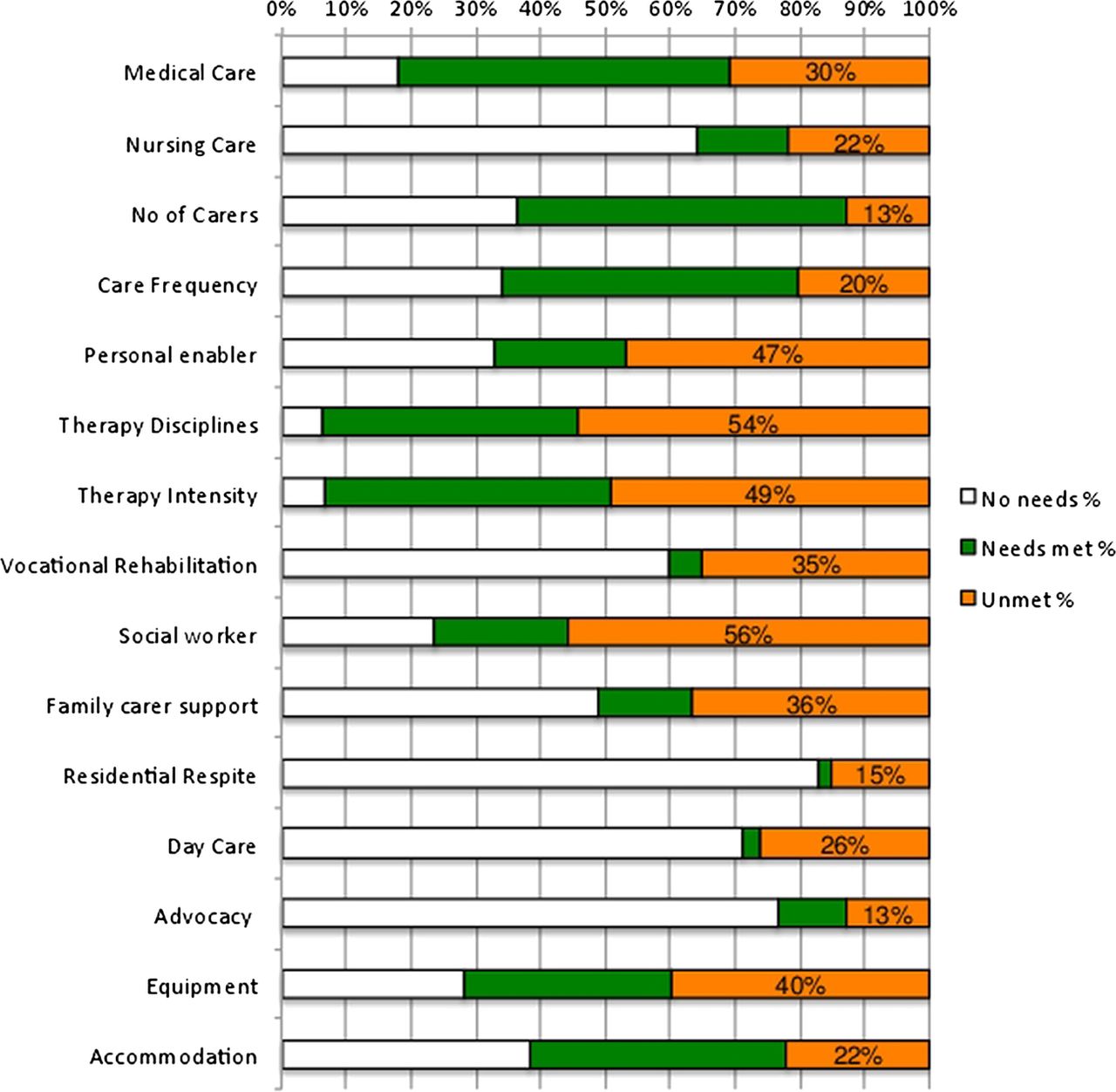
By no means do all patients have needs in every part of the scale. In addition to the population-based statistics described above, the NPCS can also be used to explore ‘metness of need’—that is, the extent to which individual needs were met on a case-by-case level. Figure 2 summarises the proportions of individual met and unmet needs across the 15 NPCS items. In the Health and person care domain, less than 30% of cases had unmet needs for medical and nursing care, but over half of the respondents had unmet needs for therapy—both in terms of the number of disciplines required and the intensity of input. Owing to the severe and complex nature of their disabilities, work was not an option for 60% of this group. However, of the 84 (40%) who required vocational rehabilitation, only 10 (12%) had their needs addressed, leaving 88% (or 35% overall) with unmet vocational needs.
{kind=link}
{kind=link}
This bar chart illustrates ‘metness of need’, that is, the proportion of individuals who had needs identified in each item of the Needs and Provision Complexity Scale at discharge from inpatient rehabilitation, and the proportions who did and did not have their needs met.
In the Social care and support domain, more than half of the patients (56%) had unmet needs for social worker/case management support. A relatively small proportion of this sample reported needs for respite and advocacy support (<30%), but again, few of these had their needs met. Only 22% reported unmet accommodation needs, but 40% had unmet equipment needs.
Cost implications
To inform the likely costs of addressing these gaps in service provision, we analysed the NPCS-estimated costs of needs versus current provision. For comparative purposes, all costs are computed as costs/patient/annum.
To confirm that the 211 respondents were representative of the whole recruited sample in this respect, we first compared the NPCS-estimated costs of health and social care needs at discharge between those who did (n=211) and did not (n=217) respond at 6 months. No significant differences were found in any of the domains or subscales. The costs of need for personal care (which includes formal and informal care) made up the largest proportion of costs (£22 988 (43%)) within the community care setting. This is unsurprising and is consistent with both the CSRI data from this sample9 and also with costing data from the other studies.13
Table 4 summarises the comparative costs of needs identified at discharge compared with the cost of services provided, as estimated by the NPCS costing algorithm. The results mirror the findings from analysis of the ordinal NPCS scale—namely that the costs of Rehabilitation, Social support and Equipment provided in the community are significantly less than predicted—while the costs of personal care provided are much greater than predicted. However, owing to the relatively high cost of personal care, our cost analysis reveals that the mean underspend on Rehabilitation and Social support (£4110 in total) is exceeded some 3.5-fold by the above-predicted expense of Personal care (borne mainly by families), and the cost of residential accommodation or adaptations to the existing accommodation (£14 559 in total).
Comparison of NPCS-estimated mean per annum costs for ‘Needs’ (predicted at discharge) versus ‘Gets’ (the cost of services provided) at 6 months postdischarge (n=211)
Discussion
In this first analysis of needs and provision using the NPCS, we examined the extent to which health and social care needs (as assessed by the clinicians at discharge from inpatient rehabilitation) were and were not met during the first 6 months in the community (as reported by patients and their carers). The NPCS demonstrated significant gaps between needs and service provision, especially with respect to ongoing community rehabilitation, equipment and social support. By contrast, needs for medical and nursing care were relatively well met, and provision of personal care was higher than predicted.
There are a number of possible explanations for lower than predicted levels of service provision. The levels of need might have reduced over that period, leading to a corresponding reduction in service provision. Against this, however, were the static or slightly deteriorating levels of dependency, carer burden and community integration, which suggested that the group had ongoing needs for health and social support. Alternatively, respondents may have been unable to recall all the services received, or they may have failed to understand that they were being asked to consider service provision over the whole 6-month period. The systems in place to ensure full capture of services provided were (1) recording of the maximum level, if input had varied, (2) checking of questionnaires with follow-up telephone interviews to clarify any missing or ambiguous responses, (3) parallel recording of the CSRI. Moreover, the differential findings of ‘overprovision’ and ‘underprovision’ in the different domains of the scale also suggest that the reported deficits were not simply due to a misunderstanding of the questionnaire or lack of recall.
Similarly, there are several possible explanations for the higher than predicted levels of personal care provision. It could suggest a deterioration of motivation for independence outside the intensive rehabilitation environment with greater reliance on carer support; an overprotective attitude on the part of families and carers; or a failure on the part of the discharging clinicians to appreciate the true extent of care needs in the home environment. The latter possibility is unlikely as many of these patients were on graded discharge programmes prior to discharge, so their needs for care in the home environment were generally well understood.
Putting together the above findings, we believe that a more likely explanation is that the prediction of care requirements made by professionals at discharge was based on the assumption that appropriate ongoing rehabilitation, equipment and social support would be provided and, in the absence of these commodities, patients remained more dependent on others to meet their care needs.
The NPCS also provides useful insights into the relative cost implications of failing to provide the required level of ongoing support. The NPCS-estimated cost of providing for increased personal care and accommodation requirements was 3.5 times more than the underspend on rehabilitation and social support. The figures suggest that the potential sums that commissioners ‘save’ by not investing adequately in rehabilitation and support are exceeded by the additional costs of personal care and institutional care, to the tune of over £10 000/patient/annum. However, these findings must not be interpreted as an opportunity for disinvestment. Despite repeated calls for joined-up health and social care commissioning,20 these remain segregated in most parts of the UK at the current time—so that savings in the cost of housing and social support do not readily translate into extra funding being available for rehabilitation and other healthcare services. More importantly, the physical and financial burden of caring for people with LTNCs falls largely on their families and informal carers (80% in this study). So it is the patients/families who currently bear the brunt of those extra care costs, rather than the State.
Strengths and limitations
-
Despite our conscientious efforts to trace patients, just under half (49%) of the original recruited sample provided NPCS-Gets data to compare with identified needs. Given the itinerant nature of this population and the difficulty that many patients with complex disability have in completing questionnaires,21 this low response rate is not unexpected. The demographic and baseline characteristics of the respondents and non-respondents were shown to be similar, suggesting that our findings are representative of the whole cohort, but the possibility of sample bias cannot be excluded.
-
The NPCS is a relatively new tool. The psychometric evaluation12 was undertaken using data from the same cohort sample that is presented here. This has the advantage of providing direct evidence of the tool's performance in the very sample under investigation. However, the NPCS requires further testing in different populations before it may be considered to be fully robust.
-
The costing algorithm, in particular, requires further testing and refinement. The costing assumptions were developed by professionals with specific experience in managing patients with LTnC. They require further testing in other populations and settings, and would need to be translated for use in other countries.
-
The study design tends to assume that needs for (and provision of) services remain static over 6 months. This time frame was chosen for a sample of patients with complex neurological disability whose needs were not expected to change rapidly (as supported by the lack of change in dependency, carer burden and community integration). However, a formal re-evaluation of needs at 6 months would have strengthened the findings. The time-points for future evaluations will depend on the expected trajectory for change in the population under study.
-
Other authors have highlighted the need to take into account both user and professional perspectives on met and unmet needs.22 The NPCS was originally designed as a framework for recording of information by clinicians in the context of integrated care planning. While this study demonstrates the feasibility of capturing user perspectives through the self-complete questionnaire and follow telephone interviews, it did not capture professional perspectives at 6 months, and nor did it allow for simultaneous reassessment of ongoing need. A combination of patient and clinician completion of the NPCS in the course of case review/planning meetings may provide better capture of both viewpoints in future evaluations, but has resource implications for research if these are not conducted as part of routine practice.
-
Finally, the multicentre cohort was drawn from the nine tertiary specialist brain injury services in London. This sample was deliberately chosen to yield a study population with complex needs for ongoing community-based support, but the findings are limited to one geographic region in the UK and might not be generalisable to other settings.
Our findings resonate, however, with those generated by other researchers. Following the publication of the NSF for LTnC, the UK Department of Health funded a substantial research initiative to support implementation which has recently been published.23 Nationwide surveys by Fitzpatrick et al24 and Jackson and colleagues13 ,25 report that the majority of respondents were able to access the requisite healthcare (medical and nursing), but satisfaction was generally low in respect of the coordination of services and rehabilitation inputs were hard to identify.24 Respondents also reported difficulty in accessing support for personal care,24 carer support24 and respite services25—and lengthy waits for equipment and adaptations were also commonplace.26 Reports from elsewhere in the world27 ,28 similarly echo the experience that much of the burden of caring for people with neurological disability falls on family and informal carers with inadequate support and recognition from health and social care providers. However, the NPCS offers the opportunity to evaluate service provision (including rehabilitation), specifically in relation to individual needs, and to explore the potential cost implications of providing the required inputs.
Placed in the context of this wider research, therefore, we conclude that the NPCS represents a simple but useful tool, which has the potential to inform both clinical decision-making at the individual level, and also population-based service planning and delivery for patients with complex disabilities. Although it was developed in the context of LTnC, the tool is not impairment-specific and may well have application in other long-term conditions, but the costing algorithm is likely to require adjustment for different contexts. Its further use and exploration is now warranted.
Acknowledgments
The authors gratefully acknowledge the hard work of the clinical teams in the nine centres, and of the patients and their families who participated in the follow-up survey. Special thanks are due to Helena Morris, Sasha Wade, Bernadette Khoshaba, Christine O'Connell, Amanda Fahy, Iris Molosankwe, Ralph Crook and Ali Price for their roles in data collection and administrative support for the project. Statistical advice was provided by Paul Bassett, Statsconsultancy Ltd. We are particularly indebted to Lesley Curtis, Personal Social Services Research Unit, Kent University for her assistance with costings for the NPCS algorithm. Also to the members of the LTnC Dataset Development Group who were involved in original development of the NPCS, in particular Maggie Campbell, Richard Grünewald, Richard Hills, Beverley Hopcutt, Nicola Russell and Barrie White who were instrumental in its early development and testing.
References
Footnotes
Contributors LTS led the development of the NPCS and its costing algorithm. She was the lead clinician for the NIHR-Funded project that sourced the data presented here. She led the design of the study, performed the analyses and wrote the first draft of the article. RJS was the principal investigator for the larger study of which this formed a part. He took the lead role in execution and governance of the study and was responsible for the psychometric evaluation of the NPCS. PJM provided health economic advice and expertise. DMJ was responsible for data-checking and quality. All three coauthors reviewed and commented on the manuscript.
Funding This article presents independent research commissioned by the National Institute for Health Research (NIHR) under its Health Research Health Services and Delivery Research (NIHR HS&DR) programme (project number 08/1809/235). Please visit the HS&DR website for more information. The views expressed in this article are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. Financial support for the preparation of this manuscript was also provided by the Dunhill Medical Trust and the Luff Foundation.
Competing interests Outcome measurement is a specific research interest of our centre. LTS was the lead developer of the NPCS, but neither she nor her employing institution has any financial interest in the tool which is disseminated free of charge. None of the authors has any personal financial interests in the work undertaken or the findings reported. All authors are employed by universities/hospitals which may cite this article as part of their research evaluation processes, including the UK Research Excellence Framework 2013. LTS and RJS have received financial support from the NIHR to attend conferences to disseminate the submitted work. We do not consider that any of these relationships or activities have influenced the submitted work.
Copies of the Needs and Provision Complexity Scale are available free of charge from the website14 and copies of the full questionnaire and other tools used in this study are available from the corresponding author.
Patient consent Obtained.
Ethics approval Approval for the study was granted by Bromley Research Ethics Committee (Ref no: 09/H0805/25) and subsequently by the R&D centres of the seven participating NHS trusts. The remaining two recruiting centres were in the independent sector—approval for recruitment was obtained through their internal clinical and research governance processes.
Provenance and peer review Not commissioned; externally peer reviewed.
Registration The study was registered with the NIHR Comprehensive Local Research Network: ID number 7503.
Data sharing statement No additional data are available.