Article Text

Abstract
Introduction Chronic lower back pain (CLBP) is a frequent cause of medical consultations worldwide, and it results in decreased quality of life and disability. Current treatments for CLBP are often not effective, and alternatives are urgently needed. Three promising possibilities have emerged: (1) open-label placebo treatment reduces chronic pain, (2) placebo treatment is as efficacious as opioid treatment with a high correlation between patient expectation and treatment outcome, and (3) observing positive effects in another patient can improve functional capacity. We hypothesise that treatment expectations can be positively influenced through social observation and improve treatment outcome.
Methods and analysis In our clinical trial, we will randomise patients with CLBP into five groups. Two groups receive either a 3 week course of treatment with an analgesic (ANA) (metamizole/dipyrone) or with open-label placebos (OLP). For one of each group, we will build treatment expectations through observational learning and assess its impact on the treatment. For this purpose, one group each will watch either a positive or a neutral video. The intervention groups will be compared with a control group that will not be given any medication or observational learning. Participants will be recruited via all institutions in the Hamburg metropolitan area that treat patients with CLBP. Patients are eligible for inclusion if they are at least 18 years or older, have CLBP (of at least 3 months duration), and agree to potentially receive an active ANA or an OLP. Patients with pain-related “red flags” will be excluded. The study requires 150 participants (30 participants per group) to assess the differences in the primary outcome, pain intensity. Secondary outcomes include changes in treatment expectations, anxiety, comorbid depression, stress-related neuroendocrine measures, functional and structural connectivity, functional capacity, and ANA consumption. All outcomes and treatment expectations will be measured before and after the intervention and 3 months post-intervention.
Ethics and dissemination Ethical approval was obtained in January 2020 from the Hamburg Medical Ethics Council (ref number PV7067). Outcomes will be disseminated through publications in peer-reviewed journals and presentations at national and international conference meetings.
Trial registration number The approved trial protocol was registered at the German Clinical Trials Register (DRKS) and can be found at drks.de (Identifier: DRKS00024418).
- pain management
- back pain
- clinical pharmacology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This randomised trial will investigate an innovative approach to treat patients with chronic lower back pain.
A randomised controlled design will be implemented to evaluate the effect of expectations on the efficacy of analgesics (ANAs) and open label placebos (OLPs) in combination with observational learning.
This is the first clinical study that will evaluate the influence of expectations on perceived efficacy of ANAs and OLPs in one study design.
The study design does not allow blinding of the therapist throughout the entire study.
Introduction
Background
Back pain is one of the most frequent reasons for medical consultations worldwide,1–5 and it is a global concern. Lower back pain is the most common complaints, and it can be acute or chronic. Back pain is regarded as chronic (chronic lower back pain; CLBP) if the pain lasts more than 12 weeks.6 It increases with age, and it is prevalent in 19.6% of women and men between the ages of 20 and 59.7 CLBP results in decreased quality of life, can lead to disability and is a financial burden for patients and communities.8 Hence, effective treatment of CLBP is crucial and highly relevant. Unfortunately, current treatment options are unsatisfactory. Despite considerable efforts to improve CLBP, common front-line pharmacological therapies are often not significantly more effective than placebos.9 10 Despite the unsatisfactory effect of analgesics (ANAs), CLBP is often treated solely with medication. However, the (long-term) consumption of ANAs, especially opioids, can lead to severe side effects and addiction, as it is currently being witnessed with the so-called ‘opioid crisis’.11 This lack of effective drug treatment partially explains the rising numbers of surgical and other interventional procedures in patients who undergo CLBP, despite little evidence of the long-term benefits.12 National guidelines for the treatment of CLBP13 recommend an interdisciplinary multimodal pain treatment approach, which is often also ineffective10 and is only available to a limited number of patients because few institutions offer this intensive treatment. CLBP should be treated with a multimodal management strategy that includes the bio–psycho–social perspective.14 Alternative treatment strategies are urgently required, and current research findings regarding cognitive pain modulation should be exploited.15
Treatment expectations
One possibility for the inclusion of the bio–psycho–social perspective to go beyond a pharmacological approach to enhance the treatment effect is to integrate psychological mechanisms into CLBP treatment and to increase patient involvement in the treatment. A novel approach is to exploit the effect of treatment expectancy.16–21 Positive expectations can enhance the treatment effect and play a key role in placebo effects.9 Negative expectations can impair treatment effects and are relevant to the nocebo effect. For example, it has been shown that the expectation of impending pain substantially alters our perception of pain. Expectation of pain can turn an otherwise non-painful sensation to a painful experience22 or substantially reduce or even block pain altogether.9 23 24 Experimental studies suggest that positive expectations can modulate the perception and neural processing of pain and the response to placebos and active drugs. Hence, more systematic exploitation of the mechanisms and effects of expectations is necessary to improve the efficacy of treatment in clinical populations. Therefore, harnessing expectations in a therapeutic way might be promising to improve treatment for patients with CLBP in a safe and cost-effective way.25 26
So far, most evidence for the striking effect of expectations has come from experimental studies with healthy volunteers and not from studies that include patients with chronic pain. However, the desire for pain relief might be different for patients with chronic pain than for healthy volunteers. Therefore, a study that systematically investigates how to exploit the placebo effects is highly relevant.
Influence of treatment expectation on active drug treatment
Treatment expectation can enhance the effect of both placebos and active drugs.27 Clinical and experimental evidence indicates that expectation can substantially modulate the efficacy and tolerability of active medical treatment, including pharmacotherapy.27 Positive treatment expectation has been shown, for instance, to double the ANA effect of the opioid remifentanil28 and to substantially enhance the effect of the acute antimigraine drug rizatriptane.29 Up to 50% of the response to ANAs can be attributed to expectation and not to the pharmacodynamic effect of the administered drug.30 31 Similar effects have been reported for other medications, including psychotropic drugs.27 32 The influence of the expectation of treatment outcome is not limited to pharmacological interventions. Positive expectations also affect outcomes in multimodal treatment programmes for chronic pain,33 the effect of deep brain stimulation on motor performance in Parkinson’s disease27 and the outcome of surgical procedures.34 35 Until now, the influence of expectations on active drugs has mainly been tested in experimental studies on healthy volunteers. The extent to which the effect of the medication for the treatment of chronic back pain can be influenced by expectancy manipulation has not yet been investigated. Pain medication recommended in the treatment guidelines for back pain is suitable for this purpose. Expectation manipulation to enhance active drug treatment in clinical samples is, therefore, a pivotal next step to advance the systematic use of treatment expectation in clinical practice.
Open label placebos
Classic clinical controlled placebo trials imply that patients receive the placebos deceptively, which means that patients do not know whether they receive active or inactive medication. This approach is possible and reasonable in trials because patients consent to the possibility of receiving a placebo instead of the active medication. However, in daily clinical practice, this is not ethically acceptable. One way to avoid this dilemma is to administer the placebo openly (open label placebo; OLP) so that the patients are aware of what they are taking.36 37 Recent research has revealed that patients with CLBP have shown a clinically relevant response, even when they were aware that they were taking a placebo.36 38 Initial studies showed that the administration of OLPs lead to significant improved effects over the usual treatment in regard to pain and disability and are well accepted by the patients.36 37 39 Patients are openly told that they are receiving a placebo and are informed about the underlying mechanisms of placebo effects. Treatment expectation might be the underlying mechanism for the effectiveness of OLPs. Therefore, the effect could be enhanced by using the mechanisms underlying treatment expectation, which are, for example, conditioning or observational learning.40 This systematic modulation of expectation could boost treatment effect and, in particular, enhance treatment for previously inadequate pain relief.41
Observational learning
Treatment expectation is generally formed in various ways, including conditioning via prior experiences,42 43 therapeutic context, observational learning40 44 45 and verbal suggestions via instructions.9 29 Furthermore, pain is influenced by social interaction and can be modulated by observing others.44 46 Initial studies confirm that this effect can be achieved through the observation of the benefits of treatment in others.40 47 However, these studies were conducted with healthy participants under laboratory conditions, meaning that the pain was induced, and the participants did not suffer from chronic pain. One study with patients with chronic pain has revealed that intentional observational learning has an effect on disability in patients with CLBP.48 However, especially for patients with chronic pain, further research is required because there are frequent changes in treatment expectations due to the circumstance that patients continuously interact with other patients, healthcare providers and personal acquaintances. However, in clinical practice, a model patient who demonstrates the advantages of an intervention is not always available. Therefore, it is important to evaluate whether prerecorded videos of patients who have benefitted from a treatment can alter treatment expectations and enhance treatment effects.
Objectives and outcome
Primary objective
The primary objective of this study is to evaluate whether observational learning enhances positive treatment expectations and whether the positive expectations improve the treatment outcome of OLPs or active ANAs in patients with CLBP in comparison to the usual treatment. We will randomise patients with CLBP to either a 3-week treatment with an ANA, metamizole or a 3-week treatment with OLPs. We will build treatment expectations through observational learning and assess the impact on the two groups. For this purpose, patients will watch either a positive or a neutral video. We will assess the patients’ treatment expectations before and after 3 weeks and again after 3 months, and we will evaluate the effect of this expectation on subjective and objective outcome measures.
The primary subjective outcome is the intensity of the CLBP after 3 weeks of treatment on a Numeric Rating Scale (NRS) 0–10 (0=no pain; 10=worst pain imaginable). A composite pain intensity score (mean of minimum, maximum and average pain intensity) will be assessed at baseline and 3 weeks after the baseline on a NRS 0–10. This well-established outcome measure has also been used in the two existing studies of OLP treatments for CLBP and will allow comparing the results.36 39 We hypothesise that observational learning enhances positive treatment expectations and that positive expectations improve treatment outcome, so both groups that received positive reinforcement through the positive video should experience more satisfactory outcomes from the treatment than those who saw the neutral videos.
Secondary objectives
A secondary objective is to determine whether positive expectations and ANA treatment effects combine in an additive or synergistic manner. We hypothesise that the group receiving the positive reinforcement will have better outcomes than the group receiving no positive reinforcement. In addition, we will investigate whether individual trait and state variables such as anxiety, comorbid depression and stress-related neuroendocrine measures modulate treatment expectancy and consequently the effect of this on treatment outcome. Moreover, another aim is to gain insight into whether the functional and structural connectivity of the prefrontal cortex with the pain-related regions at rest predicts the effects of expectation on ANA treatment outcome. This will be investigated through resting state functional (rsf) MRI and diffusion tensor imaging (DTI).
Consequently, the secondary outcomes consist of subjective and objective outcome measures. Subjective outcome measures will be the patients’ self-ratings. Whereas, the objective outcome measures will be functional capacity, neuroendocrine measures and functional and structural connectivity of the prefrontal cortex. Subjective and objective outcome measures are described in detail in the paragraph titled ‘Outcome Measures’.
Methods and analysis
Setting
The study will be part of a collaborative research centre (CRC) project (SFB 289). Therefore, some of the tests will be analysed across all participating projects. This study will be conducted at the University Medical Centre Hamburg-Eppendorf, Germany.
Study aim
The proposed study will evaluate the expectations and effects of OLPs in contrast to active ANAs for the treatment of CLBP. The following are the proposed key questions.
Research aims in the present study are:
Can the effect of treatment expectation on pain be enhanced by observational learning?
Does positive treatment expectation enhance the ANA effects of treatment (main effect of expectation)?
Do the effects of positive expectation and pharmacological treatment combine in an additive or multiplicative (synergistic) manner?
Does the impact of treatment expectation on ANA treatment outcome differ between subjective (pain, perceived limitation in mobility) and behavioural (functional capacity) outcome measures?
Research aims in the present study that are also analysed as part of other projects within the SFB 289/CRC are:
Do individual trait and state variables such as anxiety, comorbid depression and stress-related neuroendocrine measures modulate the effect of treatment expectancy on treatment outcome?
Does the functional and structural connectivity of the prefrontal cortex with pain-related regions at rest predict expectation effects on ANAs treatment outcome?
Do salivary cortisol awakening response and salivary alpha-amylase predict expectations effects on ANAs treatment outcome?
Patient and public involvement
Patients should benefit from clinical studies, and this has been a priority for this project from the outset. The study grew out of the authors’ clinical activity and therapy expertise with chronic pain patients. Therefore, the patients were already involved in the planning phase and were asked whether they would accept the study design, the deception condition and what information they considered necessary to understand the procedure. The patients were able to provide valuable input. We discussed the study in an interview with the chairperson of the German pain organisation ‘UVSD SchmerzLOS’ (independent association of active patients with pain in Germany, ‘Painless’). The ‘UVSD SchmerzLOS’ has also published an interview that introduces the main aspects of the clinical applications of placebo effects in their journal.
The production of the videos for the observational learning for the treatment (ANA or OLP) effects is of high importance for our study. We based the video script on the medical history of one of our patients with CLBP and hired a professional actor to perform in it. We carefully investigated satisfaction with the videos of patients with CLBP and distributed materials by interviewing patients who were not later enrolled in the study. In addition, patients will be asked for in-depth feedback on the materials and study design after their participation in the study. When the results of the study are published, they will be sent to all patients who provided written consent.
Target population
Participants will be eligible or not eligible for the study according to the following criteria:
Inclusion criteria
Age≥18 years.
Primary symptom CLBP (ICD-10).49
Average pain intensity≥4/10 on NRS during past week.
Sufficient fluency in German language to understand and respond in German language and questionnaires.
Exclusion criteria
Severe acute or chronic mental health condition (eg, psychosis).
Chronic diseases with a dominant role in disability (eg, rheumatic disorders, cancer, severe heart diseases).
Pain-relevant ‘red flags’6 (eg, tumour, active rheumatologic disorder).
Inflammatory or neuropathic back pain.
Unstable ANA medication—dose and frequency of ANA treatment should be stable for 3 weeks prior to screening.
Regular intake of metamizole (dipyrone).
Known allergies or other contraindications for metamizole (dipyrone).
Pregnancy and breast feeding.
Notably, if patients are not eligible to participate in the MRI scanning, they will not be excluded from participation for the study itself.
Recruitment
Participants will be recruited via general practitioners, specialised institutions for back pain, orthopaedic surgeons, physiotherapists, pain therapists and all institutions in the Hamburg metropolitan area that treat patients with CLBP.
Relevant contact partners in Hamburg, Germany, will be contacted and informed about the study. They will receive a checklist to be able to do fast screening of the inclusion and exclusion criteria. Thereafter, potential participants will receive a flyer with all the relevant information and contact addresses. After the study team receives the contact information of potential participants, the study physician will assess the inclusion and exclusion criteria.
Study design
This study is based on a fully balanced within-subject and between-subject placebo study design (figure 1). Treatment outcome will be assessed at the subjective (pain rating, limitation in mobility) and objective behavioural (functional capacity) levels. For this purpose, active ANA, OLP and expectation (positive=high vs neutral=low) will be fully crossed. In addition, a control group (natural history; NH) will complement the design. The NH group will receive no intervention (no treatment, no videos). Treatment expectation (high/low) will be induced through observational learning of treatment benefits in a standardised video showing either positive or neutral treatment effects in another patient.
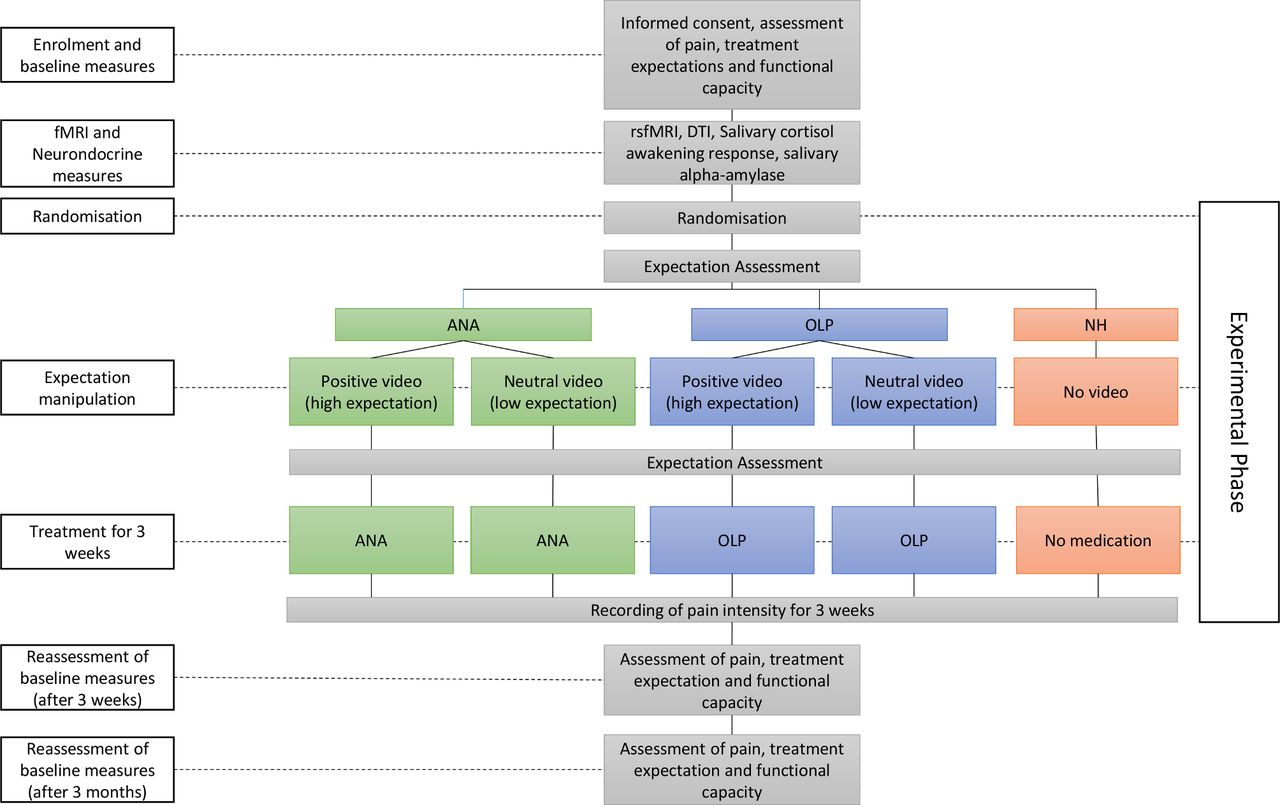
Study design. ANA, analgesic; DTI, diffusion tensor imaging; NH, natural history; OLP, open label placebo; rsFMRI, resting state functional MRI.
The study includes three visits over the course of 3 months, including a follow-up after 3 months. The baseline assessment of pain includes perceived limitation in functional capacity, treatment expectation and further psychological assessment. If patients meet the inclusion criteria, they will be fully informed about the study and asked to provide written informed consent. All patients will be reminded to continue with their usual care (eg, current medication), and they will be informed that they will be randomised to receive either an approved and widely used non-opioid ANA or a placebo, or they will be assigned to the control group. Participants will also be informed that both the active ANA and the placebo have shown beneficial effects for CLBP in previous studies, with varying responses between individuals.36 39
After providing written consent, participants will complete a questionnaire and do certain physical exercises to assess baseline values. To assess and analyse predicting variables, patients will undergo rsfMRI scanning, 3D-MPRage T1-weighted sequence (T1), DTI and neuroendocrine measures (salivary cortisol awakening response and salivary alpha-amylase) at rest within 1 week after enrolment in the study. After the baseline assessment, patients will be randomly allocated to one of the five study groups. Participants will be randomised using block randomisation stratified by gender (ratio 1:1) to allocate the participants to one of the five study arms (ANA/high, ANA/low, OLP/high, OLP/low and NH). A member of staff who will not be involved in the trial will prepare sealed envelopes.
Once the study psychologist has obtained informed consent and baseline data regarding medical background, pain and physical capacity, participants can choose a random sealed envelope, and the intervention and treatment will commence accordingly.
Before the corresponding medical treatment is started, participants will undergo a treatment expectation modulation by watching a brief (10 min) video that is part of the general standardised study information. Alterations in treatment expectation will be assessed immediately after the intervention. On the following day, patients will start their treatment (ANA or OLP) at home. The NH group will be assessed in the same manner as the four experimental groups, but they will not undergo modulation of expectancy (video) or receive ANA treatment (ANA or OLP). Participants in the NH group will be offered ANA or OLP after completion of the main observation period (3 months) and after participating in the study.
In addition to the treatment, patients will be given a pain diary and questionnaires to complete within the 3 week phase. Patients will be contacted once a week and encouraged to update their pain diaries. At the follow-up sessions (at 3 weeks and 3 months), the assessment tools used for the baseline assessment will be repeated. Participants will be contacted to remind them of their appointments.
Blinding
The researcher conducting the primary data analysis will be blinded to group allocation. Due to the nature of the study, the researcher conducting the intervention will not be blinded to group allocation. Therefore, the possibility of an experimenter effect cannot completely be excluded but should be minimised due to the study design.
Intervention
After providing written informed consent for participation in the study and the fMRI scanning, the participants will be randomly assigned to one of the five study groups and receive treatment-specific information that is largely similar for the ANA and OLP treatment (figure 2).

{kind=link}
{kind=link}
Treatment information. ANA, analgesic; OLP, open label placebo; NH, natural history.
Video-based treatment expectation manipulation
On randomisation to the study medication and the substance-specific/adjusted verbal information, patients will be asked to carefully watch a 10 min video that will be introduced as part of the general standardised study information. Patients in the high expectation groups will watch a video in which an actor introduced as a fellow patient describes and demonstrates the improvement in their back pain and pain-related functional impairments, following ANA or OLP treatment. In the first part of the video, the patient executes a number of different movements with visible signs of discomfort (pretreatment). In the second part, the same movements are repeated, but the patients shows no signs of discomfort (posttreatment). The videos are identical except for the treatment, which will be either an ANA or an OLP. Participants in the neutral expectation groups, ‘OLP/low expectation’ and ‘ANA/low expectation’, will watch a control video of the same length, in which the same actor will provide neutral information regarding CLBP without any reference to the course of treatment. The age of the fellow patient is approximately 60 years, which best reflects the mean age of this patient group.39
Treatment: active ANA versus OLP
The non-opioid metamizole (dipyrone) will be used for the active ANA treatment, as it is generally well-tolerated and has no known central nervous system side effects that could interfere with treatment expectation. According to the guidelines,50 51 metamizole (dipyrone) can be used to treat CLBP at the lowest effective dose and for as short a duration as possible when non-steroidal anti-inflammatory drugs are contraindicated or not effective, which applies to the majority of patients with CLBP who present at tertiary referral centres such a university clinic. Metamizole (dipyrone) and OLP will be provided as film-coated tablets with an identical appearance. Patients randomised to the ANA group will receive 3×2 tablets (=3000 mg), and the OLP groups will receive the same number of placebo tablets. The NH group will receive no treatment other than the medication already prescribed before the trial. To rule out the possibility of agranulocytosis, blood samples will be taken from all patients before the study and after the 3-week intervention.
Outcome measures
Treatment outcome will be assessed at the subjective (pain rating, perceived limitation in mobility) and observed (physical capacity) levels 3 weeks and 3 months after randomization and compared with the baseline assessment. The following variables will be recorded (table 1).
Outcome measures
Sample size calculations
Our previous studies have shown large to even larger effects from placebo interventions in patients with CLBP with similar paradigms, d=1.8338 and d=1.56.9 Furthermore, the existing OLP studies in patients with back pain have revealed lower, but still substantial, effects on pain and reported disability with d=0.4439 and d=0.76.36 Accordingly, we expect a difference in the effect on primary outcome (pain intensity) between high and low expectation conditions, and this difference is expected to exceed an effect size of Cohen’s d=0.40. This effect should be shown for at least the pre–post comparison. The corresponding power analysis was based on F statistics for the calculation of analyses of variance (ANOVA) with repeated measures (interaction effect of within and between factor, effect sizes of d=0.4, α=0.05, power 1-ß=0.9, 5 groups, 2 assessments with G*Power).52 This requires 125 participants, and with consideration of the expected drop-out rates, a cell size of 30 participants (N=150) per group is considered sufficient.
Statistical analysis
Between and within differences in clinical outcomes and group allocation will be studied for the different outcome measures with ANOVA tests. The data will be analysed as intention to treat by a researcher blinded to group allocation. Exploratory post hoc analysis will be applied in the event that significant main results are found. The analyses will be performed with IBM SPSS Statistics software V.27.0 (IBM Corp) and data will be reported as means with 95% CIs, unless otherwise specified. Greenhouse-Geisser or Huynh-Feldt correction for the F test will be used to adjust the df for deviation from sphericity, if necessary. For all performed analyses, two-sided P values of p<0.05 will be considered statistically significant.
Outlook and perspective
CLBP is highly prevalent, and it is a major cause of decreased quality of life and disability. The number of prescriptions for opioid medications for CLBP has increased dramatically.10 This trend has been accompanied by significantly increased levels of prescription opioid overdoses, abuse, addiction and diversion.10 Therefore, strategies that exploit the potential of expectation to enhance ANA treatment outcomes are urgently needed. If the observation of treatment benefits prove to enhance the response to OLP and/or active ANA treatment, this could have fundamental implications for routine clinical care, as it may be used as an ethically acceptable53 and cost-effective add-on or an alternative to current treatment modalities. The balanced placebo design used in this study will also shed light on the as yet unexplored question of whether the effects of expectation and of the drug combine in an additive or multiplicative manner. The insights gained in this study will pave the way for future studies that evaluate whether and how these results generalise to other (chronic) pain conditions and ANA treatments. The thorough clinical and psychological assessment in combination with brain imaging (rsfMRI, DTI, T1) and neuroendocrine measures also promises to identify subgroups of patients who are particularly likely to benefit from such interventions and can be systematically targeted in defined patient subgroups in future studies. The brain imaging performed in this study can lay the foundation for not only identifying predictors but also the mechanisms underlying the beneficial effects of expectation in patients in future funding periods, as these may differ fundamentally from those in healthy volunteers.
Ethics and dissemination
The study has been approved by the Hamburg Medical Ethics Council. The results of this trial will be reported in relevant academic journals and conferences.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors RK and JS jointly wrote the manuscript. RK, JS, MS and TF designed the study design. MS and CZ critically reviewed the manuscript and provided important intellectual content. RK obtained funding and supervised the whole study.
Funding The work is funded by the Deutsche Forschungsgemeinschaft (German Research Foundation)—Project-ID 422744262—TRR 289.
Disclaimer The funder played no role in the study design, in the collection, analysis or interpretation of the data, in the writing of the paper or in the decision to submit the article for publication.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.