Article Text

Abstract
Objective To identify and characterise activities for deprescribing used in general practice and to map the identified activities to pioneering principles of deprescribing.
Setting Primary care.
Data sources Medline, EMBASE (Ovid), CINAHL, Australian New Zealand Clinical Trials Registry (ANZCTR), Clinicaltrials.gov, ISRCTN registry, OpenGrey, Annals of Family Medicine, BMC Family Practice, Family Practice and British Journal of General Practice (BJGP) from inception to the end of June 2021.
Study selection Included studies were original research (randomised controlled trial, quasi-experimental, cohort study, qualitative and case studies), protocol papers and protocol registrations.
Data extraction Screening and data extraction was completed by one reviewer; 10% of the studies were independently reviewed by a second reviewer. Coding of full-text articles in NVivo was conducted and mapped to five deprescribing principles.
Results Fifty studies were included. The most frequently used activities were identification of appropriate patients for deprescribing (76%), patient education (50%), general practitioners (GP) education (48%), and development and use of a tapering schedule (38%). Six activities did not align with the five deprescribing principles. As such, two principles (engage practice staff in education and appropriate identification of patients, and provide feedback to staff about deprescribing occurrences within the practice) were added.
Conclusion Activities and guiding principles for deprescribing should be paired together to provide an accessible and comprehensive guide to deprescribing by GPs. The addition of two principles suggests that practice staff and practice management teams may play an instrumental role in sustaining deprescribing processes within clinical practice. Future research is required to determine the most of effective activities to use within each principle and by whom.
- clinical pharmacology
- protocols & guidelines
- primary care
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The datasets used and/or analysed during the current study are included in the article and as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
First study to investigate deprescribing activities in general practice.
First study to map deprescribing activities to guiding principles.
This study used a robust, up-to-date and comprehensive search strategy.
Critical appraisal of studies was not conducted.
Effectiveness and outcomes of the identified activities were not examined.
Introduction
The WHO estimates that half of all medicines prescribed worldwide are done so inappropriately.1 ‘Inappropriate medication use (IMU)’ can occur when medications are prescribed and taken despite there being no clinical benefit or the risk of taking a medication outweighs the benefit.2 IMU is often linked with polypharmacy where patients with multiple health issues are prescribed multiple medications, placing them at increased risk of adverse reactions and interactions.3 It is estimated that 20%–30% of the general population experience harmful events due to IMU and polypharmacy resulting in hospitalisation and increased risk of mortality.4 5Deprescribing (‘the planned and supervised process of dose reduction or stopping unnecessary or potentially harmful medication’)6 is a recommended component of best practice prescribing which can address the issues of IMU and polypharmacy. Both prescribing and deprescribing require skilful and careful clinical judgement to balance the risks and benefits of medicines, minimising potential harms and improving patient health outcomes.7 General practitioners (GPs) prescribe the majority of medications8 and are well placed to conduct the majority of deprescribing. However, deprescribing is not routinely occurring in clinical practice.7 9
Evidence suggests that patients are willing to cease unnecessary medications but require empowerment and engagement from their GP to do so and are likely to leave it to their GP to initiate the deprescribing conversation.10 However, research has identified a number of barriers to this occurring, including appointment time constraints, lack of good quality guidelines,9 clinical inertia11 and not knowing when to deprescribe.12 When asked about what would assist with their deprescribing role, GPs express a desire to have support and work in collaboration with other healthcare professionals,9 have ready access to non-pharmacological options and resources, and decision-making systems and tools13 to enable them to regularly and confidently conduct deprescribing.
Activities to support GPs to deprescribe have been investigated, although only one systematic review has focused on deprescribing by GPs in primary care. This review by Dills et al14 found three effective activities for successful deprescribing: (1) pharmacist–physician collaboration for conducting medication reviews; (2) giving clinicians intensive education about deprescribing; and (3) providing individual patients with information about chronic disease management and IMU (eg, pharmacological and lifestyle advice and alternative options for treatment).14 Most of the included studies were set in long-term care, assisted living and outpatients, which are commonly considered to fall outside the definition of primary care. Further, only 6 of the 58 studies were conducted in general practice. Although GPs do practise in these settings, the effectiveness of the identified activities may not be generalisable to GPs practising specifically within the general practice setting.
Isenor et al15 recently explored deprescribing activities in primary care, which included pharmacy, general practice and allied health. Results of this scoping review revealed that checklists, algorithms, leaflets, patient finder tools, goal setting tools, and prompts or cues in the form of reports, letters, posters or electronic medical record alerts were most frequently used to support deprescribing. These activities were often used in conjunction to form interventions to change GP and patient behaviour. This suggests that deprescribing interventions are multifaceted and employ a variety of techniques to encourage deprescribing at the patient, clinician and systems levels.13 Results showed that GPs were the most targeted healthcare professional for intervention, with pharmacists most commonly conducting the deprescribing process. Although pharmacists may play an important role in deprescribing, what activities GPs are using in practice remain unclear.
It is also important to consider how deprescribing activities are being used in practice as this process is essential for successful deprescribing.16 Research indicates that how deprescribing activities are delivered has previously been under-reported in deprescribing trials, making it challenging to apply deprescribing evidence into clinical practice.17 In the absence of a gold standard deprescribing process, Woodward’s five principles of deprescribing offer a strong framework and are core to the deprescribing process.18 The five principles of deprescribing consist of (1) review all current medications; (2) identify medications to be targeted for cessation; (3) plan a deprescribing regimen; (4) plan in partnership with patient and carers; and (5) frequent review and support (see figure 1).6 Woodward’s principles were the first deprescribing guiding principles described in the literature and state that deprescribing should be a collaboration between the prescriber and patient, with subsequent adaptations placing an even greater emphasis on the importance of patient-centred care.18 19 The principles were developed with corresponding deprescribing activities; however, whether deprescribing interventions are following these recommendations is not known.
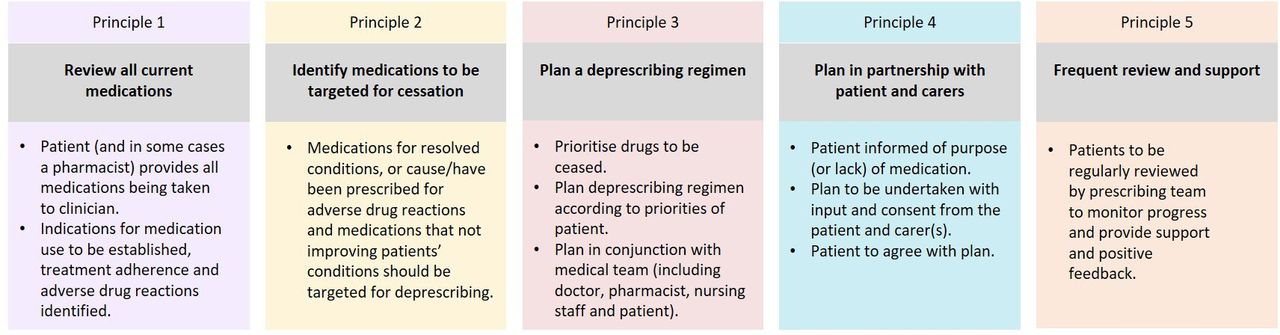
Woodward’s five principles for deprescribing.6
To date, research has focused on deprescribing activities or adapting deprescribing principles, independently, rather than consolidating the two for use in practice. Further, to our knowledge, no reviews have looked specifically at deprescribing activities and principles in general practice. Examining activities and principles together may help to identify areas of the deprescribing process that require attention and provide a comprehensive and accessible knowledge base for GPs, to support and inform their decision-making around deprescribing. As scoping reviews have become a popular, rigorous and transparent method for providing in-depth and comprehensive coverage of the literature,18 we conducted a scoping review to provide an up-to-date and inclusive look at deprescribing activities in general practice and map them to a well-known set of deprescribing principles. Specifically, we aimed to (1) provide a summary of the deprescribing literature across all medical conditions presenting to general practice; (2) map the activities to Woodward’s five principles of deprescribing; and (3) identify any key deprescribing activities being tested in general practice interventions.
Method
Search strategy
Methodology was decided on in April 2020 via discussion between authors. A research librarian at the University of Melbourne was consulted to develop search terms and methods. Studies were identified by searching electronic databases Medline, EMBASE (Ovid), CINAHL, Australian New Zealand Clinical Trials Registry (ANZCTR), Clinicaltrials.gov, ISRCTN registry and OpenGrey from inception to the end of June 2021. Handsearches of four primary care journals (Annals of Family Medicine, BMC Family Practice, Family Practice and Journal of General Practice (BJGP)) were conducted using the search function provided by the journal websites. See table 1 for key concepts for searching and online supplemental appendix A for full search activity.
Supplemental material
Key concepts for searching
Participants
Studies that focused on adults attending general practice and/or healthcare professionals in general practice were included, regardless of the primary diagnosis, type of healthcare professional delivering care, country in which study took place or year published. Studies were excluded if they were not conducted with human participants. Studies focusing on participants younger than 18 years of age were also excluded due to the unique nature of deprescribing medications in paediatric populations (for example see Begum and Tomlin20).
Setting
Studies were eligible for inclusion if they were set in general practice (ie, participants were recruited from, or deprescribing was conducted in, a general practice clinic), and if the medication being deprescribed was one that was taken orally. Studies where patients were recruited from general practice but the majority of the deprescribing process was conducted in the patients’ home or other setting were excluded. Studies that did not describe the activities of the deprescribing intervention and if they focused on prescribing/deprescribing prevalence or adherence/non-adherence were excluded.
Types of studies
Studies were included if they were original research (randomised controlled trial (RCT), quasi-experimental, cohort study, qualitative and case studies). Systematic reviews and meta-analyses were included for handsearching purposes. Protocol papers and protocol registrations were included as they describe interventions that are being prepared for trial. Where the full protocol paper was available, this took precedence over the protocol registration record. Articles were excluded if they were non-empirical research (editorials, guidelines/guideline development, commentaries, opinions, letters, factsheets, clinical education activities). Conference abstracts were also excluded as they often lack in-depth intervention descriptions. Studies were excluded if a deprescribing intervention was not the focus. Study quality was not formally assessed and was not an inclusion criteria as this is not a requirement of scoping reviews.21
Study selection
One reviewer (AC) reviewed all titles and abstracts for eligibility, and 10% of titles and abstracts were separately reviewed by a second reviewer (CK-H) for agreement. The eligible full text articles were downloaded into the COVIDENCE web-based screening and data extraction tool.20 Two reviewers (AC and CK-H) independently evaluated 10% of the full-text articles to decide if they meet the inclusion/exclusion criteria. Five articles required discussion between the two reviewers to resolve disagreement about inclusion. Consultation with a third reviewer was not needed as agreement between the reviewing authors was reached. AC then reviewed all remaining full-text articles for inclusion. A data extraction form was developed to gather the following information for all included studies: author(s), country and year of publication, study type, population, setting, methodology, primary medical condition, medication to be deprescribed, comparator information and study results. To extract information about the deprescribing activities used in the interventions, full-text articles were uploaded into NVivo22 and coded by AC.
Categorisation of the results
Initial reason for medication prescription targeted for deprescribing was categorised by the International Classification of Diseases 11th Revision (ICD-11)23 where possible. To create order for the complex material found in the included studies, intervention activities were categorised into ‘who’, ‘what’, ‘how’ and ‘where’. Specifically, ‘what’ activities were mapped to the five principles as these are the activities that most pertain to the deprescribing process. For patients, GPs, allied health and eTools that were categorised under ‘who’ were further classified as ‘lead’ or ‘support’. A lead role was assigned if they initiated and oversaw the deprescribing process. A support role indicated they were not the initiator or overseer, but were involved in the deprescribing process. eTools were categorised under ‘who’ as they were used in place of a person to conduct deprescribing activities. Any activities not mapped to the five principles were grouped together to determine if they contained common traits to form additional principles. Additional principles were named for when the mapped activities took place within the original five principles.
Patient and public involvement
Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Results
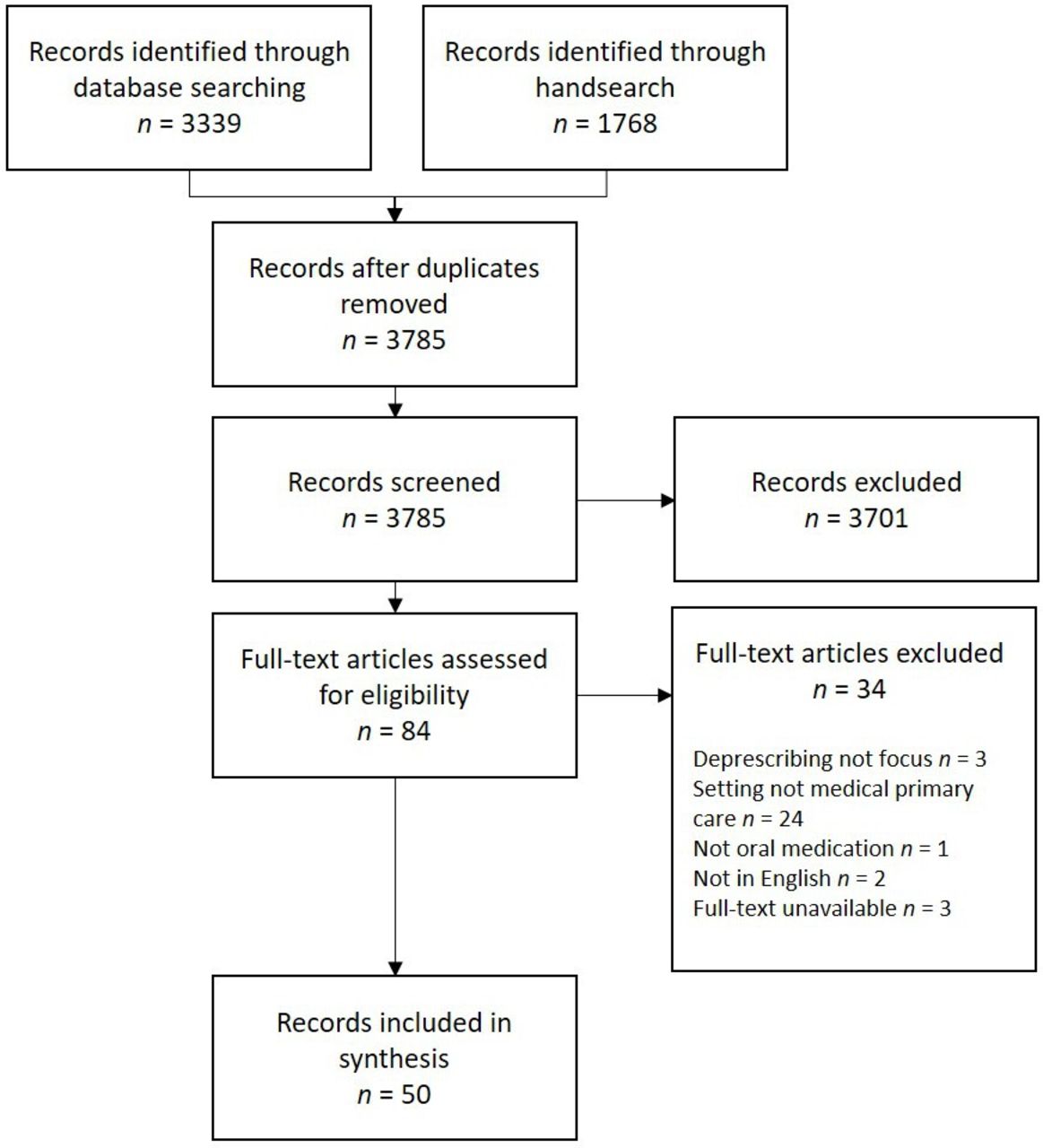
The search yielded a total of 5107 articles, 3785 after duplicates were removed. Review of titles and abstracts led to the retrieval of 84 full-text articles for assessment. Of these, 50 empirical research studies were included (see online supplemental appendix B for individual study characteristics). Figure 2 shows the flow of articles through the search and eligibility screening process.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram showing results of search and process of selecting articles for deprescribing scoping review.
Included articles were published between 1983 and 2021, with an increase in publication rates in the last 5 years (table 2). Research was primarily conducted in the UK (n=9 (18%)), The Netherlands (n=7 (14%)) and the USA (n=7 (14%)). Twenty studies specifically targeted older patients (aged 60 years and older).24–43
Characteristics of publications on deprescribing activities
Most studies were randomised controlled trials (RCTs) (n=31 (62%)) and aimed to reduce polypharmacy (n=16 (32%)) and benzodiazepine use (n=14 (28%)). Definitions of polypharmacy varied between studies, ranging from ≥2 medications24 to ≥15 medications.25 Two studies did not specify what the target medication was initially prescribed for—one focused on falls prevention, the other on long-term use.26 44 In a third of the studies, the target medication was initially prescribed for the treatment of mental illness. The most common reason for deprescribing was medications deemed as IMU (n=26 (52%)). Some studies specifically targeted a subset of IMU (eg, long-term use) which is presented as an individual reason for deprescribing.
Activities and principles of deprescribing
Deprescribing activities and principles were applied across populations, diagnoses and medication types. Overall, 17 activities were identified and were mapped to seven principles. Six activities did not fit within the original five principles, therefore two additional principles were created: principle 0: engage practice staff in education and appropriate identification of patients and principle 6: provide feedback to staff about deprescribing occurrences within the practice. Principle 0 included five activities which occurred prior to activities mapped to Woodward’s five principles. Principle 6 included one activity which occurred after the five principles.
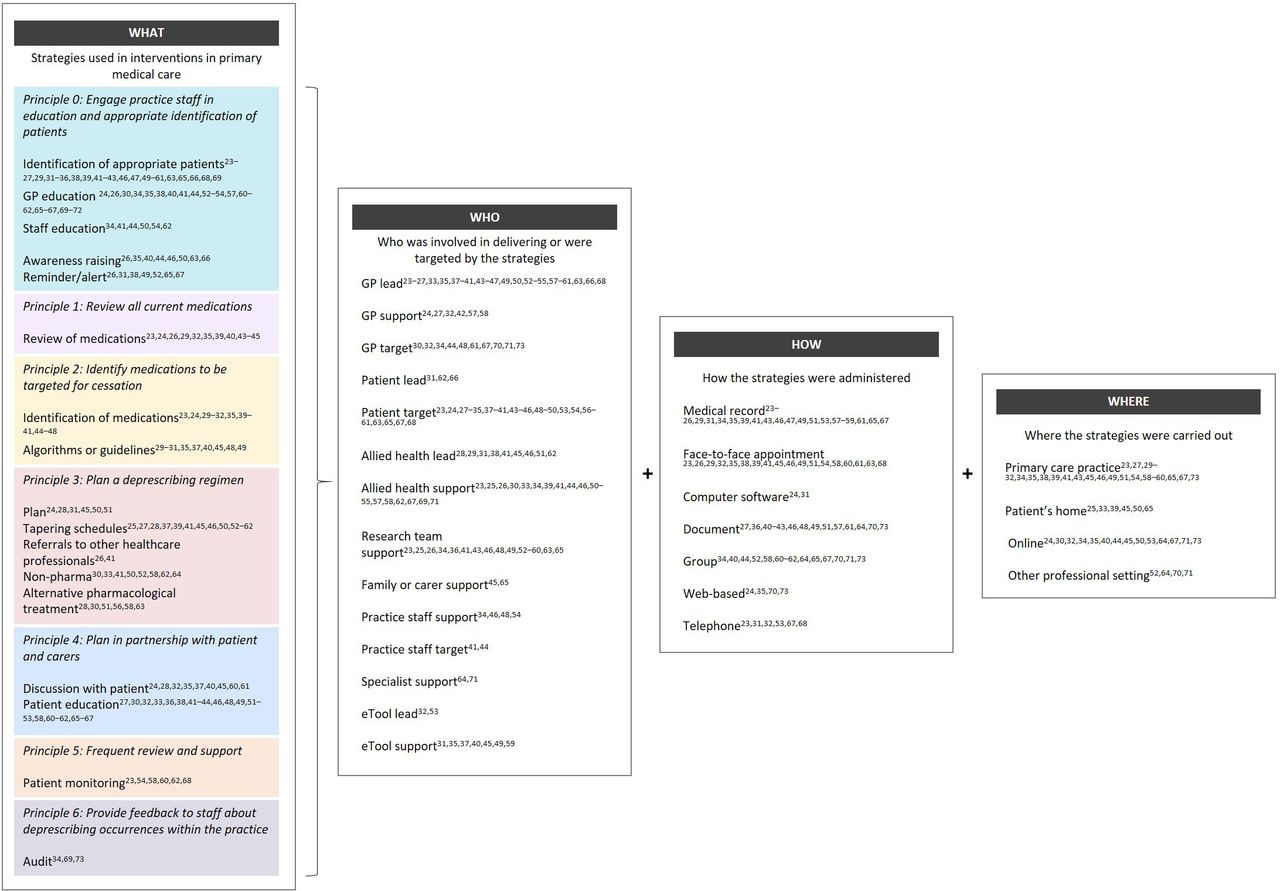
Unsurprisingly, GPs and patients were heavily involved in the deprescribing process. Activities of deprescribing were administered in several different ways including medical records and documents. Deprescribing activities were mainly carried out in the general practice clinic. Figure 3 shows the deprescribing activities mapped to the corresponding principle including who is involved in the deprescribing process, how activities and principles might be administered and where they take place. Figure 4 presents Woodward’s five principles with the addition of principle 0 and principle 6.

Deprescribing activities mapped to corresponding principles. GP, general practitioner.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Adapted deprescribing principles based on Woodward’s five principles of deprescribing. GP, general practitioner.
Principle 1: review of all current medications
A review of all medications was conducted in 11 studies24 25 27 30 33 36 40 41 43 45 46 and was the only activity mapped to principle 1. GPs most commonly lead this activity,24 25 27 36 40 41 43 45 46 with pharmacists30 and eTools33 also given a lead role.
Principle 2: identify medications to be targeted for cessation
Identification of medications for cessation was conducted in 15 studies.24 25 30–33 36 40–43 46–49 This was led mostly by GPs (n = 13),25 31 32 36 38 40–42 46–50 with a pharmacist30 and an eTool33 leading two further studies. In one study, leadership of identifying medications was shared by a GP, practice nurse or pharmacist.47 Identifying the medications for cessation was were often supported by algorithms (n=9) that used information from the review of medications in principle 1 and made recommendations for which medications to target for deprescribing.30–32 36 38 41 43 49 50 Four studies incorporated the algorithm in an eTool.32 36 38 41
Principle 3: plan a deprescribing regimen
Documented plans for deprescribing were made in five studies.25 29 32 51 52 A variety of healthcare professionals were involved in this process including pharmacist leads,29 32 an eTool,25 a nurse52 and a GP.51 Tapering schedules were widely used (n = 19)26 28 29 38 40 42 47 51 53–63 and were delivered by GPs28 38 40 47 51 55 62 and pharmacists.29 A pharmacist, GP and nurse were responsible for tapering schedules in one study.63 eTools were used in two studies.54 60 In 10 studies researchers developed and disseminated the tapering schedule to participants.26 42 50 53 56–59 61 64 Referrals to other healthcare professionals,27 42 non-pharmacological options31 34 42 51 53 59 63 65 and alternative pharmacological options29 31 52 57 59 64 were also mapped under principle 3. These activities were used to support patients to deprescribe after receiving a tapering or deprescribing plan. Non-pharmacological options included guided mindfulness-based cognitive therapy51 and exercise programmes.63
Principle 4: plan in partnership with patient and carers
Patients were included in the deprescribing discussions in eight studies.25 29 33 36 38 41 61 62 A deprescribing decision aid was used as a tool in one study to facilitate the deprescribing discussion.51 Carers were included in one study, although they were not involved in the deprescribing discussion. GPs conducted discussions with patients in six studies25 30 31 38 61 62 and were aided by an eTool in three studies33 36 41 and a pharmacist in one study.29
Patient education was also a commonly occurring strategy (n = 25).28 31 33 34 37 39 42 44–47 49 50 52–54 59 61–63 66–69 Education consisted of advice and information about when and how to reduce medications delivered in a variety of ways including receiving a letter in the mail,29 advice from their GP.28 One study used internet modules54 to extend this information by providing material on dealing with withdrawal symptoms and relapse, overcoming fear of stopping and staying well.
Principle 5: frequent review and support
Six studies reported five different approaches to monitoring patients after the deprescribing process was initiated.24 55 59 61 63 69 Monitoring involved follow-up telephone appointments24 69; follow-up in-person appointments which focused on the provision of positive reinforcement,61 tracking of physiological responses to deprescribing (eg, blood pressure and cholesterol checks)55 63 and completion of case reports.59 Follow-up timeframes ranged from 2 days69 to 6 months55 following enrolment in the study. Patients attended up to four59 61 follow-up visits over the course of the intervention. Three studies did not specify when follow-up visits occurred and four did not specify the number of follow-visits included in the intervention.
Principle 0: engage practice staff in education and appropriate identification of patients and Principle 6: provide feedback to staff about deprescribing occurrences within the practice
Five activities were mapped to ‘Principle 0: engage practice staff in education and appropriate identification of patients’, including the most frequently occurring activities found across all of the studies: identifying patients and GP education. Awareness raising of deprescribing among healthcare professionals and reminders and alerts for clinicians were also mapped to this principle. Each of these activities appear to be tasks that GPs, other healthcare professionals and general practice clinics should complete before patient appointments and medication management occurs. Identification of appropriate patients who were eligible for deprescribing occurred in most studies (n = 38).24–28 30 32–37 39 40 42–45 47 48 50–62 64 66 67 69 70 Although this may have occurred as study participant selection, it was included as an activity of deprescribing as GPs need to know which patients to initiate the deprescribing discussions with. GP education occurred in almost half of the studies (n = 24)25 27 31 35 36 39 41–43 46 53–55 58 61–63 66–68 70–73 and was conducted prior to any patient contact and therefore before deprescribing started. GP education was delivered in a variety of ways including workshops,27 training videos25 43 and as part of GP medical training.65 72 Practice staff education occurred less frequently35 42 43 46 51 55 63 and typically involved staff being invited to attend the education provided to GPs, rather than delivery of separate or tailored training. Awareness raising was achieved in general practices through practice recruitment and training in study protocols, practice sign-up and participant recruitment (n=9).27 36 41 43 46 47 51 64 67 Eight studies27 32 39 43 50 53 66 68 used reminders or alerts mostly via patient medical records to notify GPs that a patient with an upcoming appointment required a medication review.
The only activity mapped to principle 6 was the auditing of deprescribing occurrences in practice researchers in three studies.35 70 73 One study provided practices with comparisons of quality of care against agreed-on standards of practice in the form of a report at unspecified intervals.35 Two studies used monthly reports given to GPs with one including intervention monitoring information70 and the other providing information regarding GP benzodiazepine prescriptions.73
Key deprescribing activities
Four deprescribing activities were the most commonly used in the 50 reviewed studies: (1) 76% of studies used identification of appropriate patients; (2) 50% used patient education; (3) 48% used GP education; and (4) 38% used a tapering schedule. Identification of these key activities may guide the development of future deprescribing interventions in general practice as well as provide a quick reference for GPs of deprescribing activities in clinical practice.
Discussion
Deprescribing is critical to addressing the well-recognised problem of IMU, but is currently underperformed in general practice. In looking to assist GPs to engage in deprescribing this, scoping review amalgamated deprescribing activities being used in general practice with pioneering principles of deprescribing. This may provide GPs with a comprehensive and accessible knowledge base for when to use deprescribing activities principles in clinical practice.
Two principles were added to Woodward’s original five principles of deprescribing4 addressing an area of concern in the literature regarding the lack of GP-initiated deprescribing. Principle 0 encompassed activities aimed at helping GPs to initiate the deprescribing conversation. Auditing activities mapped to principle 6 may also complement principle 0 as auditing information allows staff to improve professional practice.74 Providing GPs with information about their own deprescribing practices may improve initiation of the deprescribing process.
The most frequently occurring activities were identifying appropriate patients for deprescribing, patient and GP education and using tapering schedules. Identifying which patients require deprescribing was classified as a deprescribing activity in the current study. Although this activity was used as part of study eligibility, this may be important for the initiation of the deprescribing process for GPs and warrants further testing.
Our findings are consistent with previous literature that has found heterogeneity in the deprescribing process. In particular, the current review adds support for GP and patient education being critical components of the deprescribing process as suggested by Dills et al.14 However, identifying appropriate patients for deprescribing has not previously been specified as deprescribing activity to be used in practice and highlights a current gap in the literature.
Focusing on deprescribing conducted solely in general practice yielded different findings from previous literature. We found that 32% of the included studies focused on polypharmacy compared other reviews that included a wide array of primary care settings (eg, 65% of studies in the scoping review by Isenor et al).15 Traditionally, polypharmacy is an issue for patients aged 65 years and older. As general practice is most commonly attended by adults aged 20–64,74 this age difference may be reflected in the current results. Such differences in population and medication suggest that deprescribing activities may also be different within the general practice setting. Previous research has also suggested pharmacists as leaders of the deprescribing process; however, when focusing on general practice, GPs were overwhelmingly responsible with other healthcare professionals in supporting roles. GPs may be logical leaders for deprescribing, although they may require support from others.
Strengths and limitations
Both a limitation and strength, this review included protocol papers and protocol registrations. As deprescribing is only emerging in the literature, we thought it is important to see what activities are currently being used or will be used in general practice. Protocol papers and registrations are required to describe the intended intervention rather than the actual tested intervention therefore some activities may have been missed.
An assessment of bias was not conducted on the included studies. The most common study design included in this review was RCTs, which suggests that bias may be limited; however, most (n=21) of the RCTs were described in protocol registrations or protocol papers only. As scoping reviews allow for the inclusion of a wider range of literature, the inclusion of protocols minimalised the risk of missing relevant interventions. Further, a rigorous search was conducted, allowing for a diverse set of literature to be identified in a robust and reproducible manner. Finally, previous literature has focused on studies conducted from 2002 to 2020, possibly due to ‘deprescribing’ only having been coined as a term in 2003. As medication discontinuation is not a recent concept, the current review may have captured some previously missed deprescribing activities.
Implications for research and practice
The addition of principle 0 and principle 6 suggests that the deprescribing process can be implemented and conducted in clinical practice cyclically, potentially creating a self-sustaining process. To preserve this ‘deprescribing loop’, a whole of practice approach may be needed. Certainly, the activities mapped to the additional principles indicate that initiation of deprescribing is in the hands of not only the GP but also the wider practice staff who may play an essential role in supporting the GP and patient to initiate deprescribing. In particular, practice staff will most likely be required to take on the role of identifying appropriate patients for deprescribing. Currently, research teams are heavily involved in conducting this activity; however, outside of the research setting and in clinical practice, this task will need to be assigned to nominated practice staff for this important step to be carried out.
This scoping review has provided an overview of what activities are being used in deprescribing and operationalised them into a framework principles of deprescribing; however, guidance is still needed for how GPs might select activities for different patients and medication type. This may also assist in identifying roles for practice staff and management.
Finally, as evidence-based deprescribing principles are still lacking, the adapted principles presented in the current study should be tested and evaluated in practice. In particular, the cyclical nature of the described deprescribing process should be tested for feasibility.
Conclusion
Evidenced-based deprescribing activities and principles to guide deprescribing have yet to be combined to develop a comprehensive but easy to use guide to support GPs to deprescribe. This scoping review was the first to amalgamate deprescribing activities and pioneering deprescribing principles resulting in two additional principles. The guiding principles helped to capture the variety of deprescribing activities that currently exist in the literature and has highlighted which areas of the deprescribing process require further attention. Further, the activities included within each principle can provide guidance for GPs, practice staff and practice management teams on how they can contribute to the deprescribing process. The current findings may provide a starting point by offering a selection of deprescribing options to use in practice.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The datasets used and/or analysed during the current study are included in the article and as supplementary information.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @amy_x_coe
Contributors All authors (AC, CK-H, SF, EM, JG) contributed to the conceptualisation and design of the study. AC and CK-H performed screening. AC performed data extraction and synthesis which was reviewed by JG and CK-H. AC drafted the manuscript. JG and CK-H revised early drafts and all authors revised later drafts.
Funding AC is funded by the Rotary Club of Richmond and Kaiyu Scholarship for PhD Research in Mental Health, Australian Rotary Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.