Article Text

Abstract
Objective Overview on risks of acupuncture-related adverse events (AEs).
Design Systematic review and meta-analyses of prospective studies.
Data sources PubMed, Scopus and Embase from inception date to 15 September 2019.
Eligibility criteria for selecting studies Prospective studies assessing AEs caused by needle acupuncture in humans as primary outcome published in English or German.
Data extraction and synthesis Two independent researchers selected articles, extracted the data and assessed study quality. Overall risks and risks for different AE categories were obtained from random effects meta-analyses.
Main outcomes Overall risk of minor AEs and serious adverse events (SAEs) per patients and per treatments.
Results A total of 7679 publications were identified. Twenty-two articles reporting on 21 studies were included. Meta-analyses suggest at least one AE occurring in 9.31% (95% CI 5.10% to 14.62%, 11 studies) of patients undergoing an acupuncture series and in 7.57% (95% CI 1.43% to 17.95%, 5 studies) of treatments. Summary risk estimates for SAEs were 1.01 (95% CI 0.23 to 2.33, 11 studies) per 10 000 patients and 7.98 (95% CI 1.39 to 20.00, 14 studies) per one million treatments, for AEs requiring treatment 1.14 (95% CI 0.00 to 7.37, 8 studies) per 1000 patients. Heterogeneity was substantial (I2 >80%). On average, 9.4 AEs occurred in 100 treatments. Half of the AEs were bleeding, pain or flare at the needle site that are argued to represent intended acupuncture reaction. AE definitions and assessments varied largely.
Conclusion Acupuncture can be considered among the safer treatments in medicine. SAEs are rare, and the most common minor AEs are very mild. AEs requiring medical management are uncommon but necessitate medical competence to assure patient safety. Clinical and methodological heterogeneity call for standardised AE assessments tools, clear criteria for differentiating acupuncture-related AEs from therapeutically desired reactions, and identification of patient-related risk factors for AEs.
PROSPERO registration number CRD42020151930.
- adverse events
- risk management
- pain management
- complementary medicine
- general medicine (see internal medicine)
- quality in healthcare
Data availability statement
Data are available upon reasonable request. The full set of extracted data and the R-code underlying the meta-analyses are available from the corresponding and senior author (Petra.Baeumler@med.uni-muenchen.de, Dominik.Irnich@med.uni-muenchen.de).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- adverse events
- risk management
- pain management
- complementary medicine
- general medicine (see internal medicine)
- quality in healthcare
Strengths and limitations of this study
First systematic review on acupuncture-related adverse events (AEs) including a risk of bias assessment.
First meta-analyses on AEs related to acupuncture.
Complying with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Combining studies with heterogeneous AE definitions but providing respective sensitivity analyses.
Causality assessment based on descriptions of AEs as available from the included articles.
Introduction
Acupuncture describes the insertion of fine needles at defined points on the patient’s body for therapeutic or preventive purposes. It is used worldwide with growing popularity. In the European Union, acupuncture was identified as the most frequently provided method of complementary and alternative medicine with 80 000 physicians and 16 380 non-medical practitioners.1 In the UK alone, 2.3 million traditional acupuncture treatments are carried each year.2 In the USA, the number of acupuncturists doubled between 2002 and 2012.3 The effectiveness of acupuncture is supported by level 1a evidence, for example, for chronic musculoskeletal pain and headache,4–6 postoperative pain,7 8 postoperative nausea and vomiting,9 as well as allergic rhinitis.10 Furthermore, promising evidence exists for its potential role in the treatment of numerous other indications, such as stroke rehabilitation,11 depression,12 aromatase inhibitor-induced arthralgia,13 and asthma.14 Thus, acupuncture offers a non-pharmacological treatment option for various highly prevalent conditions with great disease burden and significant health economic impact. Long-term pharmacological treatment of these conditions is often associated with substantial side effects.15 16 Consequently, also risk estimates on acupuncture-related adverse events (AEs) are required for evidence-based risk–benefit considerations that are essential for clinical decision making.
However, uncertainty remains about acupuncture safety. AEs related to acupuncture are repeatedly and controversially discussed in both scientific literature and public media. An overview of systematic reviews in 201717 illustrates that many of the previous reviews on the safety of acupuncture just summarised case reports or case series. In turn, those reviews, including studies that do allow for AE frequency estimation, such as cohort studies and large randomised controlled trials (RCTs), mostly addressed only certain types of AEs, particular patient groups, restricted acupuncture regimens or certain countries. These data are surely important for clinical decision making in particular cases but leave the overall risk of acupuncture-related AEs in the general population obscure. Additionally, debate exists about differentiating AEs from therapeutically intended reactions that are claimed to form part of the acupuncture treatment. For example, international consensus exists that aggravation of symptoms represents an AE, because disease burden increases. However, transient worsening of symptoms followed by long-term improvements can be interpreted as a so-called healing crisis in complementary and alternative medicine.18 In contrast, such consensus is still missing for local reactions, such as small bleedings upon needle withdrawal, needling pain, and flare around the needling site. These are also interpreted as beneficial signs by acupuncture experts and in standard textbooks and have been linked to neurophysiological mechanisms of acupuncture. Accordingly, quality and intensity of these events should be considered when classifying them as AE.19–21
The last review on prospective studies on AEs related to acupuncture with high external validity dates back to 2001,22 did not meta-analytically summarise AE risk estimates, and did not assess the quality of included studies. In addition, inconsistency and incompleteness of reporting in primary studies hampered the drawing of firm conclusions on acupuncture safety. Since then, various large-scale clinical trials and nationwide surveys on acupuncture safety have been conducted.
Therefore, it was the aim of this review to provide an up-to-date summary of prospective trials that were particularly designed to evaluate AEs related to needle acupuncture with manual or electrical stimulation and in combination with or without moxibustion.
Methods
We systematically reviewed prospective studies that reported on acupuncture-related AEs. The protocol has been registered at the International Prospective Register of Systematic Reviews23 on 25 September 2019 (registration number CRD42020151930, online supplemental appendix S1). The research checklists according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses24 and according to the guideline of Meta-analysis Of Observational Studies in Epidemiology25 are displayed in the online supplemental appendix S2.
Supplemental material
Supplemental material
Search strategy
We searched PubMed, Scopus and Embase for articles published before 15 September 2019 by applying the following search strategy: 1: acupuncture; 2: “adverse event”; 3: ”adverse events”; 4: “adverse effect”; 5: “adverse effects”; #1 AND #2; #1 AND #3; #1 AND #4; #1 AND #5. Additional records were identified from previous reviews on acupuncture-related AEs.17 “Acupuncture” and “adverse effects” are medical subject headings (MeSH) terms.
Inclusion and exclusion criteria
We included articles reporting on prospective studies (cohort studies, RCTs, surveys or surveillances) assessing AEs associated with needle acupuncture involving manual or electrical stimulation combined with or without moxibustion in humans as their primary outcome. Case reports and case series were not included. Only articles published in English or German were included. Publications on assessments of acupuncture point injection therapies or non-penetrating acupuncture point stimulation, such as laser acupuncture, acupressure or transcutaneous electrical nerve stimulation, were excluded. We also excluded articles reporting solely on moxibustion or restricted acupuncture regimens, such as press-needle, auricular, or one-point acupuncture. Trials focusing just on one type of acupuncture-related AE or just on a narrowly defined patient population were excluded.
Article selection and data extraction
Article selection was performed independently by two reviewers (WZ and PB, TS and PB, or LM and PB). Retrieved records were first screened for eligibility by abstract. Full texts were obtained for the remaining articles. Final decision about eligibility was obtained by consensus of all four reviewers.
Estimates of overall risks and risks for each reported type of AEs were extracted as absolute numbers of patients with AE per total number of patients and treatments with AE per total number of treatments. Data concerning AEs from sham-acupuncture or placebo-acupuncture treatments were not extracted. The different types of AEs were assigned to one of the following categories: bleeding, local pain, other local AE, distant pain, central nervous system, peripheral nervous system, vegetative nervous system, motor system, gastrointestinal/gynaecological system, cardiovascular system, respiratory system, generalised skin reactions, headache, emotional interference, sleeping problems, AE related to moxibustion, needling malpractice, aggravation of symptoms, and other or unclassified AE (online supplemental appendix S3).
Supplemental material
Following the differentiation between AEs and adverse drug reactions defined by the International Conference on Harmonisation (ICH) of Good Clinical Practice,26 articles were classified into reports on AEs irrespective of their causal relationship to acupuncture and adverse reactions for which a causal relationship was a reasonable possibility. Serious adverse events (SAEs) were reported as indicated in the included articles in accordance with the ICH criteria. These include any untoward medical occurrence that at any dose results in death, is life-threatening, requires inpatient hospitalisation or prolongation of existing hospitalisation, results in persistent or significant disability/incapacity or is a congenital anomaly/birth defect.26 AE definitions and severity assessments as stated in the included publications are provided in the online supplemental appendix S4. Causality assessment of SAEs was performed by independent acupuncture therapists who were medical doctors with more than 300 hours of acupuncture training and with more than 10 years of intensive acupuncture practice. As the basis of this assessment was limited to incomplete information provided in the articles, for example, lacking time references, the standard categories of the WHO-UMC (Uppsala Monitoring Centre) causality assessment system27 were reduced to 'possibly related to acupuncture', 'unlikely related to acupuncture', or 'unclassifiable'. AE risk estimates given as patients with AE per total number of patients were interpreted according to the guidelines of the Council for International Organisations of Medical Sciences as very common (≥1/10 patients), common (≥1/100 to <1/10), uncommon (≥1/1000 to <1/100), rare (≥1/10 000 to <1/1000) or very rare (<1/10 000).28
Supplemental material
Documentation of study characteristics included the study type, the country in which the study was conducted, the reporter, the method and the time point of AE assessment, complaints as well as the age and the gender structure of the study population, the average number and the frequency of treatments per patient, the average number of needles per treatment, the needle in time, the acupuncture style, the method of needle stimulation, and the number, the gender, the training, and years of experience of acupuncturists. Data on patients’ and acupuncturists’ AE reports from the article published by Weidenhammer et al in 2008 were handled as two separate trials.
Risk of bias assessment
Included studies were assessed for risk of bias according to a checklist developed by Faillie and colleagues for systematic reviews focusing on drug AEs.29 This checklist is applicable to RCTs, cohort studies, case–control studies, nested case–control studies, and systematic reviews. The questions are structured in eight risk of bias domains. Possible answers are ‘not applicable’, ‘yes’, ‘unclear’ or ‘no’. A summary risk of bias assessment is provided for each domain as well as for the whole study. According to the inclusion criteria of this review, questions concerning systematic reviews, cross-over trials, and case–control studies were not applicable.
Data analysis
Data were analysed using the package meta implemented in R.30 Pooled estimates with 95% CIs for overall AE risk and risks of different types of AEs were obtained from proportion meta-analyses. Random effects models were calculated by the Hartung-Knapp method with arcsine transformation of proportions. Cochran Q test, and I2 statistics were used to assess the heterogeneity of included studies. Meta-analyses were performed for the overall risks for an AE, for an SAE, for an AE requiring treatment, and the risks for the different types of AEs. Separate meta-analyses were conducted for AE risks given as the number of patients with AE per total number of patients undergoing an acupuncture series and AE risks given as the number of treatments with AE per total number of treatments performed. All studies reporting the respective risks were included in the different meta-analyses. All AEs that were reported separately in the articles but were allocated to the same AE category were treated as they had occurred in different patients or treatments, respectively. Sensitivity analyses were performed for studies that explicitly only reported about AE that had, at the discretion of the assessors, a causal relationship to acupuncture treatments. None of the articles reported the mean and variance of the number of AEs per treatment. Thus, the expected number of AEs per treatment could not be estimated by means of a meta-analysis but just by considering the sum of AE relative to the sum of treatments. An additional sensitivity analysis was performed by excluding AEs that are usually very mild and transient or are often argued to be part of the treatment or a desired treatment response, such as transient bleeding, needle site pain or a flare around the needle insertion point. AEs that were indicated by any means as significant were not excluded from this sensitivity analysis.
Patient and public involvement
No patients were involved in defining the research question, the outcome measures, the design, or conduct of this review. No patients were asked to advise on interpretation of results. Authors will share the results during patient seminars and information events. A concise version of the results will be made available for non-profit acupuncture organisations to be presented on their web pages.
Results
Study characteristics
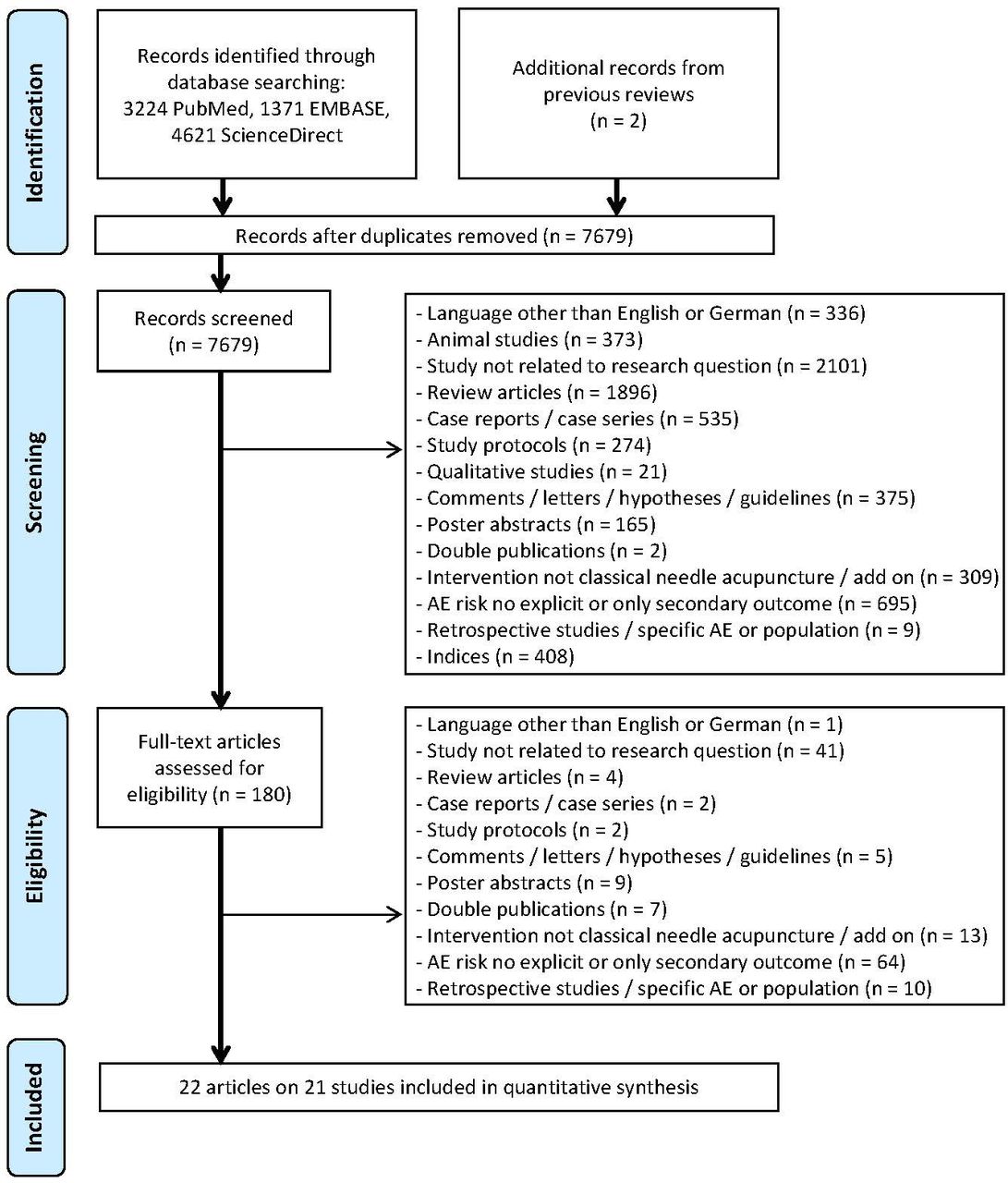
A total of 7679 records were retrieved from the database search and two were identified from previous reviews on acupuncture-related AEs. A total of 7499 records could be screened by abstract, and for 180 articles full texts were obtained. A total of 22 articles reporting on 21 studies covering 12.9 million treatments met our inclusion criteria (figure 1).31–52 In two studies, different data assessments on different subpopulations were performed and are treated independently in the present analyses. In one study, patient-reported AEs were assessed after one of the first treatments and three months after treatment,38 39 and in one large study, AEs were documented by therapists and in addition by a subgroup of patients.46

Flow diagram. designed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses.24 AE, adverse event.
Study characteristics are provided in table 1. The four largest trials, which included 100 000 to 500 000 patients treated in over 750 000 acupuncture sessions, were cohort studies performed as part of the German Model Projects on Acupuncture (Modellvorhaben Akupunktur).33 41 46 49 Three nationwide surveys from the UK (described in four articles),38–40 48 one in-house surveillance report from Japan,51 and one summary of AE assessments nested within three Chinese RCTs52 included 2000–6000 patients receiving over 30 000 treatments, respectively. In three surveys, two from South Korea,44 45 one from Japan,35 and one from Brazil,32 around 1000–2000 patients were included and treated in up to 14 000 acupuncture sessions. One nationwide survey conducted in Sweden assessed the AE risk based on data from over 9000 acupuncture sessions.43 In seven studies, less than 500 patients receiving a maximum of 3 500 treatments were included: four AE assessments nested within RCTs or clinical trials from China,47 Hong Kong, 31 36 and Sweden,37 one Japanese50 and one German survey,34 as well as one German cohort study.42 In most studies, acupuncture was used to treat pain in middle-aged patients. In six articles, no details on the patients’ condition were provided.34 35 40 43 48 50 Two articles reported explicitly on short-term AEs after one particular treatment only.39 45 All but five articles provided sufficient information to infer that acupuncturists had a firm medical background and/or had received intensive acupuncture training.34 36 37 42 43 One German survey also included ‘other practitioners’ most likely non-medical practitioners (Heilpraktiker) with non-standardised acupuncture training.34
Study characteristics
Eight articles described AEs reported by patients only,31 32 37–39 45 46 49 and seven articles described AEs reported by acupuncturists only.33 40 41 44 46 48 51 As said before, Weidenhammer et al described therapists’ and patients’ AE reports separately.46 Zhao et al combined the AE reports from patients and acupuncturists.52 In five articles, it was explicitly stated that acupuncturists recording the AEs also queried their patients about any uncomfortable experience during or after treatment.34–36 43 50 In two trials, AEs were documented by an independent assessor.42 47 In eight of the 22 included articles, AEs were reported irrespective of their relationship to acupuncture,31 33 34 37 40 48 51 52 while descriptions of AE assessments in 14 articles suggest that only AEs related to the acupuncture treatment were documented,31 ,32 35 36 38 39 41–44 46 47 49 50 and one article did not provide information about the AE definition.45 Further discrepancies were found in definitions of certain reactions as therapeutically intended. For example, da Silva et al did not count aggravation of symptoms as an AE because of difficulties in determining causality as well as severity and because of a common notion among practitioners that transient worsening forms part of the acupuncture treatment.32 In contrast, White et al reported aggravated symptoms as AE, but only those that were not followed by substantial improvements.48 The other articles did not specify aggravation of symptoms further.33–35 37 38 42 46 49 50 In addition, Endres et al did report on erythema at the needling site (which was accounted for in the present analysis) but did not include this in their overall AE incidence report, as it can also be regarded as a desired acupuncture reaction.33
Risk of bias assessment
According to the inclusion criteria, the study objective was clearly described in all articles (figure 2, category A). Study design was clear for all but one article, which stated that data were collected in the course of eleven clinical trials without further specification.36 Furthermore, all but one AE assessment were free of a run-in period. In one RCT, the safety assessment was initiated with a short delay.37 Both irregularities were rated as unlikely to introduce bias into the AE documentation. High risk of selection bias (figure 2, category B) was identified in the four RCTs and the AE assessment in eleven clinical trials (23% of articles) due to exclusion of patients with comorbidities or bleeding tendency. In contrast, in all surveys and cohort studies (77%), the risk of selection bias was rated as unclear due to an indistinct selection of therapists and/or patients, inclusion of voluntarily participating acupuncturists or acupuncturists from specialised medical centres only. Furthermore, none of the articles stated that patients were naive to acupuncture. Risk of bias due to study withdrawal or drop-out (figure 2, category C) was rated as low for all RCTs and two surveys, which reported only on short-term AEs (27%),39 45 and as high for one survey (5%), because treatment was ceased for 40% of the patients with AE.44 For the remaining studies (68%), the risk of bias due to early treatment termination was rated as unclear, as withdrawals and drop-outs due to AE were not reported. The risk of information bias regarding the safety outcome (figure 2, category D) was rated as high for one study (5%) because of an exclusive documentation of repeatedly occurring AEs37 and as unclear for all remaining studies (95%). At this, AE reporting by patients or acupuncturists instead of an independent assessor was classified as an unclear risk of social desirability bias. Further possible but unclear sources of detection bias were the sole use of a selection list35 36 39 44 or the sole use of open questions as AE assessment tool,49–51 lack of reporting on the AE assessment tool,43 45 47 and unclear definition of the safety outcome and/or the time point of the AE assessment (only directly after treatment,32 33 43 47 only after the last treatment initiation,37 38 41 46 49 and solely on recognition40 44 48 51). Further risk of information bias (figure 2, category E) appeared to be unclear due to poor reporting of treatment details in all but seven studies (32%).31 37 40 41 47 50 52 Bias arising from differential care, confounder assessment and statistical methods to control for confounding (figure 2, category F) was rated as low, as crude AE risk estimates and not relative risks with respect to a comparator group were extracted. The risk of bias due to other statistical methods (figure 2, category G) was also rated as low, as reporting of AE incidence was clear and well structured in all articles.
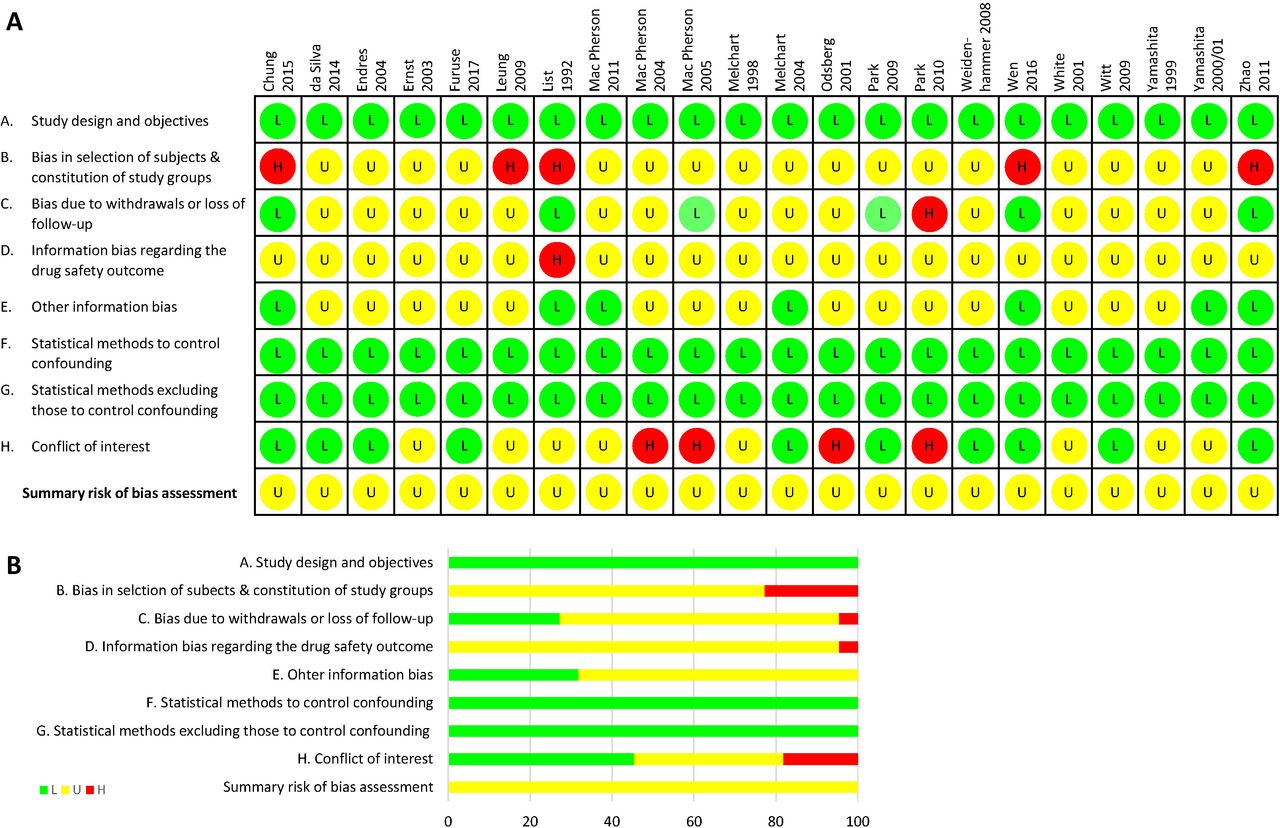
Risk of bias assessment. Risk of bias assessment was conducted according to Faillie et al.29 L, green (low risk of bias); U, yellow (unclear risk of bias); H, red (high risk of bias).
Bias due to conflict of interest (figure 2, category H) might be present in four articles (18%) due to funding by institutions with direct interest in the public acknowledgement of acupuncture.38 39 43 44 In eight articles (36%), funding or other conflicts of interest were not described.34 36 37 40 42 48 50 51 The 10 remaining articles (45%) included an explicit statement about funding by independent institutions and the absence of other conflicts of interest. For all studies, the overall risk of bias was rated as unclear based on the large proportion of unclear sources of bias.
Overall risk of acupuncture-related AEs
Eleven studies including 845 637 patients that assessed the overall AE risk as patients with AE among the total number of patients undergoing an acupuncture series were combined in a meta-analysis. The overall risk of at least one AE during a series of acupuncture treatments was estimated to be 9.31 (95% CI 5.10 to 14.62) per 100 patients treated (figure 3A).31 34 36 38 41 42 46 47 49 52 The median number of treatments per patient was nine (min 4.8, max 14), and the total number of treatments exceeded 7.4 million. Visual inspection indicated an association of the incidence of AEs neither with the number of treatments per acupuncture series nor with the study type (online supplemental appendix S5). Five studies reported the total number of acupuncture treatments with AE relative to the total number of treatments performed.32 34 36 40 42 Meta-analysis of these studies covering 55 026 treatments in total resulted in a risk of 7.57 (95% CI 1.43 to 17.95) treatments with AE per 100 treatments (figure 3B). Sensitivity analysis of studies reporting on adverse acupuncture reactions and not on AEs irrespective of their relationship to acupuncture treatments resulted in similar estimates32 36 38 40 41 46 47 49: 8.23 (95% CI 6.42 to 10.25) patients with at least one AE per 100 patients (figure 3C) and 6.08 (95% CI 0.00 to 38.76) treatments with AE per 100 treatments (figure 3D). Heterogeneity for all meta-analyses mentioned previously (including the sensitivity analyses) was substantial as indicated by an I2 between 98% and 100% (p<0.01).
Supplemental material

Meta-analyses of the overall risk of acupuncture-related AEs. Summary risk estimates for AEs were calculated as the number of patients or treatments with at least one AE relative to the total number of patients or treatments, respectively. Data on AE reports of patients and therapists from the article published by Weidenhammer et al in 200846 were handled separately. AE, adverse event.
Thirteen articles reported the incidences of different types of AEs per treatment (table 2).32 34–36 39 40 42–45 48 50 51 The average number of AEs per 100 treatments varied between 0.14 and 69.12. In total, 18 002 AEs were reported in 190 661 treatments, which makes on average 9.44 AEs per 100 treatments. Exclusion of AEs that are usually mild and transient or are often argued to be part of the treatment or a desired treatment response, such as transient bleeding, needle site pain or a flare around the needle insertion point, reduced this number to 4.81 (min 0.10, max 36.92) AEs per 100 treatments.
Number of AEs per treatment
Serious acupuncture-related AEs
SAEs were observed in five studies including 1 182 860 patients undergoing 10 570 678 treatments with incidences between two and 47 SAEs in 100 000 patients undergoing a treatment series and between two and 99 in one million treatments, respectively.33 38 41 46 51 Four articles reported that none of the AEs observed in a total of 1922 patients undergoing 19 005 treatments required medical treatment,32 36 47 50 and authors of five articles concluded that none of the AEs observed in 122 699 treatments fulfilled the ICH criteria for SAE.35 40 44 48 52 Eight articles did not mention SAEs or any AE description that allowed for inferences about SAEs.31 34 37 39 42 43 45 49
Meta-analyses of the overall risk of an SAE resulted in 1.01 (95% CI 0.23 to 2.33) patients with an SAE in 10 000 patients undergoing an acupuncture series (figure 4A 11 studies, 1 188 930 patients) and 7.98 (95% CI 1.39 to 20.00) SAEs in one million treatments (figure 4B and 1 study, 10 712 382 treatments). Exclusion of studies with zero SAE incidences changed these estimates to 1.47 (95% CI 0.10 to 4.46) in 10 000 patients suffering from an SAE when undergoing an acupuncture series and 16.90 (95% CI 0.49 to 56.60) SAEs in one million treatments. Sensitivity analyses of studies that only reported reactions with a plausible relationship to acupuncture resulted in risk estimates of 0.45 (95% CI 0.06. to 1.18) SAEs per 10 000 patients (figure 4C) and 5.45 (95% CI 0.50 to 15.67) per one million treatments (figure 4D). Again, heterogeneity between studies included in these two meta-analyses was substantial (I2>85%, p<0.001).
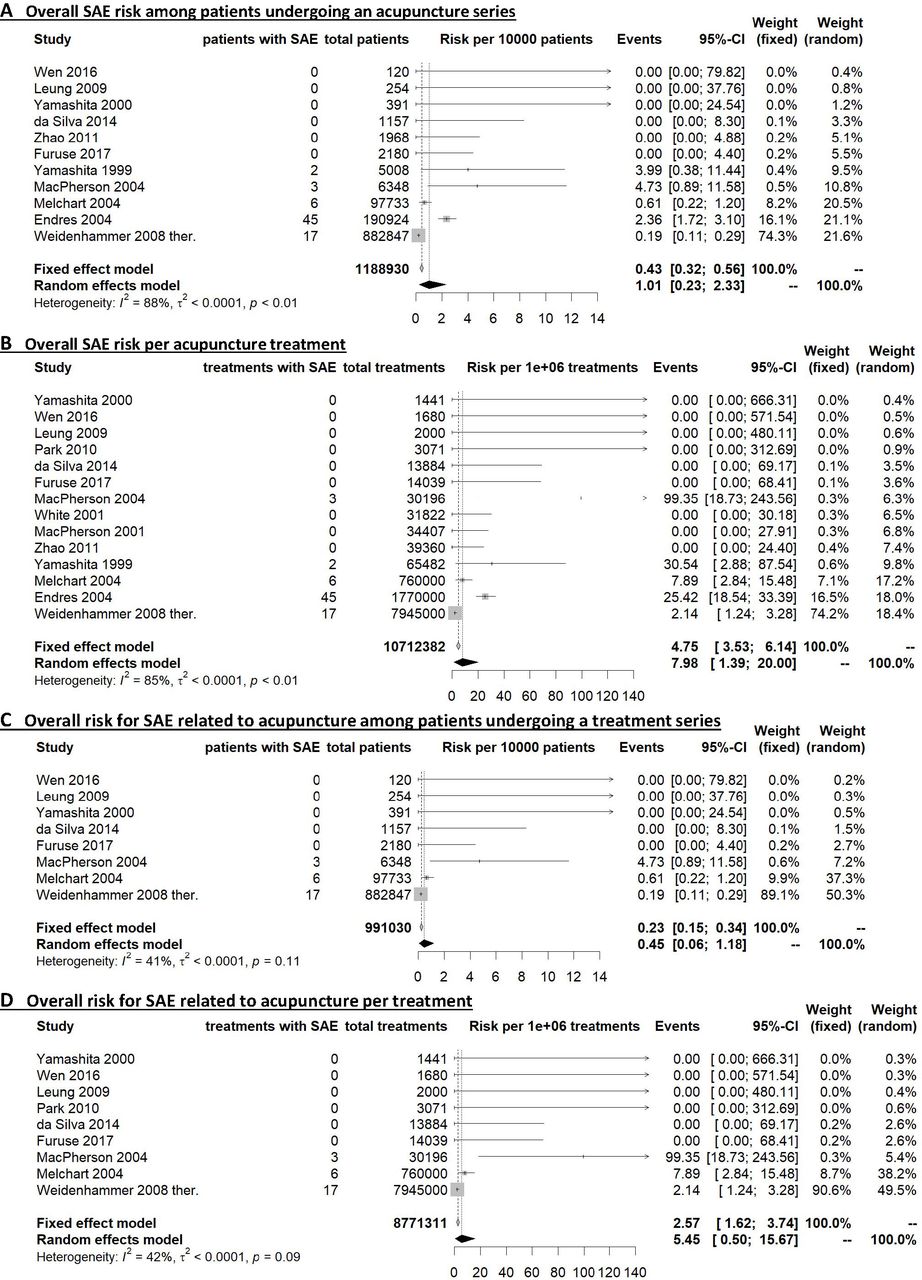
Meta-analyses of the overall risk of SAEs related to acupuncture. Summary risk estimates for SAEs were calculated as the number of SAE cases relative to the total number of patients or treatments, respectively. Data from the article published by Weidenhammer et al in 200846 refer to the AE reports of the therapists. SAE, serious adverse event.
The causality assessment of the 73 SAEs conducted by two acupuncture experts (table 3) resulted in 32 SAEs (44%) being possibly related to acupuncture. Among those, pneumothorax, strong cardiovascular or vasovagal reactions, and fall or trauma were the most frequent SAEs with a frequency of one to three cases in one million treatments each. One article that was not taken into account in the SAE meta-analyses, because observed AEs were not categorised in minor AEs and SAEs, also reported two cases of pneumothorax in over 200 000 patients undergoing on average 10 acupuncture treatments.49 Nineteen SAEs (26%) were rated as unlikely related to acupuncture. Among those were nine deaths observed in one large study among patients aged between 67 and 87 years and related to pre-existing health conditions.33 Authors reported that the resulting death rate of 4.71 per 100 000 patients was below the expected death rate derived from population statistics. Other SAEs classified as unlikely related to acupuncture were a circulatory reaction with amnesia, suicidal tendencies, acute general infection, a car crash two days after treatment, a malignant parotid tumour, tonic–clonic seizures, and an ophistotonus. Twenty-two SAEs (30%), intervertebral disk prolapses and hospitalisations due to pain exacerbation or unknown reasons, were rated as ‘unclassifiable’.
Causality assessment of SAEs as reported in the included articles
Acupuncture-related AEs requiring treatment
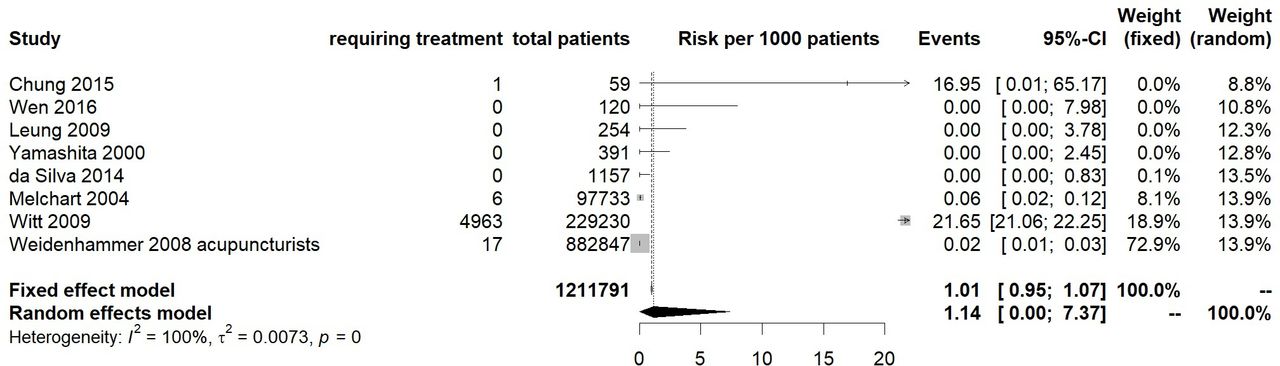
Eight studies determining the number of patients with AEs requiring treatment during an acupuncture series included 1 211 791 patients. The meta-analysis of these studies yielded a summary estimate of 1.14 (95% CI 0.00 to 7.37) in 1000 patients for the risk to suffer from an AE that required treatment when undergoing an acupuncture series (figure 5).31 32 36 41 46 47 49 50 Also here, heterogeneity was substantial (I2 of 100%). Two articles that had defined requirement of treatment as an SAE criterion reported lower incidences (2 and 6 events per 100 000 patients)41 46 than the other two articles reporting on AEs requiring treatment without referring to SAEs (1.7 and 2.2 in 100 patients).31 49
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Meta-analyses of the overall risk of AEs requiring treatment. Summary risk estimates for AEs requiring treatment were calculated as the number of patients with such AE relative to the total number of patients. AE, adverse event.
Risks of different types of minor AEs
Overall risks of the different types of minor AEs (for categorisation, see online supplemental appendix S3) were estimated in separate meta-analyses as patients with such AE per total number of patients undergoing a treatment series or as treatments with such AE per total number of treatments (table 4). Risks estimated in single studies (online supplemental appendices S6 and S7) varied largely for all types of minor AEs. Most frequent and commonly occurring minor AEs with summary risk estimates between 1% and 5% of patients undergoing an acupuncture series were bleeding events, pain at the needling site, other local AEs, vegetative reactions, aggravation of symptoms, and events related to the central nervous system. Summary risk estimates for bleeding events, needle site pain, vegetative reactions, and aggravation of symptoms also ranged from 1% to 5% of treatments, while the meta-analysis of symptoms related to the central nervous system per acupuncture treatment resulted in a risk of 2 in 1000 treatments. AEs estimated to be uncommon with summary risk estimates of 1–7 out of 1000 patients undergoing an acupuncture series were symptoms of the peripheral nervous system, pain distant to the needling site, gastrointestinal or gynaecological symptoms, headache, cardiovascular symptoms, affection of the motor system, generalised skin reactions, adverse emotional reactions, and sleeping problems. Symptoms affecting the peripheral nervous system, distant pain, as well as gastrointestinal or gynaecological symptoms were estimated to occur in 1–7 out of 1000 treatments; headache, cardiovascular and motor symptoms, as well as adverse emotional reactions were estimated to occur only in 1–8 out of 10 000 treatments. The risk of respiratory AE was estimated to be rare with a summary risk estimate of 4 out of 10 000 patients undergoing an acupuncture series and three out of 10 000 treatments. Summary risk estimates for AEs caused by therapists’ malpractice and burns caused by moxibustion were one to two in 1000 patients undergoing an acupuncture series and 2 in 10 000 to one in 1000 treatments, respectively.
Supplemental material
Supplemental material
Summary risks estimated for different types of AEs
Some of the studies showed outlying incidences for particular types of minor AE. List and Helkimo observed at least one vegetative reaction in the course of an acupuncture series for craniomandibular disorder in over half of the patients (58.6%),37 and MacPherson and Thomas reported vegetative reactions in 27.9% of treatments. 39 These findings exceed the frequency of vegetative reactions of up to 13.6% of patients identified in the remaining studies and were mainly based on patient reports of abnormal tiredness after treatment. List et al also report the highest incidence of aggravation of symptoms with 93% of patients with craniomandibular disorder (CMD) as well as the highest frequency of needle site pain with 44.8% of patients. This was followed by an RCT with 32.2% of patients suffering from needle site pain31 and a cohort study among patients with chronic pain of which 10% suffered aggravation of symptoms after receiving acupuncture.42 The remaining 19 articles reported incidences smaller than 3% for aggravation of symptoms and 14% for needle site pain.
Discussion
Overall risk of acupuncture-related AEs
To date, this is the first systematic review of prospective studies that provides summary risk estimates for acupuncture-related AEs derived from meta-analyses. The obtained results suggest that an AE can be expected in every 10th patient that undergoes a series of acupuncture treatments and, overall, in every 13th treatment. Minor AEs were common and represented the large majority of reported AEs. About half of the reported minor AEs are usually mild and transient or might even be regarded as part of the acupuncture treatment or therapeutically intended reactions (bleeding, needle site pain, and flare around the needle site).21 SAEs can be expected rarely in about every 10 000th patient in the course of an acupuncture series and, overall, in every 125 000th treatment. Sensitivity analyses excluding studies with zero SAE incidences still suggest SAEs being rare (every 7000th patient and every 60 000th treatment) particularly in comparison to SAE risk associated with pharmacological treatments.16 53 54 This risk was 30% to 50% lower when only considering studies reporting on SAEs with a plausbly causal relationship to acupuncture. AEs requiring treatment occur uncommonly in about every 900th treatment, but additional AEs are likely to also have involved medical decision making about further diagnostics and follow-up. With meta-analyses for the overall risk of acupuncture-related AEs covering over 845 637 patients undergoing more than 7.4 million treatments and for the risk of SAEs covering more than 1.2 million patients and 10.6 million treatments, the amount of data is equivalent to that on the safety of, for example, common analgesics.55 56 This work augments insights on acupuncture-related AEs from previous reviews with either narrow eligibility criteria or focusing on case reports.17 It includes data from the largest and most rigorous trials on acupuncture safety, for example, from the large nationwide cohort studies conducted in the UK and Germany, which had not yet been aggregated.33 38–41 46 48 49 Thus, our results provide rigorous support for the previously drawn conclusion22 57 58 that acupuncture is among the safe treatments in medicine with SAEs occurring rarely and half of the common minor AEs being mild and transient. The uncommon AEs requiring treatment necessitate solid medical competence of acupuncturists.
Types of AEs related to acupuncture and implications for medical education of acupuncturists
Common minor AEs were bleeding, needle site pain, other local reactions at the needling site, vegetative reactions, aggravation of symptoms, and AEs related to the central nervous system (1–5 out of 100 patients). This is in line with other reviews22 59 also on auricular60 and paediatric acupuncture.58 All other types of minor AEs can be regarded as uncommon (1–7 per 1000 patients), despite respiratory reactions that occurred very rarely (4 per 10 000 patients). SAEs most often reported were pneumothorax, strong cardiovascular or vasovagal reactions, and fall or trauma with one to three cases in one million treatments. Several other sometimes fatal SAEs repeatedly described in case reports were not observed in the included studies, for example, traumatic injuries of inner organs, local and systemic infections, subarachnoid bleeding, infective endocarditis, and cardiac tamponade.61–65 This is likely due to the fact that acupuncturists in most of the studies were well trained, as SAEs are claimed to be avoidable by proper acupuncture training and practice. Concordantly, cases of acupuncture malpractice were uncommon in the included trials.
Heterogeneity between studies
Possible causes of the substantial heterogeneity observed in all meta-analyses are differences in patient populations, needling regimens, AE definition, and AE assessment. Sensitivity analyses of trials reporting on adverse reactions only with a plausible relationship to acupuncture resulted in marginally lower overall AE risk estimates but reduced the SAE risk from one to 0.45 cases in 10 000 patients and from eight to five cases in one million treatments. Thus, reporting of SAEs irrespective of the relationship to acupuncture is surely more conservative but likely to cause risk overestimation. In line with this, the causality of more than half of the SAEs was rated as unlikely or unclassifiable by two independent acupuncture experts.
The variety of combinations of further patient-, treatment-, and assessment-related factors prevented meaningful subgrouping of studies for additional sensitivity analyses, and the likeliness of their contribution to the observed heterogeneity makes formal assessment for publication bias unadvisable.66 However, some distinct observations are worth discussing. Certain patient populations might be at higher risk of experiencing acupuncture-related AE; for example, in one study conducted among patients with CMD, AEs were prominently frequent.37 The role of acupuncture regimens in explaining heterogeneity could not be determined due to the limited information about number, location, and stimulation of needles. In contrast, the number of treatments per acupuncture series and study type seemed not to have impacted reported AE incidences.
Further possible causes of heterogeneity are differences in contrasting AEs from therapeutically intended reactions that form part of acupuncture treatment; for example, in contrast to international consensus,18 aggravated symptoms were not or only in part counted as AEs in two studies.32 48 Local reactions such as bleeding, pain, and flare at the needling site, which represented half of the AEs reported, are referred to as beneficial signs in standard acupuncture textbooks and by authors themselves.20 33 As the principle of acupuncture is to induce endogenous antinociceptive mechanisms and anti-inflammatory humoral responses through microtrauma of the skin and tissue, it can be argued that moderate local reactions are indeed desired reactions indicating an induction of regulative processes. Mild pain and a flare at the needling site have been linked to important neurophysiological mechanisms of acupuncture.21 Additionally, aching or soreness at the needling site might be part of the intended deqi sensation (propagated sensation along the channels) supposedly related to acupuncture effectiveness.19 The loss of small drops of blood upon needle withdrawal is interpreted as a sign of the patient’s constitution called ‘excess’ or ‘excess heat’ in traditional Chinese medicine terminology and was suggested not to be interpreted as AE.67 On the other hand, standard textbooks explicitly explain needling techniques avoiding pain and bleeding.20 68 This debate calls for a uniform, internationally recognised consensus on the definition of local acupuncture reactions as AEs, for example, according to their quality and intensity.
In addition, included studies differed in reporters (acupuncturists, patients, acupuncturists also questioning patients, and independent assessors), the type of documentation (selection list, open questions, or a combination of both), and assessment time points. Due to the large variability of combinations, the individual impact of these factors could not be estimated, but literature suggests that patients report more AEs than therapists,69 and that open questions presented to patients lead to lower risk estimates than the presentation of a selection list of possible AEs.31 Thus, standardised AE assessment methods should be established for acupuncture studies.
Risk of bias in included studies
Although large prospective studies are among the most important sources of safety data, they come with the known risk of information, selection, and confounding bias.70 Risk of information bias was mostly related to poor reporting of acupuncture regimens and the discrepancies in AE definition and assessment. This is in line with the shortcoming identified for reporting of AEs in acupuncture RCTs.71 Possible causes of selection bias identified were mainly voluntary participation of practitioners, unsystematic patient selection, and study conductance in highly specialised institutions. Practical reasons make these causes of selection bias inherent to safety studies. They, however, are unlikely to importantly impair external validity, considering the large number of patients and treatments, the variety of countries in which studies were conducted, and the inclusion of different study designs. Future large-scale comparative safety studies, along with modern statistical methods for confounder adjustment, could be used to contrast AE risks of acupuncture and other treatments and to identify patient and treatment characteristics associated with AEs in real-world clinical settings.72
Limitations
First, it is debatable whether studies should be summarised irrespective of whether AEs not necessarily related to acupuncture or adverse reactions likely caused by acupuncture were reported. In order to provide the most comprehensive information possible, respective sensitivity analyses were conducted. Another limitation with regard to the inclusion criteria is the restriction to articles published in German or English as many studies on acupuncture are published in Chinese. Additionally, the risk estimates for the different types of minor AEs are likely to be slightly overestimated and should be interpreted as a rough indication that allows distinguishing frequent from less frequent acupuncture-related minor AEs. In categorising the minor AEs, it was disregarded that several different AEs falling in one category could have occurred in the same patient or during the same treatment. Also, calculations of risks in treatments with AE per total number of treatments could not adjust for the fact that multiple AE assessments in the same patient are not independent. Furthermore, zero incidences of certain types of AEs were not available. Finally, the causality assessment presented for SAEs is limited to expert opinions and is only based on the information provided in the respective articles. Such an evaluation does not replace a rigorous causality assessment that would involve querying patients and therapists.
Clinical implications
Patients should be informed that acupuncture commonly causes minor AEs, but rarely SAEs. Examples for SAEs should at least cover the most frequent ones, pneumothorax, and strong cardiovascular or vasovagal reactions potentially leading to fall or trauma, along with the respective incidence of one to three per million treatments. Patients should also be made aware of the fact that a great part of the minor AEs are either very mild or even intended effects that indicate a beneficial physiological reaction. However, they should be encouraged to report any prolonged discomfort or pain that are to be avoided during treatment. Acupuncturists should carefully balance treatment intensity according to patients’ reactions in order to minimise AEs. They should assess local AEs upon needle withdrawal and query patients about AEs directly after treatment as well as at the subsequent visit. Therapists should be aware that, although uncommon, AEs requiring treatment can be expected and necessitate medical decision making. Medical competence is particularly required for the indication of acupuncture in patients at high risk of AEs or those in which AEs could lead to particular aversive outcomes, such as pregnant women, elderly and patients with cardiovascular comorbidities. In these patients, acupuncture can be especially beneficial, as conventional treatments, for example, with analgesics are often limited by side effects or drug interactions, but selection of acupuncture regimens needs to involve careful risk–benefit considerations. Theses medical competences required to provide optimal patient safety should also be reflected by acupuncture education standards and regulations. At this, policy makers should take into account the worldwide popularity of acupuncture which is likely to further increase, as its scientific level of evidence has led to more than 4000 practice guidelines recommending acupuncture for different mostly pain indications.69
Conclusion
Acupuncture can be considered among the safer treatments in medicine. It rarely causes SAEs, and the majority of the common minor AEs are very mild. AEs requiring medical management are uncommon. For optimal patient safety, acupuncture education standards regulations should reflect that solid medical competence of acupuncturists is required to manage AEs properly and to minimise the risk of malpractice. Clinical and methodological heterogeneity calls for an international consensus on AE assessment tools in acupuncture studies and criteria for differentiating acupuncture-related AEs from therapeutically desired reactions as well as identification of patient-related risk factors for acupuncture-related AEs. In particular, comparative safety studies are needed to contrast acupuncture to standard care in its main indications.
Data availability statement
Data are available upon reasonable request. The full set of extracted data and the R-code underlying the meta-analyses are available from the corresponding and senior author (Petra.Baeumler@med.uni-muenchen.de, Dominik.Irnich@med.uni-muenchen.de).
Ethics statements
Patient consent for publication
Acknowledgments
We thank Mrs Luise Möhring and Dr Barbara Jopen-Wolff from the Multidisciplinary Pain Centre, Department for Anaesthesiology, University Hospital LMU Munich. Mrs Möhring assisted in article screening and Dr Jopen-Wolff participated in the causality assessment. The contribution of Mrs Wenyue Zhang during the planning phase was made possible by the support of the China Scholarship Council of the LMU Munich.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors DI, PB and WZ defined the research question as well as inclusion and exclusion criteria for this systematic review. WZ, TS and PB were responsible for article screening, data extraction and classifications of adverse events. TS and PB performed the quality assessment. Questions and discrepancies were discussed among all authors until consent was achieved. PB conducted the meta-analyses and designed the tables and figures. All authors contributed to drafting the manuscript and approved its final version for publication. PB, the corresponding author, attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. As the senior author, DI is the guarantor of the work presented in this article and accepts full responsibility for the finished article, has access to any data and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests DI reports receiving honorarium and travel costs from non-profit academic organisations, physician chambers and universities for teaching and lecturing, and serving as president of the German Medical Acupuncture Association (Deutsche Ärztegesellschaft für Akupunktur, DÄGfA, a non-profit medical association). PB declares receiving honorarium and travel costs from non-profit academic organisations and universities for teaching and lecturing and being a member of the scientific advisory board of the DÄGfA. WZ and TS declare no other relationships or activities that could appear to have influenced the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.