Article Text

Abstract
Objectives COVID-19 causes lung parenchymal and endothelial damage that lead to hypoxic acute respiratory failure (hARF). The influence of hARF severity on patients’ outcomes is still poorly understood.
Design Observational, prospective, multicentre study.
Setting Three academic hospitals in Milan (Italy) involving three respiratory high dependency units and three general wards.
Participants Consecutive adult hospitalised patients with a virologically confirmed diagnosis of COVID-19. Patients aged <18 years or unable to provide informed consent were excluded.
Interventions Anthropometrical, clinical characteristics and blood biomarkers were assessed within the first 24 hours from admission. hARF was graded as follows: severe (partial pressure of oxygen to fraction of inspired oxygen ratio (PaO2/FiO2) <100 mm Hg); moderate (PaO2/FiO2 101–200 mm Hg); mild (PaO2/FiO2 201–300 mm Hg) and normal (PaO2/FiO2 >300 mm Hg).
Primary and secondary outcome measures The primary outcome was the assessment of clinical characteristics and in-hospital mortality based on the severity of respiratory failure. Secondary outcomes were intubation rate and application of continuous positive airway pressure during hospital stay.
Results 412 patients were enrolled (280 males, 68%). Median (IQR) age was 66 (55–76) years with a PaO2/FiO2 at admission of 262 (140–343) mm Hg. 50.2% had a cardiovascular disease. Prevalence of mild, moderate and severe hARF was 24.4%, 21.9% and 15.5%, respectively. In-hospital mortality proportionally increased with increasing impairment of gas exchange (p<0.001). The only independent risk factors for mortality were age ≥65 years (HR 3.41; 95% CI 2.00 to 5.78, p<0.0001), PaO2/FiO2 ratio ≤200 mm Hg (HR 3.57; 95% CI 2.20 to 5.77, p<0.0001) and respiratory failure at admission (HR 3.58; 95% CI 1.05 to 12.18, p=0.04).
Conclusions A moderate-to-severe impairment in PaO2/FiO2 was independently associated with a threefold increase in risk of in-hospital mortality. Severity of respiratory failure is useful to identify patients at higher risk of mortality.
Trial registration number NCT04307459
- COVID-19
- respiratory physiology
- respiratory medicine (see thoracic medicine)
- virology
- respiratory infections
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- COVID-19
- respiratory physiology
- respiratory medicine (see thoracic medicine)
- virology
- respiratory infections
Strengths and limitations of this study
This was a multicentre, prospective study.
The study has enrolled a conspicuous number of well-characterised patients hospitalised with COVID-19 pneumonia.
A selection bias may be due to the high number of severe patients due to the hub characteristics of the participating centres.
Not all patients were evaluated in room air conditions at admittance, thus potentially underestimating the severity of the study sample.
Introduction
SARS-CoV-2 and the related COVID-19 has caused a pandemic and ~860 000 deaths worldwide.1 The clinical spectrum can range from mild symptoms (eg, fever and malaise) to severe hypoxic respiratory failure, sepsis, multiorgan involvement and death. The infection appears to induce an inflammatory reaction with pulmonary infiltrates generating hypoxaemia secondary to intraparenchymal shunt and ventilation/perfusion mismatch, favoured by endothelial damage and dysfunction, and altered regulation of perfusion and associated with macroembolism and/or microembolism.2 3 So far, risk factors such as older age,4–6 severity of clinical presentation,4–7 increased D-dimer values,4 cardiovascular disease (CVD)4 5 and hypertension5–8 have been associated with unfavourable outcomes.
It has been proposed that clinical severity of COVID-19 should depend on the presence of any of the following criteria: a partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) ratio <300 mm Hg, a respiratory rate >30 per min and a peripheral oxygen saturation (SpO2) <93%.4 9–12 Several consensus statements recommend different PaO2 and SpO2 thresholds to prescribe continuous positive airway pressure (CPAP),13–15 non-invasive ventilation or intubation.16 Data on the association between severity of respiratory failure at admission and patients’ outcomes are still limited.
The aim of the present study was to assess the clinical characteristics of patients with COVID-19 based on the severity of respiratory failure, and to explore the relationship between the degree of gas exchange impairment and clinical outcomes (CPAP initiation and mortality).
Methods
An observational, prospective, multicentre study was conducted in three academic hospitals in Milan (Italy) from 7 March to 7 May 2020, involving three respiratory high dependency units and three general wards. A detailed list of participating centres is reported in the online supplemental file. The authors received no specific funding for this work.
Supplemental material
Patient and public involvement
Participants were not involved in the design and conduct of the research, interpretation of results and writing of the manuscript. The results of the study will be shared with local patients’ organisations by social media and summary reports on organisations’ websites.
Patients
Adult hospitalised patients with a virologically confirmed diagnosis of SARS-CoV-2 infection were considered eligible for study enrolment. Patients aged <18 years or unable to provide informed consent were excluded from the study. Hospitalisation criteria are reported in the online supplemental file.
Procedures
Anthropometrical and clinical characteristics were collected at admission. The PaO2/FiO2 ratio was calculated from the first available arterial blood gas analysis performed in the emergency department. PaO2/FiO2 thresholds to grade severity of respiratory failure were taken from the acute respiratory distress syndrome (ARDS) Berlin definition, and were17: normal (PaO2/FiO2 >300 mm Hg); mild (PaO2/FiO2 201–300 mm Hg); moderate (PaO2/FiO2 101–200 mm Hg); severe (PaO2/FiO2 ≤100 mm Hg). Blood count and biochemistry parameters were assessed during the first 24 hours after hospital admission.
Outcomes
The primary outcome was the description of patients’ clinical characteristics at admission and the assessment of in-hospital mortality based on the severity of respiratory failure.
Secondary outcomes were the assessment of intubation rate and application of CPAP during the hospital stay.
Study definitions
SARS-CoV-2 infection and co-infections
The COVID-19 diagnosis was based on a positive nasopharyngeal swab collected in the emergency department. SARS-CoV-2 infection was proved by means of reverse transcriptase PCR (RT-PCR). In case a first swab was negative, and the clinical picture was highly suggestive for COVID-19, the swab was repeated. Co-infection with influenza virus A and B, adenovirus, human rhinovirus, respiratory syncytial virus, human metapneumovirus were also investigated and analysed by means of RT-PCR or rapid influenza diagnostic tests.18 Microbiological testing for bacteria and fungi in blood, upper and lower airway tract, sputum and urinary antigens for Streptococcus pneumoniae and Legionella pneumophila were performed according to standard operating protocols.
Management of respiratory failure
Helmet CPAP was the only non-invasive respiratory support used in patients with confirmed or suspected COVID-19 pneumonia not responsive to oxygen masks in order to reduce the viral exposure of the healthcare workers in rooms without negative pressure.19 Patients with a PaO2/FiO2 ratio <300 mm Hg in room air were administered oxygen with nasal cannulae to reach a SpO2 of 94% or PaO2 >60 mm Hg; in case of unsuccessful intervention within 30 min, patients were put on reservoir masks with 90%–100% FiO2 or helmet CPAP was initiated with positive end expiratory pressure (PEEP) up to 12 cmH2O based on the respiratory distress and comorbidities following standard operating procedures as previously described.14 CPAP failure after 2 hours with the maximal tolerable PEEP and a FiO2 of 100% was considered in case of: a) persistence of PaO2/FiO2 <300 mm Hg; b) haemodynamic instability (systolic blood pressure <90 mm Hg despite adequate fluid support) or altered consciousness; d) respiratory distress, fatigue and/or a respiratory rate >30 bpm.20 Patients who fulfilled CPAP failure criteria were evaluated by an ICU physician for potential intubation. A do not intubate (DNI) order was established by the treating attending physician following a multidisciplinary discussion with the unit staff and the ICU and based on patient’s age, comorbidities and clinical status.
In-hospital treatment
Unless contraindicated, patients received hydroxychloroquine and lopinavir/ritonavir following local standard and Italian guidelines.21 22 In patients with severe pneumonia, methylprednisolone was given at a maximal dose of 1 mg/kg according to the American Thoracic Society/Infectious Diseases Society of America (ATS/IDSA) guidelines23 and local standard operating procedures. Criteria for methylprednisolone initiation included age <80 years, PaO2/FiO2<250 mm Hg, bilateral infiltrates at the chest X-ray or CT scan, a C reactive protein >100 mg/L and/or a diagnosis of ARDS according to the Berlin definition.17 Immunomodulation with off-label tocilizumab at a dosage of 8 mg/kg body weight was administered in patients with signs of hyperinflammatory syndrome and elevated interleukin-6.21 Unless contraindicated, patients received prophylactic low molecular weight heparin (LMWH) or were switched to therapeutic LMWH dosage if already on chronic anticoagulant therapy. Patients with signs of deep vein thrombosis, pulmonary embolism or D-dimer values >5000 received a therapeutic dose of LMWH.
Statistical analysis
Qualitative variables were summarised with absolute and relative (percentage) frequencies. Parametric and non-parametric quantitative variables were described with means (SD) and medians (IQRs), respectively. Fisher’s exact and χ2 tests were used to compare qualitative variables, whereas Student’s t-test or Mann-Whitney U test, analysis of variance or Kruskall-Wallis, corrected with Sidak adjustment, were used to compare quantitative variables with normal or non-normal distribution, respectively. Cox proportional hazard regression analysis was performed to assess the relationship between clinical outcomes and independent variables. Kaplan-Meier survival curves were plotted to show differences for the outcome mortality, considering the confounding variables age, respiratory failure, PaO2/FiO2 and antihypertensive treatment; log-rank test was computed to assess the presence of any statistically significant differences. A two-tailed p value <0.05 was considered statistically significant. All statistical computations were performed with the statistical software STATA V.16 (StatsCorp, Texas, USA).
Results
Clinical characteristics of the whole sample size
A total of 412 patients were enrolled (280 males, 68%) (table 1). The median (IQR) age at admission was 66 (55–76) years, and 54.6% of patients were ≥65 years of age; 61.8% of patients had a PaO2/FiO2 <300 mm Hg, with a median (IQR) PaO2/FiO2 of 262 (140–343) mm Hg; 24.4% had mild, 21.9% moderate and 15.5% had severe respiratory failure. CPAP was prescribed in the emergency department in 9.7% of cases, whereas only three patients were immediately intubated. Median (IQR) white blood cell (WBC) count was 6.7 (5.1–9.4) per 109/µL, 10.9% had leucopenia and 45.9% had lymphocytopenia. Median (IQR) D-dimer values were 890.5 (470–2157) mg/L fibrinogen-equivalent units (FEU) and 34% had a D-dimer >1000 mg/L FEU (table 1).
Characteristics and outcomes of patients at admission
Half of the patients (50.2%) showed cardiovascular comorbidities, with hypertension being the most prevalent (38.8%). Diabetes and chronic kidney disease were observed in 16.8% and 13.6% of the cases, respectively. Chronic obstructive pulmonary disease (COPD) and asthma accounted for the 6.1% and 3.2% of the study sample. A complete list of observed comorbidities is reported in table 1 of the online supplemental file.
The most frequently administered therapy was hydroxychloroquine (81.6%), whereas corticosteroids and tocilizumab were prescribed in 25.5% and 21.6% of the patients, respectively.
During the hospital stay, 42.7% were exposed to CPAP, 8.7% underwent mechanical ventilation and were transferred to the ICU.
Characteristics based on severity of respiratory failure
The cohort was divided in four groups based on the severity of respiratory failure (table 2). Advanced age and male were more prevalent in patients with severe respiratory failure (p=0.0001 and 0.02, respectively).
WBC, neutrophils, C reactive protein and D-dimer values were higher in severe cases (all p=0.0001). Impaired gas exchange was associated with a decreased lymphocyte counts, ranging from a median (IQR) value of 1.13 (0.84–1.50) per 109/µL in patients with PaO2/FiO2 >300 mm Hg to 0.74 (0.57–0.99) per 109/µL in patients with severe respiratory failure (p=0.0001).
Patients’ characteristics and outcomes depending on the severity of respiratory failure
The proportion of patients with cardiovascular comorbidities and hypertension was significantly higher in patients with a respiratory failure if compared with that of patients with a PaO2/FiO2 >300 mm Hg (p<0.0001). Obesity was more prevalent in patients with moderate and severe respiratory failure if compared with obesity prevalence in patients with PaO2/FiO2 ≥201 mm Hg (23% vs 5.5%; p=0.002); similar differences were found for COPD (22.2% vs 7.2%; p=0.04). Chronic use of ACEi was more prevalent in patients with respiratory failure (p<0.0001).
The highest proportion of intubated patients was in the severe group (17.5%) (table 2).
Impact of cardiovascular diseases and renin-angiotensin-aldosterone system inhibitors
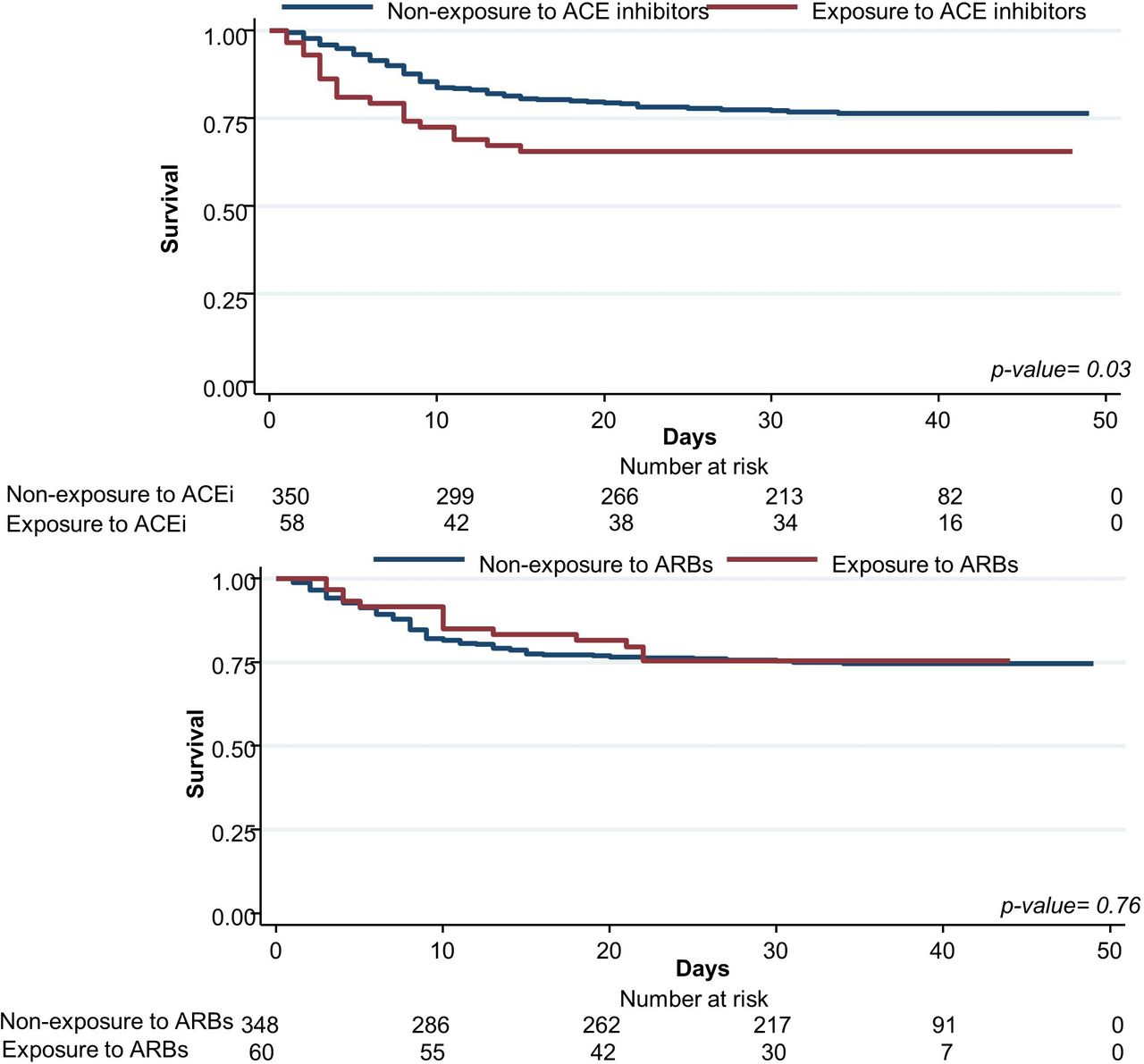
Overall, chronic therapy with ACEi was associated with worse PaO2/FiO2 at admission (median value 223.5 vs 273.0; p=0.004) (table 2 of the online supplemental file) and higher in-hospital mortality (35.6% vs 23.5%; p=0.048) (table 2 of the online supplemental file and figure 1). Severity of respiratory failure at admission, intubation and mortality rates were not associated with ARBs therapy (table 3 of the online supplemental file and figure 1).

Survival curves based on ACE inhibitors (ACEi) or angiotensin receptor blockers (ARBs) exposure. Survival in patients hospitalised with COVID-19 pneumonia (n=412) based on the chronic exposure to ACEi (upper panel) or ARBs (lower panel).
Respiratory failure and outcomes in patients with cardiovascular disease, depending on ACEi and ARBs exposure
Patients with CVD or hypertension had significantly lower PaO2/FiO2 at admission (both p<0.0001), a higher proportion of respiratory failure (both p<0.0001) and an increased need for CPAP during the hospital stay (p=0.02 and 0.003, respectively) (table 4 of the online supplemental file and table 3).
Risk factors for in-hospital mortality
In-hospital mortality and respiratory failure
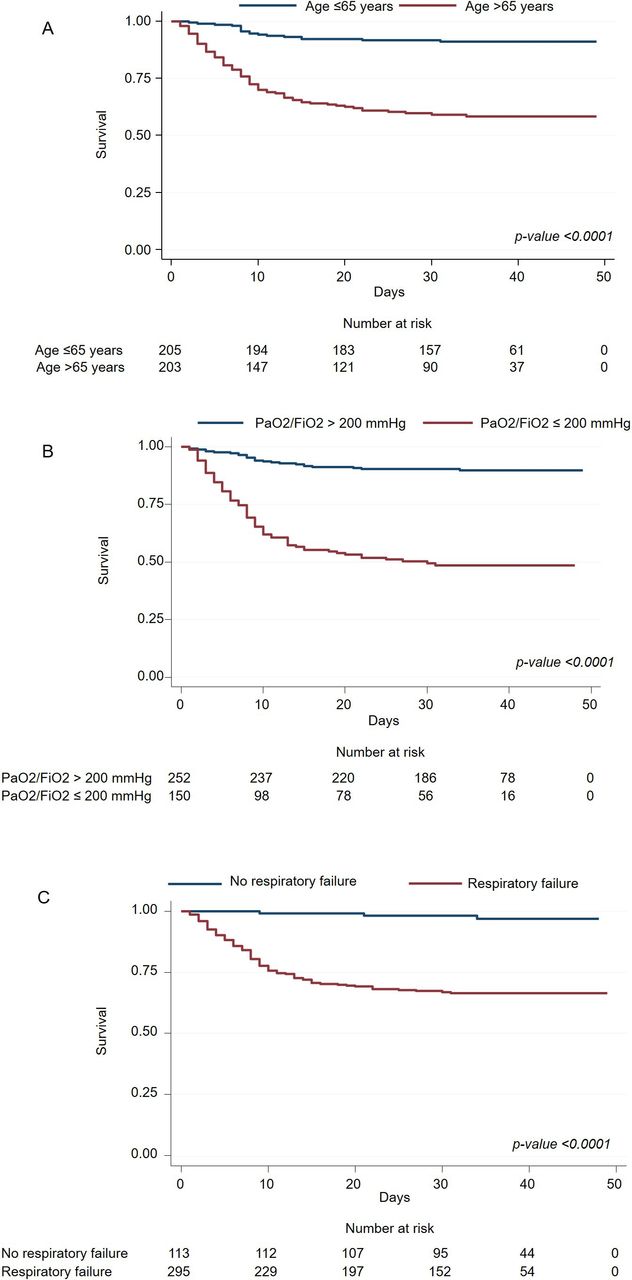
In-hospital mortality was 25.5%. It proportionally increased with lower PaO2/FiO2 values, being highest in the severe group (55.6%) and lowest in patients with PaO2/FiO2 >300 mm Hg (6.5%; p<0.0001). The number of days from admission to death was lowest in the severe group and highest in patients with normal PaO2/FiO2 at admission (p=0.0001) (table 2). Age >65 years, male sex, exposure to ACEi, having a CVD, presence of respiratory failure at admission, a PaO2/FiO2 ≤200 mm Hg and need for CPAP at admission were significantly associated with an increased mortality at the univariate analysis (table 4); however, the multivariate analysis showed that the only independent risk factors were age >65 years (HR 3.41; 95% CI 2.00 to 5.78, p<0.0001), a PaO2/FiO2 ≤200 mm Hg (HR 3.57; 95% CI 2.20 to 5.77, p<0.0001) and the presence of respiratory failure at admission (HR 3.58; 95% CI 1.05 to 12.18, p=0.04) (figure 2). Fifteen days postadmission, patients with moderate-to severe respiratory failure had a survival rate of 56% (figure 2).
{kind=link}
{kind=link}
Survival in patients hospitalised for COVID-19 based on age and severity of respiratory failure. HR for survival in patients hospitalised with COVID-19 pneumonia stratified by age (> or ≤ 65 years, panel A), severity of respiratory failure at admission (PaO2/FiO2 ratio ≤200 mm Hg and >200 mm Hg, panel B) and presence of respiratory failure at admission (panel C). Note that 15 days postadmission, patients with moderate-to-severe respiratory failure had a survival rate of about 56%, while patients without respiratory failure (panel C) had a survival rate of 99%. PaO2/FiO2, partial pressure of oxygen to fraction of inspired oxygen ratio.
Discussion
To the best of our knowledge, the results of the present study demonstrated for the first time the independent relationship between impaired gas exchange and clinical outcomes (mortality, intubation and need for respiratory support).
We showed that age >65 years, presence of respiratory failure and a PaO2/FiO2 ≤200 mm Hg at admission were independently associated with a higher mortality rate. In fact, the mortality risk for patient without respiratory failure at admission was of 1% after 15 days from hospital admission. Conversely, survival in patients with a moderate-to-severe respiratory failure (PaO2/FiO2 ≤200 mm Hg) at admission was only 56% at 15 days. The overall mortality rate in our cohort is comparable to previous reports.5 24 However, it is higher if compared with the mortality described in other observational studies.25 26 Richardson et al reported a prevalence of respiratory failure (SpO2 <90%) of 20.4%,25 whereas it was 72.6% in our cohort. Cheng et al reported an in-hospital mortality as low as 11% in Wuhan, China. However, 58% of enrolled patients were not discharged from hospital at the time of the report,26 whereas only 12% of our cohort was hospitalised at the time of writing.
Hypoxaemia has been rarely considered as a risk factor for patients with COVID-19. Xie et al showed that patients with SpO2 <90% had 47 times more probability to die when compared with patients with SpO2 >90%.27 However, in patients with COVID-19-associated pneumonia, low PaO2 values can be associated with satisfactory SpO2, hiding hypoxia, which might lead to an underestimation of the severity of the disease and in a treatment delay.28 On this basis, clinicians should not rely solely on SpO2 values, especially when evaluating patients in which symptoms had lasted for 10–12 days before their presentation to the emergency department.29 The ratio between PaO2 and FiO2 has been demonstrated to be a reliable tool to assess severity and stratify mortality risk.17 When compared with the ARDS Berlin’s definition, our respiratory failure classes had a slightly higher mortality with PaO2/FiO2 <200 mm Hg (severe 55% vs 45% and moderate 48% vs 35%). This should probably depend on the cohort heterogeneity and in, in our case, the absence of 5 cmH2O of PEEP used in the Berlin definition to grade severity of ARDS. Another issue is the low number of patients with severe respiratory failure at admission who underwent intubation (n=11). This finding can be justified by the higher chance of DNI orders in patients with severe respiratory failure, secondary to the median age and to the higher prevalence of CVD.5 However, the absence of respiratory failure at admission or a mild hypoxia did not preclude the chance of in-hospital death or intubation. Sign of respiratory distress and worsening gas exchange should be closely monitored, as a sudden and rapidly evolving disease can involve patients in stable conditions.29 30
CVD and hypertension are the most frequently observed comorbidities in patients with COVID-19 and are associated with severe disease.31 32 A debate was focused on the negative effects of ACEi and ARBs due to the role of the ACE2 receptor in viral-host dynamics.32 However, several studies ruled out the increased risk of COVID-19 infection and the link between disease severity and antihypertensive treatment.28 31 33 Our cohort was characterised by a high prevalence of CVD (50.2%), which was associated with a significantly higher mortality compared with patients without CVD. However, mortality did not change in patients chronically exposed to ACEi and ARBs. ACEi was associated with a significantly higher mortality, potentially explained by the higher disease severity of at admission of patients taking ACEi. Indeed, neither CVD, nor hypertension, nor the exposure to antihypertensive medications were independently associated with decreased survival.
Study limitations
The initial gas exchange assessment was not homogeneously conducted in all patients at admission (only 30.3% of patients were in room air conditions). This might have underestimated the severity of respiratory failure, especially in patients treated with CPAP at admission. At the time of writing, 12% of patients were still hospitalised, biasing mortality and length of stay estimates. Furthermore, a selection bias could be hypothesised, being the participating centres hub for severe patients transferred from peripheral hospitals. The local standard operating procedures, criteria for ICU admittance or management with CPAP/NIV implemented in Italy could differ in other settings, limiting the inference of our findings.
Conclusions
The severity of respiratory failure assessed with the PaO2/FiO2 ratio is significantly associated with intubation rate, need for respiratory support and in-hospital mortality. Age, respiratory failure and PaO2/FiO2 value at admission are independently associated with in-hospital mortality. Although the findings of the present study need to be confirmed in larger cohorts, they suggest that severity of hypoxaemia can be useful to triage patients with COVID-19 pneumonia and identify patients at higher risk of unfavourable outcomes.
Acknowledgments
The authors would like to thank Dr Roberta Barlassina, CCP, for her help and commitment in data collection. The authors would like to thank all the colleagues, healthcare professionals and employees involved during the COVID-19 pandemic. The corresponding author here confirms that he has listed everyone who contributed significantly to the work.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
PS and DR are joint first authors.
PS and DR contributed equally.
Contributors PS and DR conceived the study and contributed to data collection, analysis and interpretation. GS performed the data analysis and contributed to study design and interpretation. LS performed the analysis and contributed to data interpretation. PM, CC, GDF, MR, EF, SP, FG, MDM, GN, VV and FT contributed to data collection and interpretation. PS, DR, GS and LS drafted and revised the manuscript. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study protocol (ClinicalTrials.gov: NCT04307459), designed following the amended Declaration of Helsinki (2013), was approved by the local ethical committee (Comitato Etico Milano Area I; 17263/2020) and all recruited patients gave written informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement PS and DR had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis and had final responsibility for the decision to submit for publication. The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.