Article Text

Abstract
Objective COVID-19 started spreading widely in China in January 2020. Outpatient fever clinics (FCs), instituted during the SARS epidemic in 2003, were upgraded to serve for COVID-19 screening and prevention of disease transmission in large tertiary hospitals in China. FCs were hoped to relieve some of the healthcare burden from emergency departments (EDs). We aimed to evaluate the effect of upgrading the FC system on rates of nosocomial COVID-19 infection and ED patient attendance at Peking Union Medical College Hospital (PUMCH).
Design A retrospective cohort study.
Participants A total of 6365 patients were screened in the FC.
Methods The FC of PUMCH was upgraded on 20 January 2020. We performed a retrospective study of patients presenting to the FC between 12 December 2019 and 29 February 2020. The date when COVID-19 was declared an outbreak in Beijing was 20 January 2020. Two groups of data were collected and subsequently compared with each other: the first group of data was collected within 40 days before 20 January 2020; the second group of data was collected within 40 days after 20 January 2020. All necessary data, including patient baseline information, diagnosis, follow-up conditions and the transfer records between the FC and ED, were collected and analysed.
Results 6365 patients were screened in the FC, among whom 2912 patients were screened before 21 January 2020, while 3453 were screened afterward. Screening results showed that upper respiratory infection was the major disease associated with fever. After the outbreak of COVID-19, the number of patients who were transferred from the FC to the ED decreased significantly (39.21% vs 15.75%, p<0.001), and patients generally spent more time in the FC (55 vs 203 min, p<0.001), compared with before the outbreak. For critically ill patients waiting for their screening results, the total length of stay in the FC was 22 min before the outbreak, compared with 442 min after the outbreak (p<0.001). The number of in-hospital deaths of critically ill patients in the FC was 9 out of 29 patients before the outbreak and 21 out of 38 after the outbreak (p<0.05). Nineteen cases of COVID-19 were confirmed in the FC during the period of this study. However, no other patients nor any healthcare providers were cross-infected.
Conclusion The workload of the FC increased significantly after the COVID-19 outbreak. New protocols regarding the use of FC likely helped prevent the spread of COVID-19 within the hospital. The upgraded FC also reduced the burden on the ED.
- health services administration & management
- health policy
- public health
- accident & emergency medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study identified the roles of fever clinic and its functional association with the emergency department during the COVID-19 pandemic.
A reasonably large sample size was included over the duration of this study.
The findings of this study can serve as valuable references for hospitals worldwide in the battle against COVID-19.
Our analysis was limited in a single tertiary hospital in Beijing. Comparing the data from this study with the data from other local hospitals would further validate this study.
Introduction
Background
COVID-19, caused by SARS-COV-2, broke out in Wuhan, China, at the end of 2019.1 The number of confirmed cases has rapidly increased since then on a global scale.2 The control of the spread of SARS-CoV-2 is of the primary concern3 at this stage. The main manifestation of COVID-19 includes acute fever, cough and dyspnoea4; therefore, the emergency department (ED) has become the primary facility that provides initial diagnosis and treatment for patients with potential COVID-19. Due to the large number of patients presenting to ED every day, the likelihood of cross-infection and the spread of COVID-19 within the hospital is very likely to occur.5 6 In mainland China, the ‘fever clinic’ (FC) is a separate unit that is affiliated with the ED, specialising in the screening of infectious diseases. They have been designed to protect patients in the ED from those who have contracted infectious diseases.7 The implementation of the FC system was originally suggested by the National Health Commission of the People’s Republic of China during the SARS epidemic in 2003.8 As a result of the successful implementation of the FC system, suspected patients with infectious diseases are not managed first inside the Chinese ED.9 However, after the SARS era, the importance of the FC system in terms of infection control within the hospital has been largely neglected.
FC upgrade post-COVID-19 outbreak
Before the COVID-19 outbreak, four doctors were allocated to the FC of Peking Union Medical College Hospital (PUMCH) where influenza A and B were routinely screened for patients presenting with fever and respiratory symptoms. The FC was also tasked with excluding eruptive infectious diseases (eg, measles, rubella and varicella). Patients with such potential infectious diseases received their initial treatment in the FC; some of them were subsequently transferred to inpatient isolation wards, while others were transferred to the ED for further evaluation and monitoring. After the COVID-19 outbreak, 12 doctors worked in the FC equipped with ‘grade 3’ personal protective equipments (PPEs),10 including a disposable medical-grade protective suit, an isolation gown, an N95 filtering facepiece respirator, goggles, a disposable full-face shield, two layers of clean gloves and boot covers. Two consulting rooms were added to supplement the original single room. The number of medical care providers providing in-person coverage increased from 2 to 9, while the number of nursing staff increased from 9 to 15 per 24 hours. Resuscitation equipments, such as endotracheal intubation tools, central venous catheters, non-invasive and invasive ventilator machines, high-flow oxygen therapy devices and bedside ultrasound, were prepared for use.
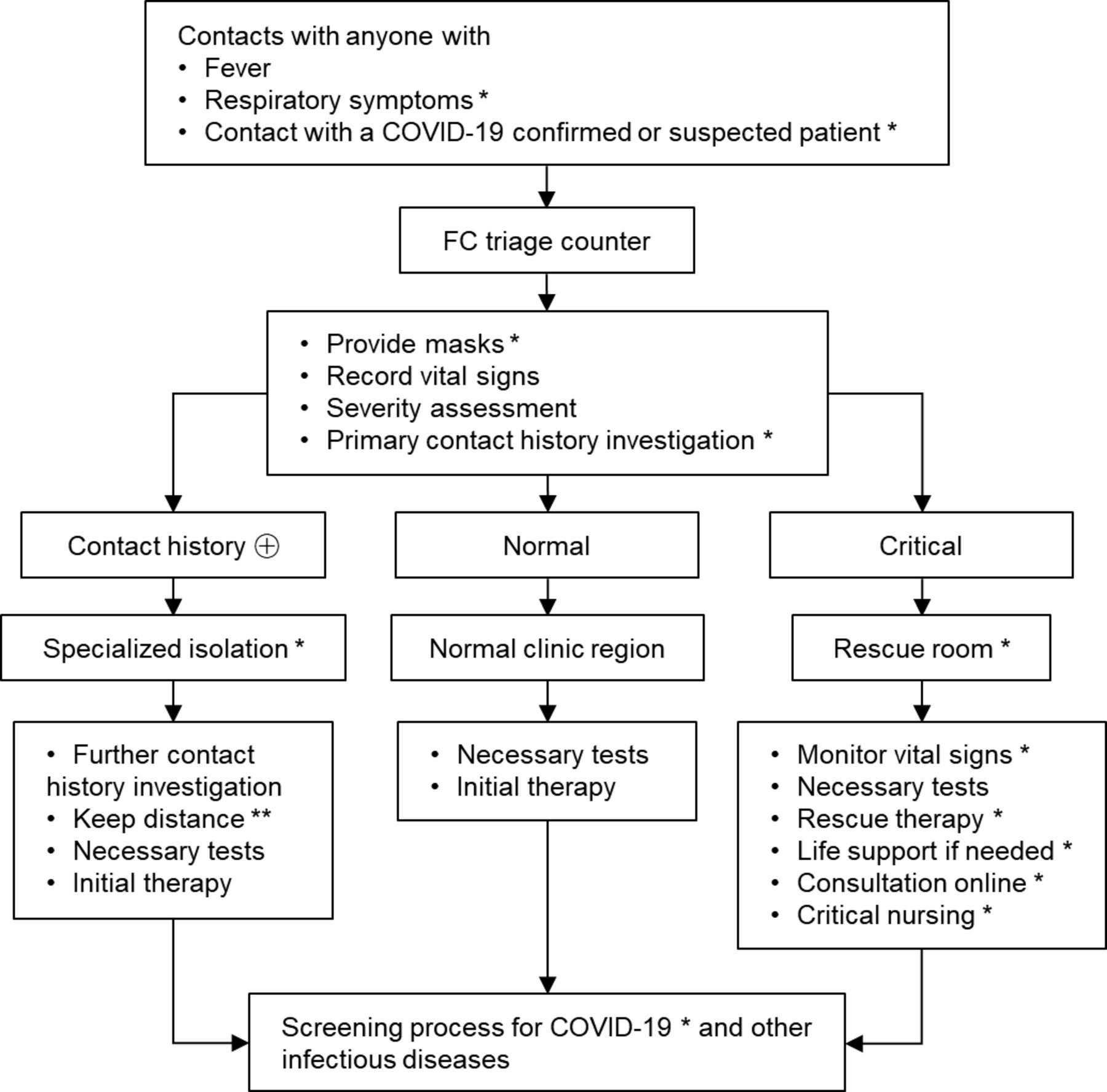
All patients with either fever or respiratory symptoms, regardless of a history of COVID-19 exposure, were instructed to go through the FC triage (figure 1). Each patient was required to wear a mask on arrival to the FC and was allocated to different regions according to their triage history and clinical severity (figure 1). The FC took responsibility for screening SARS-COV-2, in addition to influenza and eruptive infectious diseases. All acquired nucleic acid samples were tested by two independent laboratories licensed by the Beijing Municipal Health Commission for SARS-COV-2 testing. The screening result was only accepted as negative if SARS-COV-2 was not identified by both laboratories. Doctors in the FC were divided into three separate groups that oversaw suspected patients, critical patients and regular patients, respectively. Negative-pressure isolation wards with complete sets of resuscitation equipment were readily available for any critical patients. As soon as the screening tests were reported, patients with confirmed SARS-COV-2 would be immediately transferred to other hospitals that were designated for patients with COVID-19, whereas other patients who needed further treatment were subsequently transferred to the ED (figure 2).
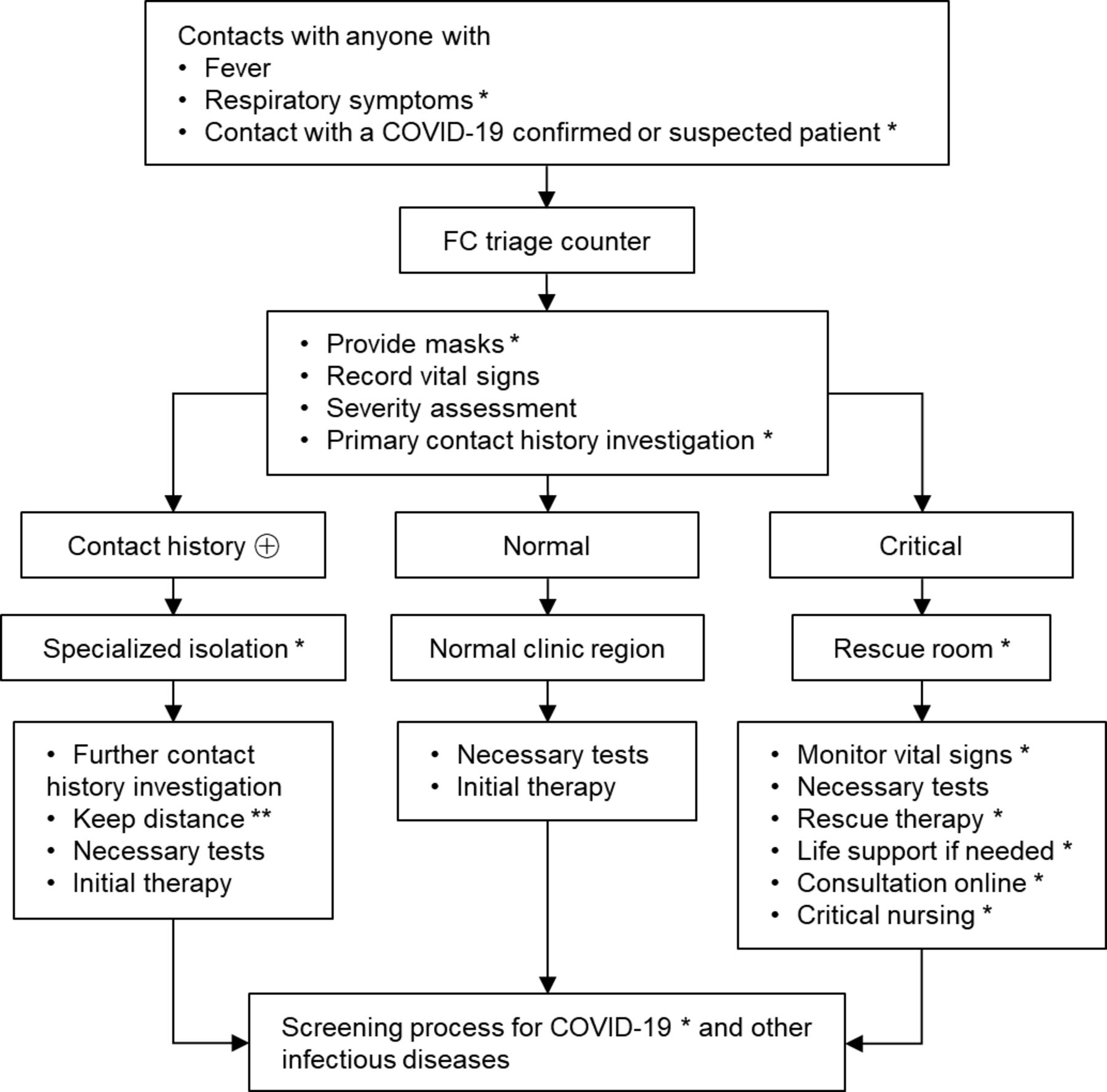
Triage process and regional isolation for different patients in the FC. *Upgraded FC parts. **Educate patients to maintain a person-to-person distance greater than 2 m. ⊕, positive; FC, fever clinic.

{kind=link}
{kind=link}
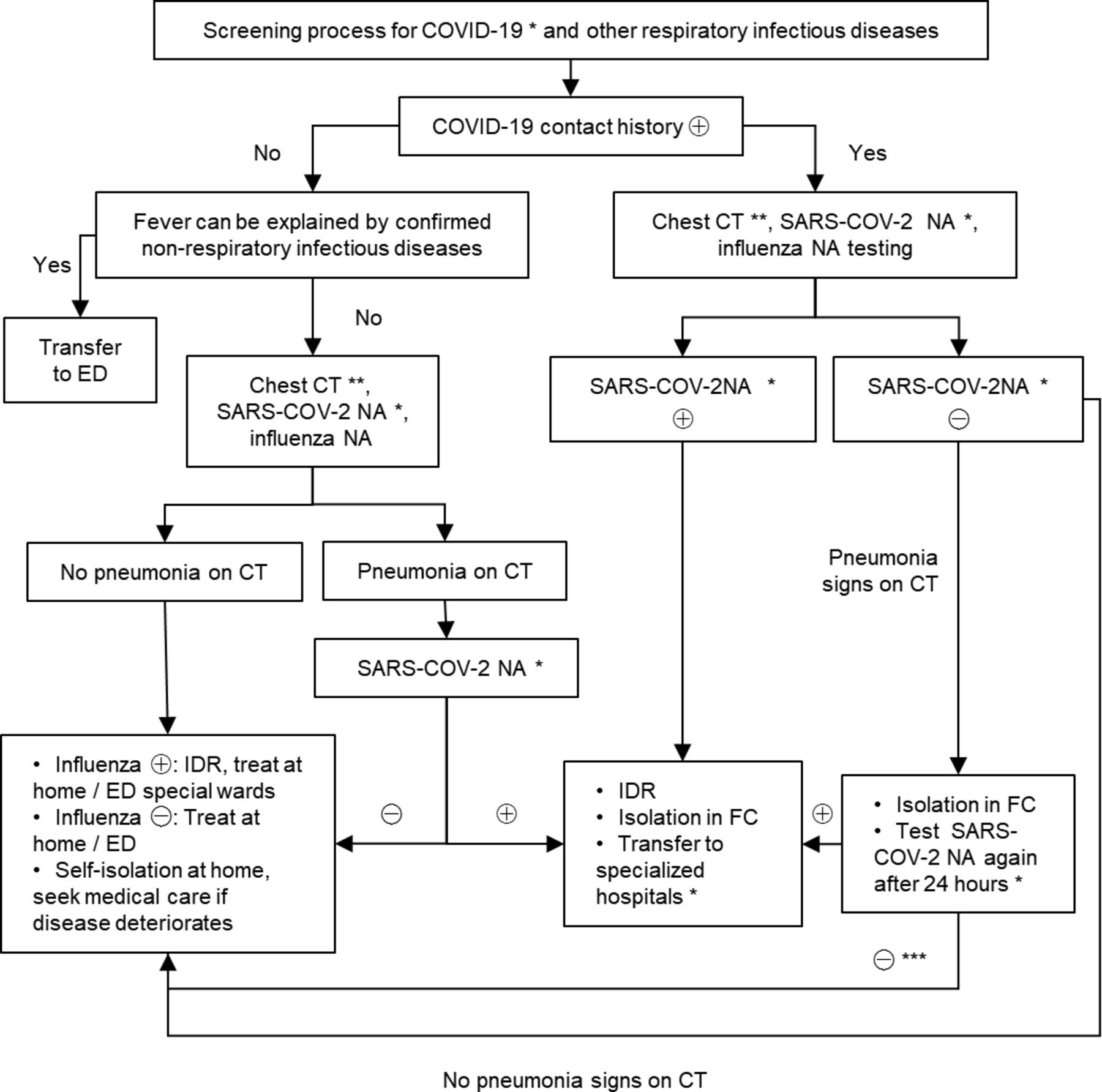
Screening process for COVID-19 and other respiratory infectious diseases. *Upgraded FC parts. **After the COVID-19 outbreak, chest CT was suggested as a routine examination for patients in FC, excluding special populations such as pregnant women and children. ***Patients are recommended to test for SARS-COV-2 RNA again 1 week later even if previous RNA tests were negative twice if they have (1) confirmed COVID-19 contact history; (2) clinical manifestations and lab tests implying viral infection, which can not be explained by other diseases; (3) chest CT strongly suggestive of viral pneumonia. ⊕, positive; ⊖, negative; ED, emergency department; FC, fever clinic; IDR, infectious disease report; NA, nucleic acid.
Methods
Data collection
We collected data from all patients presenting to the FC of PUMCH in the last 40 days before the FC upgrade (from 12 December 2019 to 20 January 2020) and for another 40 days after the FC upgrade (from 21 January to 29 February 2020). The FC was upgraded on 20 January 2020, which was also the official date when COVID-19 was declared an ‘outbreak’ in Beijing. We included all critically ill patients during the period of this study who initially presented to the FC and subsequently transferred to the ED. The data were collected from patients’ medical records and their registration information. Clinical manifestation, primary diagnosis, time of registration and the duration of each consultation were documented for all patients involved in the study.
Critically ill patients were included based on the following criteria: (1) patients who were transferred to the resuscitation room in the ED after initial screening and treatment at the FC, (2) Acute Physiology and Chronic Health Examination II (APACHE II) score of ≥8 and (3) patients who tested negative for COVID-19.11 Critically ill patients’ prognosis and treatment results were documented in their medical records. Changes in patients’ condition (eg, improvement, deterioration or death) within 7 days after their initial presentation at the FC were also recorded.
Patient and public involvement
This was a retrospective study; we collected the medical information of all involved patients from the electronic information system. Patients were not involved in the recruitment for any additional trials or any particular study designs.
Statistics
Statistical Package for Social Sciences V.24.0 software was used for statistical analysis. The Kolmogorov-Smirnov test was used to determine the normal distribution of variables. Variables with normal distribution are shown as mean (±SD). t-Tests were used for variables that followed normal distribution. Data that did not follow normal distribution were shown as a median (25%–75%) and analysed by the Wilcoxon rank-sum test. χ2 tests and Fisher's exact tests were used for enumeration data. P values less than 0.05 were taken to indicate statistical significance.
Results
Patient characteristics and disease aetiologies
In total, 6365 patients were screened in the FC, among whom 2912 patients were screened before the outbreak, and 3453 patients were screened after the outbreak. There was no statistical difference between the two groups for sex, but a significant difference in age was found (p=0.001). The most common diseases found in the FC were upper respiratory infections, followed by abdominopelvic infections and pneumonias (table 1). From 24 January to 11 February, 19 patients were diagnosed with COVID-19 at the FC. All patients with COVID-19 diagnosed in the FC during the study period had mild to moderate symptoms, and therefore, there were no critical cases involving COVID-19 in this study. It is worth mentioning that all patients and medical staff who were in contact with patients with COVID-19 were strictly followed up for 14 days, and no cases of cross-infection were discovered.
Patient characteristics and disease aetiologies
Patient transfer from the FC to the ED
The number of patients who initially presented to the FC and subsequently transferred to the ED before the outbreak was 1142, in contrast to 544 after the outbreak. There was no statistical difference in the sex ratio or age of patients between the two groups (p>0.05). Before the outbreak, 1083 cases (94.8%) of transfer were completed in 24 hours. However, significantly fewer (482 cases, 88.60%) were transferred to the ED within 24 hours (p<0.001) after the outbreak. In addition, patients received a significantly longer duration of treatment in the FC after the outbreak (p<0.001) (table 2).
Patient transfer from the FC to the ED
Critically ill patients
A total of 69 critically ill patients were initially identified in our study. Two patients were subsequently excluded due to an APACHE II score of less than 8 points. Among the remaining 67 patients, 29 visited the FC before the outbreak, while 38 presented after the outbreak. The ratio of the male to the female patients was 1.23:1.0, and their median age was 63 (47–78) years. There was no significant difference in the sex ratio or the age of patients between the two groups (p>0.05). There was also no significant difference in the severity of disease between the two groups when examining their respective APACHE II scores (16.1±6.67 vs 18.74±6.72). Patients with septic shock and pneumonia, combined with respiratory failure, accounted for most diagnosis. The number of in-hospital deaths within 7 days among critically ill patients seen in the FC was 9 out of 29 before the outbreak, and 21 out of 38 after the outbreak (p<0.05) (table 3).
Characteristics and disease aetiologies of critically ill patients
Length of stay in the FC and the ED
The total length of stay in the FC was 22 (12–47) min before the outbreak, compared with 442 (374–636) min after the outbreak (p<0.001). In addition, the total length of stay in the resuscitation room of the ED lengthened from 22 (7–59) hours to 48 (21–96) hours (p<0.001) (table 4).
Length of stay in the FC and ED
The most commonly provided types of treatment in the FC were antibiotic, antiarrhythmic, antihypertensive and antiplatelet medications. Common supportive treatments included nasal catheter oxygen, non-invasive/invasive ventilation, fluid resuscitation, vasopressors, intracranial pressure-lowering medications and diuretic medications. The initial treatment times are shown in table 4.
Discussion
COVID-19 is a novel infectious disease of the respiratory system. It has become a notifiable infectious disease since 20 January 2020 according to the National Health Commission of the People’s Republic of China. From 20 January, the Beijing Municipal Government initiated a level 1 (highest) public health response to prevent the spread of COVID-19.12 The FC of PUMCH was upgraded in response to the disease outbreak. In this study, we analysed the recorded patient data taken from the FC in the 40 days pre-COVID-19 and post-COVID-19 outbreaks. We found that after the outbreak, the FC had played a more important role in delivering treatment to critically ill patients. Therefore, those patients were able to undergo their initial management in the FC rather than in the ED. Some patients were subsequently transferred to the ED for further treatment if they had been tested negative for SARS-COV-2 by two different laboratories. As a result, no COVID-19 cases were transferred or identified in the ED during 40 days of the postoutbreak period. More surprisingly, no patients, doctors or nurses in other departments of the hospital were cross-infected with COVID-19. Therefore, this FC upgrade strategy is strongly suggested to have contributed to the successful prevention of the spread of COVID-19 within the hospital.
According to our data, upper respiratory infections were most commonly seen in the FC both before and after the COVID-19 outbreak. Most patients with mild COVID-19 had upper respiratory infection syndromes13; these patients were also strongly infectious and posed a substantial screening challenge. It was not possible to exclude COVID-19 merely based on clinical symptoms alone.14 The average age of patients tended to be older after the outbreak.15 A reasonable explanation for this was that patients with relatively severe diseases had to seek medical care in hospitals even though they faced a high risk of cross-infection with COVID-19. Older people generally have a higher risk of developing severe diseases, but the difference in age between the two groups did not exist in critically ill patients in our study, which could be attributed to the fact that most critically ill patients were older.
Every patient staying in the FC was considered as a potential source of infection, and preventing the spread of potentially contagious diseases to the rest of the ED and hospital was a key mission of the FC. Before the outbreak, the major work of the FC was to identify influenza, which would usually take only 30 min. Once a patient was confirmed to not have influenza, they would be allowed to be transferred to the ED with limited precautions. However, after the COVID-19 outbreak, data showed that there was a decrease in the number of transfer patients from the FC to the ED in order to reduce the likelihood of overcrowding the ED. Less crowding in the ED also likely lessened the chances of cross-infection. Traditionally, the FC was tasked with screening and providing initial supportive treatment to patients. After the outbreak, the FC needed to perform an additional task by offering more comprehensive treatment. For FC patients who needed further medical management in the ED, they could only be transferred until being tested negative for SARS-COV-2. Patients and medical staff in the ED were protected from contracting COVID-19 by the FC, but the FC had to expand to support patients during the ‘rule-out’ phase of testing.
Intensive screening also played an important role in COVID-19 testing. Before the outbreak, having a fever was the only screening indicator for all patients. Unfortunately, 11.5% of patients with COVID-19 do not present with fever, while 82.4% of patients develop respiratory symptoms, such as cough, expectoration and dyspnoea.12 This led to a modification of the FC inclusion criteria to now include (1) patients with a positive COVID-19 contact exposure, (2) patients presenting with fever and (3) patients with respiratory symptoms. With the new criteria in place, the number of FC patients grew dramatically in the 40 days after 20 January 2020.
Multiple testing methods were trialled to decrease false-negative rates. As COVID-19 showed diverse manifestations, it was unreliable to identify this disease based on only one method. In our screening process, multiple methods, including blood cell analysis, chest CT,16 SARS-COV-2 nucleic acid17 and antibody tests,18 were used to screen for this disease. However, each method had its own false-negative risks; therefore, all patients suspected of any viral infection were recommended to receive a further nucleic acid test 24 hours after the first test. This method helped assure that FC patients who were subsequently transferred to the ED possessed a minimal risk of spreading COVID-19 in the hospital. In addition, to avoid false-negative results, patients with the following conditions were recommended for repeat SARS-COV-2 nucleic acid testing again after 1 week: (1) confirmed COVID-19 contact history; (2) clinical manifestations and lab testing suggesting a viral infection that is unexplained by another disease; and (3) chest CT indicating viral pneumonia, despite previous negative nucleic acid testing. With these strict screening criteria imposed, no COVID-19 cases were diagnosed among patients in the ED during the period of this study.
An effective triage strategy also reduced the risk of cross-infection. As the number of FC patients increased rapidly, the prevention of cross-infection become a major concern. According to patients’ COVID-19 contact history and clinical severity, they were allocated to one of three specialised sections of the FC. One of the sections was designated for patients who had a positive contact history. Such patients were quarantined in this section pending negative SARS-COV-2 testing while keeping a person-to-person distance of at least 2 m. For the second section, critically ill patients identified at the triage counter were quickly brought to resuscitation rooms in the FC, where experienced physicians would provide further assessment. Once negative results were reported for SARS-COV-2, they were transferred to the ED resuscitation rooms. For patients deemed least likely to have COVID-19 who did not require resuscitation, they would receive their treatment in the third section, where they would see a doctor and start SARS-COV-2 testing.
After the COVID-19 outbreak, PPE worn by healthcare workers in the FC was upgraded to a higher infection-control standard. All consulting rooms and observation rooms were negative-pressure rooms. Each consulting room was sterilised by ultraviolet light for 1 hour every day and by alcohol (75%) spray on all the surfaces (eg, desks, computers, keyboards and printers) once every 4 hours. Negative-pressure airborne infection isolation observation rooms were also sterilised by ultraviolet light for 1 hour every day even when no patients were admitted. When a patient left an observation room, ultraviolet light sterilisation and alcohol spray for surfaces were performed immediately.
This study showed that the 7-day mortality rate for critically ill patients was 55.26% (21/38) after the outbreak. In contrast, the mortality was 31.03% (9/29) before the outbreak. There are likely several reasons underlying this difference in mortality . First, the sample size was small in both groups, thus creating sampling error. Second, 2 patients from the 9/29 group and 7 patients from the 21/38 group actually carried ‘do not resuscitate’ (DNR) orders. If these DNR patients were excluded from their respective study groups, the mortality rates would narrow to 24.13% (7/29) in the first group (before the outbreak) and 36.84% (14/38) in the second group (after the outbreak). Third, a new policy at PUMCH during the COVID-19 outbreak stated that critically ill patients from the ED could not be quickly admitted into the intensive care unit and other specialist wards, in order to prevent the spread of COVID-19 in the hospital. This resulted in a longer duration of stay in the ED, likely negatively affecting the overall prognosis of critically ill patients, regardless of FC stay.
Strengths and limitations
This study had several limitations. It was a retrospective study at a single centre and carried the associated weaknesses of such study methodologies. Nevertheless, given the seriousness of the global battle against COVID-19, the findings related to FC upgrades and the coordination between FC and ED are potentially important and valuable. Future studies would benefit from examining the effects of integrating FC with other parts of the hospital to encourage even more efficient screening and infection prevention pathways.
Conclusion
This retrospective study demonstrated the effect of changes implemented in the FC system in response to the COVID-19 outbreak. All modifications to the FC were designed to improve the efficiency of triage and to lower the risk of spreading COVID-19 to the ED and other parts of the hospital. The upgraded FC also was able to lessen the burden on the ED by providing more extensive treatment for patients than in the past. Although further studies are needed to examine the best role of the FC in fighting COVID-19, this study detailed how the FC system can play a significant role in preventing the spread of COVID-19 in a large, tertiary teaching hospital. By implementing an effective FC system that works in parallel with the ED, hospitals may provide efficacious patient management while protecting the rest of the hospital.
Acknowledgments
We thank all the healthcare providers working in the fever clinic and emergency department of Peking Union Medical College Hospital during the COVID-19 pandemic for their dedication and professionalism during this challenging time.
Footnotes
JW and LZ contributed equally.
Contributors JW and JL were responsible for the conception and design of the study. JW, HS, PS, SX, YaL, JX and CW contributed to the literature search and data collection. LZ and FL oversaw the statistical analysis and data interpretation. LZ, JW and JZ took part in drafting the manuscript. JHW, XY, YiL and HZ revised and approved the final version of the manuscript. All authors read and approved the final submitted version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the ethics committee of the Peking Union Medical College Hospital (ref S-K1091). All of the data used in this study were anonymised before its use.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. Extra data can be accessed via the Dryad data repository (http://datadryad.org/, doi: 10.5061/dryad.rjdfn2z84).