Article Text

Abstract
Purpose To describe the rationale, methods and research potential of eye and vision measures available in UK Biobank.
Participants UK Biobank is a large, multisite, prospective cohort study. Extensive lifestyle and health questionnaires, a range of physical measures and collection of biological specimens are collected. The scope of UK Biobank was extended midway through data collection to include assessments of other measures of health, including eyes and vision. The eye assessment at baseline included questionnaires detailing past ophthalmic and family history, measurement of visual acuity, refractive error and keratometry, intraocular pressure (IOP), corneal biomechanics, spectral domain optical coherence tomography (OCT) of the macula and a disc–macula fundus photograph. Since recruitment, UK Biobank has collected accelerometer data and begun multimodal imaging data (including brain, heart and abdominal MRI) in 100 000 participants. Dense genotypic data and a panel of 20 biochemistry measures are available, and linkage to medical health records for the full cohort has begun.
Findings to date A total of 502 665 people aged between 40 and 69 were recruited to participate in UK Biobank. Of these, 117 175 took part in baseline assessment of vision, IOP, refraction and keratometry. A subgroup of 67 321 underwent OCT and retinal photography. The introduction of eye and vision measures in UK Biobank was accompanied by intensive training, support and a data monitoring quality control process.
Future plans UK Biobank is one of the largest prospective cohorts worldwide with extensive data on ophthalmic diseases and conditions. Data collection is an ongoing process and a repeat of the baseline assessment including the questionnaires, measurements and sample collection will be performed in subsets of 25 000 participants every 2–3 years. The depth and breadth of this dataset, coupled with its open-access policy, will create a powerful resource for all researchers to investigate the eye diseases in later life.
- epidemiology
- dementia
- medical retina
- medical ophthalmology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
UK Biobank is the largest prospective cohort with extensive measures on ophthalmic diseases and conditions.
Repeated physical measures every few years and linkage to National Health Service records will provide valuable information on health outcomes.
A large number of incident cases of eye diseases in 5 years will allow the detection and quantification of small effect sizes.
A low response rate (5.5%).
Introduction
Ageing populations worldwide face an increasing burden of chronic and neurodegenerative diseases,1 resulting in substantial health and economic burdens.2 3 Chronic age-related eye diseases, such as age-related macular degeneration (AMD), diabetic retinopathy (DR) and glaucoma, are leading causes of visual impairment in Western populations. Increased intraocular pressure (IOP) is one of the most significant risk factors for the development4 and progression5 of glaucoma. A recent study from the UK Biobank demonstrated that factors including diabetes, height, smoking and black ethnicity have different associations with Goldmann-correlated IOP (IOPg) and corneal-compensated IOP (IOPcc).6 Hence, suggesting that these factors are related to corneal biomechanical properties. In another UK Biobank study, 67 321 participants underwent optical coherence tomography (OCT) imaging of both eyes.7 The OCT is a non-invasive imaging system that provides high-resolution, cross-sectional images of the retina, retinal nerve fibre layer (RNFL) and the optic nerve, aiding in the diagnosis and management of eye diseases.8 Loss of vision due to eye diseases has a considerable impact on an individual’s activities and quality of life.9 10 Identifying modifiable risk factors of common disabling diseases of later life may help develop preventive strategies. These conditions are often caused by a combination of genetics, environmental and lifestyle factors. Built on a foundation laid by the Human Genome Project,11 the last decade has seen dramatic advances in the understanding of molecular mechanisms in the human health and disease. A myriad of studies using traditional linkage methods and genome-wide association studies12–14 have now raised questions about the role of gene–gene (GxG) and gene–environment (GxE) interaction in determining disease susceptibility.15 16 Extensive information on environment and lifestyle in conjunction with biological samples are crucial to assess GxE interactions.
To avoid the potential for reverse causality and minimise recall bias, exposures should be measured before they are affected by disease or its treatment. Prospective cohorts offer many advantages for assessing the combined effects of genes, environment and lifestyle factors and its association with various health outcomes. The prospective nature of these cohorts allows the exposures to be recorded before the disease onset, and a wide range of diseases to be investigated, including those that may be challenging to study retrospectively.17 Furthermore, the overall beneficial and adverse effects of a specific exposure on the lifetime risks of numerous diseases can be examined. Only a small proportion of individuals will develop the disease and the effects of various exposures on disease development are likely to be modest. Hence, to address questions of GxG and GxE interaction, prospective studies need to include a large number of participants, with several hundred thousand participants.18 19 However, there is a lack of large prospective studies at such a scale that allow investigation of risk factors or gene–environmental interaction of eye diseases.
UK Biobank (https://www.ukbiobank.ac.uk/) is a large-scale multisite cohort study, conceived to provide a resource for the scientific community to examine genetic and environmental risk factors for complex diseases of middle and old age in the UK population. UK Biobank has collected extensive baseline questionnaire data, physical measures and biological samples, with comprehensive follow-up and characterisation of many different health outcomes.20 Towards the end of the baseline phase, the UK Biobank Steering Committee advised the broadening of the scope of the study to include more detailed examination of participants, including assessment of arterial stiffness, a hearing test, additional cognitive function tests, cardiorespiratory fitness, collection of whole blood and saliva, as well as an examination of eyes and vision. The UK Biobank eye and vision data provide researchers with a unique opportunity to access a very large dataset containing detailed ocular phenotypic information, together with rich biomarker variables, dense genotyping and extensive information on lifestyle variables, medical history and healthcare episodes, thus giving unique research resource. As such, UK Biobank offers comprehensive data to explore novel aetiological associations, risk factors and to make evidence-based recommendations on policy. This report aims to describe the methods and the baseline characteristics of the participants who underwent eye and vision assessment in UK Biobank.
Cohort description
Whole UK Biobank cohort
UK Biobank is a large, multisite, study of 502 656 UK residents aged between 40 and 69 years who were registered with the National Health Service (NHS). The overall study protocol (http://www.ukbiobank.ac.uk/resources/) and protocols for individual tests (http://biobank.ctsu.ox.ac.uk/crystal/catalogs.cgi) are available online. Briefly, extensive baseline questionnaires and physical measures were obtained from 22 assessment centres between January 2006 and October 2010.20 21 This included data on sociodemographics, family history and early life exposures, psychosocial, environmental, lifestyle, environmental and health status, hearing threshold and cognitive function as well as self-reported medical conditions. In addition to the baseline questionnaire, web-based questionnaires were included to obtain data on dietary intake, occupational history, cognitive function, mental health and gastrointestinal symptoms. In addition, mailed triaxial accelerometers will supplement the physical activity data in 100 000 participants.20
Physical examination included blood pressure, heart rate, hand grip strength, anthropometrics, spirometry, bone density, arterial stiffness, fitness test. Biological samples, including stored blood, urine and saliva samples, were collected to allow many different types of assay (eg, genetic, proteomic, metabolomics, biochemical and haematologic), (https://www.ukbiobank.ac.uk/)22 23 providing a uniquely rich resource for investigating aetiological risk factors and thereby assisting in the prevention and treatment of many different conditions. The UK Biobank Axiom array was used for genotyping and the methods have been described in detail.23 Furthermore, UK Biobank launched the world’s largest health imaging study in 2014 (www.imaging.ukbiobank.ac.uk) that aims to perform MRI of brain, heart and abdomen, carotid ultrasound and dual-energy X-ray absorptiometry body scans on 100 000 participants.24 A detailed follow-up of participants over a 20-year period is envisaged through data linkage to national electronic medical records. Thus, linking to NHS will provide valuable information on health outcomes (eg, mortality, cancer registrations, hospital admissions, primary care data, etc).
The key ethics and governance principles relating to UK Biobank are laid out in the Ethics and Governance Framework,22 prepared by the project funders. Major funders include Medical Research Council (MRC) and Wellcome Trust, while other funding bodies include Department of Health (DoH), Scottish Government and the Welsh Government, North West Development Agency, British Heart Foundation and Diabetes UK. All participants provided informed consent.
UK Biobank eye and vision subcohort
Study location
Ocular measurements commenced in late 2009 at six assessment centres as an additional enhancement to the initial baseline measures. The six centres are distributed across the UK, including Croydon and Hounslow in Greater London, Liverpool and Sheffield in Northern England, Birmingham in the Midlands and Swansea in Wales.6
Examination procedures
Questionnaires
Self-reported eye diseases, including glaucoma, DR and AMD, were obtained from self-administered questionnaires.
Measurements
The methods and protocol for the ocular examination component were designed by ophthalmologists from Moorfields Eye Hospital (MEH), London, UK. The core funding for the examination was provided by the Wellcome Trust, the MRC and the DoH. Additional support for training, implementation and quality control came from the NIHR Biomedical Research Centre at MEH. All ocular examinations were undertaken by trained personnel to ensure that the ocular measurements were acquired in a stepwise manner using standard operating procedures or instructions, and they had to pass a structured examination before the project started. The entire process including the teaching material was reviewed and moderated by an ophthalmologist from MEH, London, UK. The ocular examinations were conducted without pharmacological mydriasis and took an average time of 11 min to complete.7 Baseline eye examination was conducted from June 2009 to July 2010, subsequently, from August 2012 to June 2013, a subset of approximately 20 000 underwent follow-up examination, including all eye measures.
Visual acuity
Visual acuity (VA) was measured using a logarithm of the minimum angle of resolution (LogMAR) chart (Precision Vision, LaSalle, Illinois, USA) on a computer screen under standard illumination. It follows the British Standards Institute,25 and the right eye was measured first. The test was performed with participants wearing the distance refraction at 4 m, or at 1 m if a participant was unable to read. Participants were asked to read each letter from the top of the chart and down as far as possible. The test was terminated when ≥2 letters are incorrect and recorded as LogMAR VA.
Refraction
Non-cycloplegic autorefraction was performed using the Tomey RC-5000 Auto Refkeratometer (Tomey, Nagoya, Japan) and the right eye was measured first. For each eye, up to 10 measurements were taken and each measurement had a score between 0 and 9 (smaller scores indicate more reliable measurements). To ensure measurements were reliable, each reading achieved a score of ≤4.26
Intraocular pressure
IOP was measured using the Ocular Response Analyzer (ORA) (Reichert, Philadelphia, Pennsylvania, USA).27 One measurement was taken for each eye and the right eye was measured first. The ORA uses a rapid pulse air to indent the cornea and an electro-optical system records the corneal deformation. Two applanation measurements are recorded: (1) while the cornea moves inwards, achieving a first applanation state or flattening (P1); (2) when the cornea recovers from its slight concave state as the pressure decreases, and the cornea passes through a second applanated state (P2). Hence, P1 and P2 are air pressures that correspond with the two applanation states of the cornea.28 The average of the 2 ORA pressure values was calibrated against Goldmann applanation tonometer to derive IOPg (mm Hg) A separate IOPcc reading (IOPcc=P1 and 0.43*P2) was derived to limit the difference before and after laser-assisted in situ keratomileusis (LASIK) surgery and has, therefore, limited influence from corneal biomechanics than those provided by Goldmann applanation tonometer.27 29
Corneal hysteresis
Corneal hysteresis (CH) is considered an indicator of corneal viscous energy damping and is derived as the difference between P1 and P2: CH=P1 and P2.27 28
Optical coherence tomography
OCT images were obtained using a spectral domain OCT 3-dimensional (3D OCT-1000 Mark II, Topcon, Japan). The scans were conducted in a darkened room under standard illumination without pupil dilation using a 3D macular volume scan (512 horizontal A-scans/B-scan; 128 B-scans in a 6×6 mm raster pattern). The methodology of the OCT imaging has been described previously.7 30
Fundus photography
Colour photographs of the optic disc and macular were acquired using a Topcon 3D OCT-1000 Mark II system. The Topcon 3D OCT-1000 has a field angle of 45°, a digital zoom (2X, 4X), scanning range of 6×6 mm, 4.5×4.5 mm, 3×3 mm and a scanning speed of 18 000 A-scans per second. The horizontal and longitudinal (depth) resolutions were ≤20 µm and 5–6 µm, respectively.31
Data monitoring and quality assessment feedback
Daily monitoring of data collection was performed by UK Biobank using a custom-designed monitoring software (WACMAN). The WACMAN software monitored the data items collected and allowed individual operator’s performance to be reviewed—the number of measurements skipped and the degree to which the data collected by the operator lay within the range of expected values. The performance of the technicians responsible for ophthalmic imaging was monitored to provide feedback to those producing substandard quality images within three working days. This was achieved by grading the first 100 photographs of each technician and at least 5% of all OCT images.
Patient and public involvement
UK Biobank maintains a website to keep participants and researchers up to date on the study, which contains a news feed (http://www.ukbiobank.ac.uk/news/) and feedback service. In addition, UK Biobank has a twitter feed.
There is an annual scientific meeting which is recorded and available to the public as webcast.
The study was set up by the MRC, DoH and Wellcome Trust with input from major patient representative organisations (British Heart Foundation and Cancer Research UK) http://www.ukbiobank.ac.uk/public-consultation/
Statistical analysis
The baseline ocular characteristics were analysed and presented as mean±SD for continuous variables and number (%) for categorical variables. Statistical analyses were performed using STATA software V.13.0 (StataCorp).
Results
Findings to date
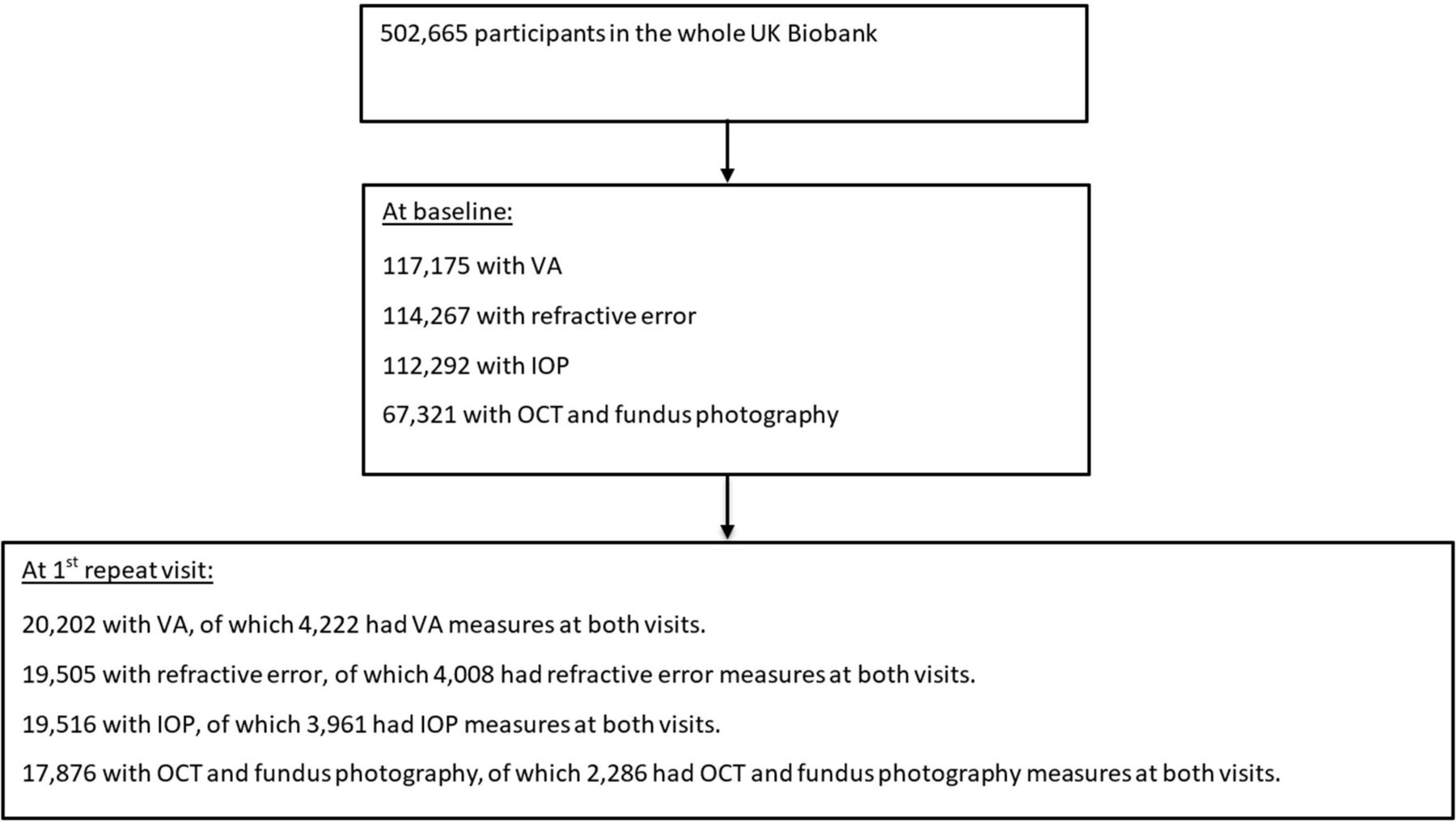
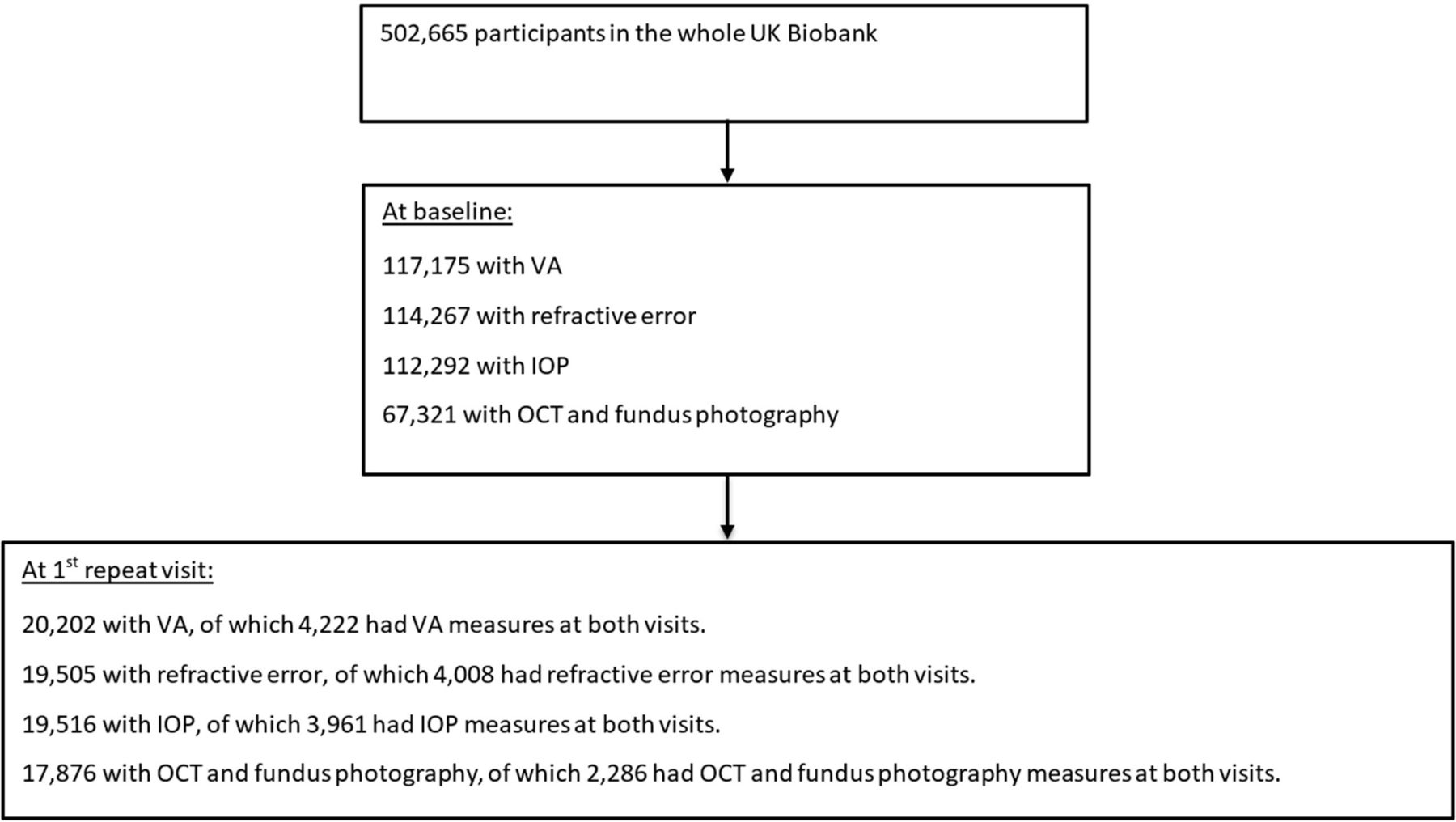
In total, ocular measures including VA, refraction and IOP data were measured in approximately 117 175 people aged 40–69 years. Of these, OCT imaging and fundus photography were performed in 67 321 (57.5%) participants. Figure 1 describes the number of participants with eye measures at baseline and first repeat visit. Table 1 describes the baseline characteristics of participants in the total cohort, and among participants with various ocular measurements at baseline and at first repeat visits. Compared with the whole UK Biobank cohort, participants with baseline VA and OCT measures consisted of a higher proportion of Asians, blacks and mixed/others ethnic groups and had more positive Townsend Deprivation Index. Compared with participants with baseline eye measures, those with repeat visit of VA or OCT data were older, more likely male, of white ethnic background, had the educational level of degree and above, had more negative Townsend Deprivation Index or better socioeconomic status and less likely to smoke.
{kind=link}
Flow chart of participants with the eye measures at baseline and first repeat visit in the UK Biobank. IOP, intraocular pressure; OCT, optical coherence tomography; VA, visual acuity.
Comparison of baseline characteristics between participants in the whole UK Biobank cohort and those with various ocular measurements
Table 2 summarises the number of participants completing each test and the summary measures for these tests. The VA and refractive error measures were quite similar at baseline and at the first repeat visits. Mean VA was approximately 0.0 LogMAR at both visits. At both visit, the mean spherical equivalent refraction was −0.3 D. Approximately 60% of participants were non-myopic, while the proportion of participants with low, moderate and high myopia were 24%, 11% and 5%, respectively. Participants’ mean IOP was slightly higher at first repeat visit than at baseline. The mean IOPg ranged from 15.7 mm Hg to 16.2 mm Hg, while IOPcc ranged from 16.0 mm Hg to 16.5 mm Hg. The proportion of participants with ocular hypertension was 12% at baseline and 16% at first repeat visit. Projected number of new cases of eye diseases including AMD, cataract and primary open angle glaucoma (POAG) expected to occur among the whole UK Biobank cohort and subcohort during the period of 25 years follow-up (table 3).32 By 2023, the expected number of new cases of any AMD, cataract and POAG were around 11 753, 107 702 and 8704 in the whole cohort, respectively, with around 14% of these cases occurring in the ocular subcohort. From 2023 to 2033, the expected number of new cases of any AMD increased by 3.5 times, while the expected number of cataract and POAG increased by two times.
Ocular characteristics of participants in the UK Biobank at baseline visit and at the first repeat visit
Predicted number of new cases of eye diseases expected to occur during the first 25 years of follow-up in UK Biobank
Findings from the UK Biobank eye data showed that first-born individuals were more often myopic than non-first-born,33 which confirms previous findings.34 35 New findings include the discovery of 112 loci, including 68 novel loci, associated with IOP and the development of POAG. Several loci suggest the importance of angiopoietin-receptor tyrosine kinase (ANG-TEK) in signalling IOP regulation, thus suggesting ANG-TEK to be a therapeutic target. In individuals without neurodegeneration, thinner RNFL was associated with worse cognitive function and more likely to have future cognitive decline.36 The use of deep-learning models predicted cardiovascular risk factors such as age (mean absolute error within 3.26 years), gender (area under the curve (AUC)=0.97), smoking status (AUC=0.71), systolic blood pressure (mean absolute error within 11.23 mm Hg) and major adverse cardiac events (AUC=0.70).37
Discussion
Common age-related eye diseases, including AMD, DR, glaucoma and myopia, are leading causes of visual impairment,38 and have both genetic and environmental contributions. Smoking and age are the most consistently observed non-genetic risk factors for AMD,39 and several established genetic risk factors have been identified.40 41 Significant gene–environmental interactions have been identified for complement factor H gene and smoking for AMD.42 However, limitations exist and generalisability of the findings is uncertain. Hence, future prospective studies of larger sample size would help to clarify the issue. The UK is in an ideal position to undertake ambitious ‘big data’ health sciences research, given the extensive coverage of the NHS and various detailed health record systems. UK Biobank has begun to harness these strengths to deliver epidemiological research at scale. Repeating detailed physical measures every few years in subsets of 20–25 000 participants adds a powerful longitudinal dimension, with health-related outcomes being tracked through linkage to NHS records including death and cancer registers, hospital inpatient and outpatient episodes and primary care. Other health record linkage including data from national mental healthcare, residential history, laboratory and disease audit datasets, National Ophthalmology Database Audit, OpenEyes, Medisoft Ophthalmology, and may also include imaging, cancer screening and dental.20 To enhance accurate identification of health outcomes, additional methods such as cross-referencing against NHS case records, imaging and eye data or banked tissues will be used for validation and subclassification.
Scope of eye data
UK Biobank is among the largest eye and vision datasets globally. By 2023, >11 000 incident cases of AMD, >8000 cases of POAG and about 107 000 cataract surgeries will have occurred in the whole UK Biobank cohort.32 This large number of new cases of eye diseases will provide substantial power for nested case–control studies to detect the main effect OR of 1.3 or higher.43 With the rise in ageing population, the rates of chronic eye diseases will increase. However, the rates of undiagnosed eye diseases remain high. Population-based studies reported that at least 50% of whites,44–47 and 55%–90% of Asians48–50 have undiagnosed glaucoma. Approximately 70% of undiagnosed cataracts were reported in USA51 and Singapore.52 In addition to undiagnosed eye conditions, people were found to be unaware of their eye conditions. Previous population-based reported that only 5%–46% of those identified as having an eye disease (eg, AMD,53 cataract,53 glaucoma and DR,54 accurately self-reporting their disease).55 Hence, linking to electronic health records is essential to ensure accuracy in identification of eye diseases. In UK Biobank, the overall self-reported glaucoma rate was 1.7% among people aged 40–69 years.56 This rate appears to be lower compared with White populations aged 40 years and older in the USA (2.08%),46 Australia (2.0%)57 and Italy (2.9%).58
Retina and the cardiovascular system
Retinal imaging has provided probably the richest data relating to eyes and vision in UK Biobank. In addition to giving unprecedented power to examine diseases of the eye, retinal morphometry can give insights into the diseases of the vascular and neurological systems. The retina shares similar embryological origin, anatomical features and physiological properties with the brain,59 it offers an accessible site to investigate the central nervous system in vivo.60 Using fundus photographs, retinal microvascular morphometry offers the prospect of meaningful improvements in risk stratification in cardiovascular disease.61 Table 4 summarises major longitudinal cohort studies (n<10 000) on an eye and systemic diseases that were performed among the Western populations62–68 and Asian populations.69–75 Early signs of elevated risk of major systemic diseases, such as diabetes mellitus,76 stroke,77–79 hypertension80 and cardiovascular diseases,81 can be detected in the retinal blood vessels. The advent of powerful computer-based algorithms offers the prospect of truly ground-breaking advances in medical care.37 A recent study demonstrated that the application of deep learning to retinal fundus images can be used to predict cardiovascular risk factors such as age, gender and smoking status.37
Characteristics of prospective cohort studies on eye diseases (n≤10 000)
Neurodegenerative diseases including Parkinson’s disease (PD), Alzheimer’s disease (AD) and multiple sclerosis (MS) all have a measurable effect on the retina. Recent studies using OCT showed differences in inner retinal layers between the normal population and participants with PD,82 AD83 and MS.84 Studies have shown reduction in the ganglion cell layer along with the inner plexiform layer in patients with AD compared with healthy controls,85–87 while others reported thinning in the RNFL, especially in the superior and inferior quadrants.83 88–90 With a large cohort and detailed measurements at multiple time points, the UK Biobank is able to assess if changes in the eye precede development of these conditions or are a consequence from the neurodegenerative conditions.
Comparison with other cohorts, biobanks and consortia
Table 5 describes large prospective cohorts (>10 000) that examine associations with eye diseases. European studies include the Rotterdam Study of 14 926 participants aged 45 years or older91 and the Gutenberg Health Study of 14 700 participants aged 35–74 years.92 In Asia, the Kangbuk Samsung Health Study performed health screening on 281 238 employees aged 20 years and older. However, there are limited ocular measurements with the KSH study.93 94 Large prospective studies are well suited for investigating the risk factors for diseases and could either be conducted as a biobank such as the UK Biobank,22 China Kadoorie Biobank95 and The American Cancer Society’s Cancer Prevention Study 396 or a consortium such as the P3G consortium,97 National Cancer Institute Cohort Consortium,98 Cohorts for Heart and Aging Research in Genomic Epidemiology99 and European Eye Epidemiology (E3) consortium. However, eye measures are not available on most of these large prospective studies except the UK Biobank and E3 consortium. The major differences between the biobank design and consortia are that the latter are often developed by pooling data from different studies with disparate consent/governance procedures that may limit the power to address previously unanticipated research questions.100 Moreover, there is more variability in sampling, measurements of exposures and identification of diseases ascertained.101 102 In contrast, biobanks are usually planned in advance with uniformity in collection of samples and genotyping has been carried out according to a predetermined strategy. Thus, consortia are typically regarded as less robust because of problems with direct and imputed genotyping, and non-standardised diagnostic criteria.
Characteristics of prospective cohort studies on eye diseases (n≥10 000)
Strengths and limitations
UK Biobank is the only prospective study with a very large sample size (>100 000) of participants with a range of eye measures. With the projected number of new cases diagnosed with a range of eye diseases, it will allow researchers to investigate the genetic, environmental and lifestyle risk factors of various eye diseases. In addition, there are intensive methods to ascertain outcomes with electronic and semiautomated sources for validation and sub classification.20
Despite the scope of eye data collected in the UK Biobank, limitations exist within the study. One important limitation of UK Biobank was its low response rate (5.5%), and that participants were more likely to be from a healthier, more affluent sector of the UK population. However, it is unlikely that the direction of the association is opposite in respondents and non-respondents, and hence representativeness is not a major concern. The UK Biobank was not set up to be representative of the general UK population. More importantly, the large sample size and extensive exposures allow for valid scientific inferences of associations between exposures and health outcomes that are generalisable to the wider population. In addition, a large number of cases allow the detection and quantification of small effect sizes. Eye measurements were performed in 6 out of 22 of the assessment centres and participants with eye measures tend to have an education level of degree and above compared with the whole UK Biobank cohort. Hence, they may come from a more affluent sector and may not represent the whole UK Biobank cohort. The first repeat eye measure was only performed in approximately 20 000 participants. However, a repeat of the baseline visit will be conducted every few years in subsets of 20–25 000 participants. The self-reported nature of eye diseases may result in recall bias and misclassification error. However, the biases should be minimal as the ascertainment of outcomes will be conducted through linkages to national healthcare database, relevant administrative databases and analysis of available phenotypic data. We have access to medical records.32
Collaboration
UK Biobank aims to provide open access data for health-related research and the data are made available to all bona fide researchers from the academic, charity, public and commercial sectors, both in the UK and internationally, without preferential or exclusive access for any user.20 All interested researchers may apply to access the data via an online application. Strict guidelines are in place to help ensure anonymity and confidentiality of participants’ data and samples.103
Conclusion
UK Biobank Eye and Vision data would allow investigation of the factors leading to the onset and disease progression of major eye diseases. In addition, the ocular phenotypes could be explored with systemic diseases such as diabetes, hypertension and neurological diseases. In conclusion, the extensive exposures and health outcomes available in the UK Biobank will provide scientists with insights into the predictors of ocular and systemic diseases, allowing customised treatment therapies and interventions tailored to the individual patient. Furthermore, its collaborative and multidisciplinary research allows scientists to use known or innovative methods to explore and further develop techniques and treatment strategies that could have a major impact on the field of biomedical, behavioural or clinical research.
Acknowledgments
We would like to acknowledge Tim Sprosen, Alan Young, Sir Rory Collins (all Oxford University Clinical Trials Service Unit and Epidemiological Studies Unit) and all those who had contributed to design and development of the UK Biobank eye data resource.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
Footnotes
Contributors SYLC had full access to all the data in the study and took responsibility for the integrity of the data and accuracy of the data analysis. Concept and design: NA, AL, CS, PTK and PJF. Acquisition, analysis or interpretation of data: SYLC, DT, NA, AL, PD, PP, ZM, CS, TP, PTK and PJF. Critical revision of the manuscript for important intellectual content: all authors. Obtained funding: CS, PP, PTK, PJF and UK Biobank Eye and Vision Consortium. All authors read and critically revised the manuscript. All authors approved the final manuscript.
Funding The UK Biobank Eye and Vision Consortium is supported by grants from Moorfields Eye Charity, The NIHR Biomedical Research Centre at Moorfields Eye Hospital NHS Foundation Trust (BRC2_009) and UCL Institute of Ophthalmology and the Alcon Research Institute.
Disclaimer No funders had a direct role in the collection, management, analysis or interpretation of the data; preparation, review or approval of the manuscript; nor in the decision to submit the manuscript for publication.
Competing interests This analysis was supported by the Eranda Foundation via the International Glaucoma Association in the design and conduct of the study. The UCL ORS and GRS programmes provided scholarship support for ZM, PTK, PJF, and PP and SYLC received salary support from the NIHR BRC at Moorfields Eye Hospital. PJF received support from the Richard Desmond Charitable Trust, via Fight for Sight, London. PJF reports personal fees from Allergan, Carl Zeiss, Google/DeepMind and Santen, a grant from Alcon, outside the submitted work.
Patient consent Obtained.
Ethics approval The North West Multi-center Research Ethics Committee approved the study (reference no., 06/MRE08/65), in accordance with the tenets of the Declaration of Helsinki. Detailed information about the study is available at the UK Biobank web site (https://www.ukbiobank.ac.uk/).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement This research used data from the UK Biobank Resource, under data access request number 2112.
Collaborators UK Biobank Eye & Vision Consortium: The UK Biobank Eye & Vision Consortium members are Tariq Aslam, PhD, Manchester University, Sarah A. Barman, PhD, Kingston University, Jenny H. Barrett, PhD, University of Leeds, Paul Bishop, PhD, Manchester University, Peter Blows, BSc, NIHR Biomedical Research Centre, Catey Bunce, DSc, King’s College London, Roxana O. Carare, PhD, University of Southampton, Usha Chakravarthy, FRCOphth, Queens University Belfast, Michelle Chan, FRCOphth, NIHR Biomedical Research Centre, Sharon Y.L. Chua, PhD, NIHR Biomedical Research Centre, David P. Crabb, PhD, UCL, Philippa M. Cumberland, MSc, UCL Great Ormond Street Institute of Child Health, Alexander Day,PhD, NIHR Biomedical Research Centre, Parul Desai, PhD, NIHRBiomedical Research Centre, Bal Dhillon, FRCOphth, University ofEdinburgh, Andrew D. Dick, FRCOphth, University of Bristol, Cathy Egan, FRCOphth, NIHR Biomedical Research Centre, Sarah Ennis, PhD,University of Southampton, Paul Foster, PhD, NIHR Biomedical ResearchCentre, Marcus Fruttiger, PhD, NIHR Biomedical Research Centre, John E.J. Gallacher, PhD, University of Oxford, David F. GARWAY-HEATH MD FRCOphth - NIHR Biomedical Research Centre, Jane Gibson, PhD, University of Southampton, Dan Gore, FRCOphth, NIHR Biomedical Research Centre, Jeremy A. Guggenheim, PhD, Cardiff University, Chris J. Hammond, FRCOphth, King’s College London, Alison Hardcastle, PhD,NIHR Biomedical Research Centre, Simon P. Harding, MD, University of Liverpool, Ruth E. Hogg, PhD, Queens University Belfast, Pirro Hysi, PhD, King’s College London, Pearse A. Keane, MD, NIHR, Biomedical Research Centre, Sir Peng T. Khaw, PhD, NIHR Biomedical Research Centre, Anthony P. Khawaja, DPhil, NIHR Biomedical Research Centre, Gerassimos Lascaratos, PhD, NIHR Biomedical Research Centre, AndrewJ. Lotery, MD, University of Southampton, TomMacGillivray, PhD,University of Edinburgh, Sarah Mackie, PhD, University of Leeds, Keith Martin, FRCOphth, University of Cambridge, Michelle McGaughey,Queen’s University Belfast, Bernadette McGuinness, PhD, Queen’sUniversity Belfast, Gareth J. McKay, PhD, Queen’s University Belfast, Martin McKibbin, FRCOphth, Leeds Teaching Hospitals NHS Trust, Danny Mitry, PhD, NIHR Biomedical Research Centre, Tony Moore, FRCOphth, NIHR Biomedical Research Centre, James E. Morgan, DPhil, Cardiff University, Zaynah A. Muthy, BSc, NIHR Biomedical Research Centre, Eoin O’Sullivan, MD, King’s College Hospital NHS Foundation Trust,Chris G. Owen, PhD, University of London, Praveen Patel, FRCOphth, NIHR Biomedical Research Centre, Euan Paterson, BSc, Queens University Belfast, Tunde Peto, PhD, Queen’s University Belfast, Axel Petzold, PhD, UCL, Jugnoo S. Rahi, PhD, UCL Great Ormond Street Institute of Child Health, Alicja R. Rudnikca, PhD, University ofLondon, Jay Self, PhD, University of Southampton, Sobha Sivaprasad, FRCOphth, NIHR Biomedical Research Centre, David Steel, FRCOphth, Newcastle University, Irene Stratton, MSc, Gloucestershire Hospitals NHS Foundation Trust, Nicholas Strouthidis, PhD, NIHR Biomedical Research Centre, Cathie Sudlow, DPhil, University of Edinburgh, Dhanes Thomas, FRCOphth, NIHR Biomedical Research Centre, Emanuele Trucco, PhD, University of Dundee, Adnan Tufail, FRCOphth, NIHR Biomedical Research Centre, Veronique Vitart, PhD, University of Edinburgh, Stephen A. Vernon, DM, Nottingham University Hospitals NHSTrust, Ananth C. Viswanathan, FRCOphth, NIHR Biomedical Research Centre, Cathy Williams, PhD, University of Bristol, Katie Williams, PhD, King’s College London, Jayne V. Woodside, MRCOphth, PhD, Queen’s University Belfast, Max M. Yates, PhD, University of East Anglia, Jennifer Yip, PhD, University of Cambridge, and Yalin Zheng, PhD, University of Liverpool.