Article Text

Abstract
Introduction The frequency of screening for HIV and other sexually transmitted infections (STIs) among men who have sex with men (MSM) is still low in China.
Methods and analysis A sexual health clinic based randomised controlled trial will be conducted in Guangzhou, Wuxi and Shenzhen, China, enrolling 600 MSM. Eligibility will be judged by the pre-programed iPad based questionnaire: (1) age ≥18 years and (2) have had two or more male anal sex partners, or condomless anal sex with a casual male sex partner, or an STI history, in the past 6 months, and (3) provides a valid mobile phone number. Eligible men will be randomly allocated 1:1 to the intervention arm (with monthly text messages reminding them to test for HIV/STIs) or to the control arm (with no reminders). Men in both arms will complete a questionnaire onsite at enrolment and after 12 months, and another questionnaire online at 6 months. Men in both arms will be tested for HIV, syphilis, anal gonorrhoea/chlamydia and penile gonorrhoea/chlamydia at enrolment and at 12 months. The primary outcome is the rate and frequency of HIV testing within the 12 months after enrolment. The secondary outcome is the rate of unprotected anal intercourse. An assessment of the cost effectiveness of this intervention is also planned.
Ethics and dissemination The study has been approved by the ethical review committees of the University of New South Wales, Australia (HC16803), the Guangdong Provincial Centre for Skin Disease and STI Control (GDDHLS-20160926) and the Wuxi Centre for Disease Control and Prevention (WXCDC2016009), China. Study findings will be submitted to academic journals and disseminated to local health authorities.
Trial registration number Chinese Clinical Trial Registry at: http://www.chictr.org.cn/showprojen.aspx?proj=15752 and WHO International Clinical Trials Registry Platform at: http://apps.who.int/trialsearch/Trial2.aspx?TrialID=ChiCTR-IOR-16009304.
- Text message service
- Reminder
- HIV
- STI
- Men who have sex with men
- Sexual health clinic
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
No study has examined the role of sexual health clinic based automated short messaging services in the testing and detection of HIV/sexually transmitted infections (STIs) in men who have sex with men (MSM) in China.
Findings from this study have the potential to help health authorities to develop new interventional strategies to control HIV/STIs among MSM in China.
This intervention, from judging eligibility to sending text message reminders, is wholly automated and requires limited human input, which can be easily replicated in other sexual health clinics in China and beyond.
Sexual behaviours and STI history during follow-up will be self-reported by participants, which may be subject to bias.
Loss to follow-up of participants is possible in this longitudinal study.
Introduction
In many countries, men who have sex with men (MSM) are disproportionately affected by HIV and other sexually transmissible infections (STIs), such as gonorrhoea, chlamydia and syphilis.1–4 More frequent screening for HIV and other STIs has the potential to improve detection of these largely asymptomatic infections, interrupting transmission and improving disease control.5 Guidelines in a number of countries call for regular screening for HIV/STIs among MSM. For example, US and Australian guidelines recommend that all MSM be screened for urethral and rectal chlamydia, pharyngeal and rectal gonorrhoea, syphilis and HIV at least once a year, with 3–6 monthly screening of MSM at higher risk for HIV/STI transmission.6 7 However, available data suggest that the rate of screening for these infections among MSM is much lower than recommended in many countries.8 9
Significant increases in screening rates for gonorrhoea and chlamydia (OR 1.4–1.9) have been demonstrated in observational studies using several different strategies: use of a computer alert on an electronic medical record,10 introduction of clinic guidelines on STI screening11 and short text messaging reminders for repeat STI screening.12 13 Increases in syphilis testing (OR 2.3–21.4) were found using the following strategies: advocating regular serological screening for syphilis during routine HIV care14; including syphilis serology testing routinely with blood tests performed as part of HIV monitoring15; use of a computer alert on an electronic medical record16; and an electronic medical record system with a reminder to clinicians to enhance syphilis re-testing following syphilis treatment.17 A before and after study in Australia using existing clinical and behavioural data of clients attending a major sexual health clinic (SHC) found that an automated, computer generated text message service (SMS), providing 3 monthly reminders, doubled the testing rate for HIV, syphilis, gonorrhoea and chlamydia among MSM.18 The study also demonstrated an increased detection rate for syphilis, gonorrhoea and chlamydia, but not for HIV.18 Another before and after study in Australia found increased HIV/STI re-testing rates among MSM as a result of 3–6 monthly SMS reminders at a large SHC.12 However, until now, there has been no randomised controlled trial to confirm these effects.
MSM in China are increasingly engaging in high risk sexual behaviours, such as low rate of condom use in anal sex, multiple concurrent partnerships and drug use during sex.19 The rates of HIV and STIs among this population are high and increasing. The estimated HIV prevalence among MSM in China has increased sharply over the past decade, from 0.6% in 2003 to 8% in 2015.20 21 Accordingly, the proportion of MSM among all people living with HIV/AIDS has also increased steadily, from 7% in 2005 to 25% in 2015.22 23 Many MSM in China were also infected with other STIs. A meta-analysis found that the prevalence levels of STIs among MSM in China were 6% for chlamydia, 2% for genital warts, 2% for gonorrhoea, 9% for hepatitis B, 1% for hepatitis C, 66% for human papillomavirus and 11% for herpes simplex virus 2.24 However, the testing rate for these infections was suboptimal. A systematic review found that >40% of MSM in China had tested for HIV in the past year.25 Nearly half of MSM in China had a baseline CD4+ cell count of ≤350/mm3 at HIV diagnosis.26 The rates of testing for other STIs were also low.27 28 Introduction of an effective intervention that can increase testing and help achieve timely diagnosis of HIV and other STIs among MSM is urgently needed in China.
Our study aims to use a randomised controlled trial to evaluate the role of SHC based automated text message services in the testing and detection of HIV and other STIs among MSM in China.
Methods and analysis
Overview
The proposed protocol (dated 8 December 2016) was developed and facilitated by collaborations between experienced investigators from the Kirby Institute, University of New South Wales (UNSW), Sydney, Australia, Dermatology Hospital of Southern Medical University (DHSMU), Guangzhou, China, Wuxi Centre for Disease Control and Prevention (CDC), Wuxi, China, Nanshan District Centre for Chronic Disease Control and Prevention (CCDC), Shenzhen, China and Sun Yat-sen University, Guangzhou, China. The study will randomise 600 MSM, 1:1, into an intervention group (with text reminders) and a control group (no reminders), and evaluate the role of the SHC based automated text message services in the testing and detection of HIV/STIs among MSM. A sample size of 300 MSM in each group will provide 90% power to detect a 15.0% (from 50% to 65%) difference in the proportion of HIV testing in the past 12 months between the two groups, taking into account 30% lost to follow-up at 12 months.
Objectives
The primary objective of this study is to determine the impact of SHC based automated text message services on the testing and detection of HIV. The secondary objective is to determine the impact of SHC based automated text message services on changes in sexual behaviours. The additional analysis is to evaluate the costs and incremental cost effectiveness of the intervention.
Study settings
This study will be based at the SHCs affiliated to DHSMU, Wuxi CDC and Shenzhen Nanshan CDC. The populations in Guangzhou, Wuxi and Shenzhen were approximately 13, 6 and 13 million, respectively, with per capita gross domestic product (GDP) of over USD20 000 in 2014.29–31 The three SHCs provide HIV/syphilis voluntary counselling and testing and HIV/STI treatment services to over 25 000 clients annually, 10% of whom are estimated to be MSM (data not published). These three SHCs are equipped with microbiological diagnostic units and capable of timely testing and treating HIV and other STIs, including syphilis, gonorrhoea, chlamydia trachomatis and genital warts.
Inclusion criteria
MSM attending the three clinics will be invited to join the study if they meet the following criteria: (1) anatomical men aged 18 years or older; (2) having more than two male anal sex partners, or condomless anal sex with a casual male sex partner, or an STI history including gonorrhoea, syphilis, anogenital warts, genital herpes and chlamydia trachomatis, in the past 6 months; (3) possessing a mobile phone; (4) willing to provide informed consent for the collection of demographic data, sexual behavioural data and HIV/STI testing and biological samples to test for HIV/STIs; (5) residing in a study city in the next 12 months or visiting a study city frequently enough to participate in the study; and (6) willing to register testing results if they test elsewhere during the study.
Exclusion criteria
MSM who meet one or more of the following criteria will be excluded: (1) severe psychiatric illnesses; (2) unable to read or use the iPad questionnaire; and (3) does not speak or read the Chinese languages.
Study procedures
We will use the following strategies for achieving adequate participant enrolment to reach the target sample size: (1) at the three clinics, study posters will be put in the waiting area, consultation rooms and male toilets; (2) the clinics will work with local MSM community organisations to refer potentially eligible MSM, who will physically attend the three clinics to complete the enrolment; and (3) doctors will encourage participants to introduce our study to their peers. A study phone number will be designated to this study.
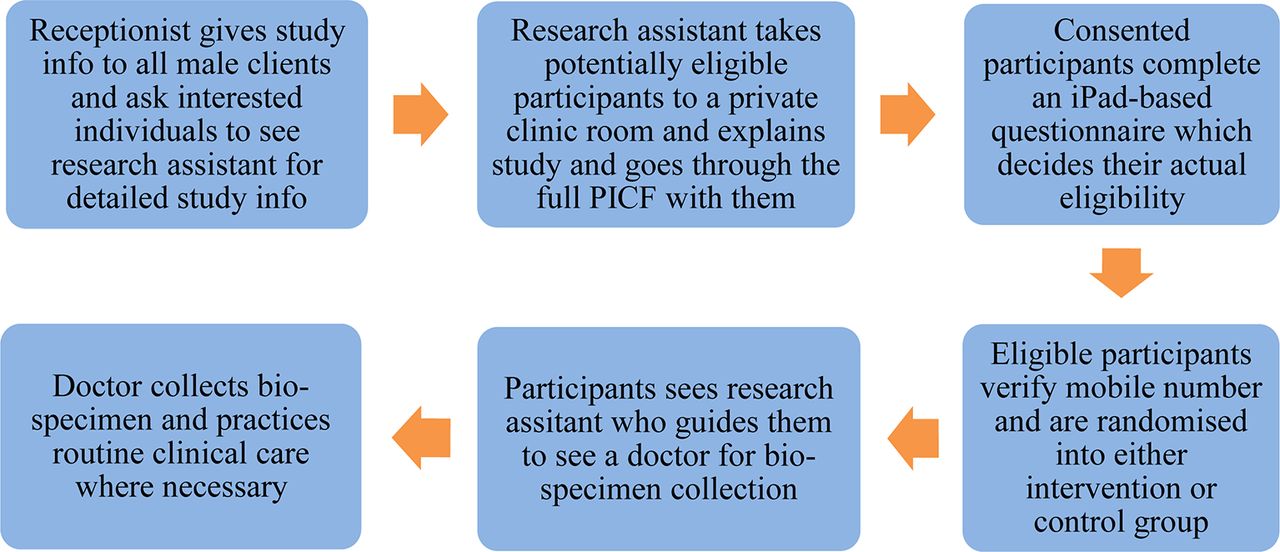
This randomised controlled trial will consist of computer assisted self-interview (CASI) and automated, computer generated SMS reminders to 600 MSM attending the SHCs. It will be conducted over 21–24 months: 3 months of logistic preparation, 3–6 months of recruitment, 12 months of follow-up and 3 months of report preparation. The detailed recruitment procedure is described in figure 1 and table 1.
Over the 3–6 month recruiting period, all male clients presenting to the clinic will be given an information flyer by a receptionist not directly involved in the study. The flyer will include basic information about the study, including that it is a study for MSM. The receptionist will ask each male client to read the flyer and visit the study research assistant who will sit at a nearby desk, if they are interested in finding out more about the study. Clients may be enrolled and passed on to the research assistant when they are seen by a clinician after leaving the waiting area. Those male clients who express interest in participating will see the study research assistant, who will take them to a private clinic room where an iPad questionnaire system is installed. The study research assistant will explain what the study involves and go through the iPad based full participant information and consent form (PICF) with potential eligible participants. Men will have time to read the PICF, to ask questions and to decide if they will participate in the study. Men will need to click the ‘agree’ button to consent before completing an iPad based questionnaire. The study research assistant will ask consented participants to complete the iPad based questionnaire on their own, in the private room. They will be instructed that if they have any further questions, they should ask the research assistant who will be at a desk, outside of the private room.
The questionnaire will collect information on sexual behaviours, HIV/STI testing behaviours and diagnosis history, and alcohol/tobacco/drug use. The pre-programmed logic in the questionnaire will judge if a participant is actually eligible, based on the sexual behaviour variables. Those who are not eligible will be thanked and released back into the clinic waiting room for their routine clinical care. Eligible participants will provide a valid mobile phone number and then be automatically randomised into the intervention or control group by the computer. They will then receive a text message with a code as their study ID. When they finish the PICF and questionnaire, participants will see the study research assistant who will guide them to see a doctor for bio-specimen collection, followed by routine clinical care, if necessary. Eligible MSM who opt out of the study will be recorded and asked about their reasons for declining.
During the whole study period, clients, clinicians, research assistants and data analysts will be blinded after assignment to the intervention. To maintain the overall quality and legitimacy of the trial, unblinding should occur only in exceptional circumstances when knowledge of the intervention can substantially increase the HIV/STI retesting rate among MSM. We will judge this on the basis of the interim data analysis. If unblinding is deemed to be necessary, the steering committee of the study will discuss and make a decision in consultation with the ethics committees.

Flowchart of recruitment details. PICF, participant information and consent form.
Schematic diagram of the study procedure
The detailed study procedure is described in figure 2. We acknowledge that direct mentioning of sensitive words, such as HIV and STIs, in SMS reminders may lead to privacy issues for participants. As a result, we will avoid using these sensitive words in actual SMS reminders. Instead, in actual reminders, we will use ‘Little A’ to refer to ‘HIV’, ‘Little B’ to refer to ‘STIs’, ‘Health check’ to refer to ‘HIV/STI testing’, ‘Self health check’ to refer to ‘HIV self-testing at home’ and ‘health kit’ to refer to ‘condoms/lubes/MSM health manuals’. We will clarify this in the PICF. All messages will include a withdrawal option.

{kind=link}
{kind=link}
Flowchart of the study procedure. STI, sexually transmitted infection.
For MSM in the intervention group, on enrolment, they will receive message A: "A gentle reminder: if you plan to have a health check again in the next 12 months, welcome to our centre. If you do it elsewhere (including self-health check) in the next 12 months, please register the results online at the following link: ******. Every time you register we will compensate you with an electronic mobile phone credit of CNY10 (USD1.5). If you change your mobile phone number in the next 12 months please let us know". When they register online, participants need to enter the mobile phone number that was validated at enrolment and the initial of their surname to enter the questionnaire. This is designed to avoid the exposure of sensitive questions to a non-participant. On the second day after enrolment, they will receive message B: "A gentle reminder: Little A and little B are spreading rapidly and it’s hard to detect by yourself. Your best protection is a regular check-up (eg, every 3 months). If you change your mobile phone number please let us know". Starting from day 30, they will receive message C every 30 days: "A gentle reminder: if you have not had a health check in the past 3 months please do so as soon as possible. If you change your mobile phone number please let us know". On day 190, 10 days after they receive message C on day 180, they will receive message D, reminding them to complete an online survey about their sexual life and testing behaviours in the past 6 months: "A gentle reminder: please complete a survey at the following link at your earliest convenience: ******. We will compensate you with an electronic mobile phone credit of CNY50 (USD8). If you change your mobile phone number please let us know". On day 370, 10 days after they receive message C on day 360, they will receive message E, reminding them to complete an onsite survey about their sexual life and testing behaviours in the past 6 months: "A gentle reminder: please attend our centre to complete the final survey. We will compensate you with an electronic mobile phone credit of CNY100 (USD16), together with a health kit. If you change your mobile phone number please let us know". At enrolment and at 12 months, men will be tested for HIV, syphilis, urethral and anal chlamydia, and gonorrhoea, and examined for anogenital warts. CD4+ testing will be provided for men diagnosed with HIV. HIV/STIs will be treated as per the relevant treatment guidelines in China. At 6 and 12 months, men will also be asked questions about their experience of the intervention, including the impact of the intervention on their everyday life, mental health, sexual health and general health (figure 2).
MSM in the control group will receive message A on enrolment, message D on day 190 and message E on 370. They will not receive messages B and C. They will complete the same questionnaire as men in the intervention group at enrolment, and at 6 months and 12 months, and will be tested for the above mentioned HIV/STIs at enrolment and at 12 months. They will not be asked about their experience of the intervention.
The 10 days’ time gap between messages C and D is planned to give men in both groups enough time to attend a SHC on receiving message C. Apart from a mobile phone number (compulsory), we will also try to collect other contact information (optional), including email, QQ and WeChat ID (instant online messaging applications frequently used in China). At 6 and 12 months, men will be contacted via the additional contact information if they do not complete a designated survey within 7 days after messages D and E are sent. Men who register testing information online or fill in an online questionnaire at 6 months will need to enter their mobile number to access the actual questionnaire. This is designed in case another person oversees the URL address from message A. The process from commencing CASI to the regular dispatch of the reminders will be entirely automated, requiring no human input.
For men in both groups, at enrolment and at 12 months, a study nurse will collect a swab from the anal canal to test for anal gonorrhoea and chlamydia, and 5 mL of blood to test for HIV and syphilis. Participants will self-collect a urine sample to test for urethral gonorrhoea and chlamydia. A doctor will check for anogenital warts for each participant. The HIV serological status will be screened by ARCHITECT HIV Ag/Ab Combo assay (Abbott Laboratories, Abbott Park, Illinois, USA). Positive samples will be further screened by enzyme linked immunosorbent assay (ELISA) (Bio-Rad Laboratories, California, USA). Samples positive for ELISA will be confirmed by the HIV-1/2 western blot assay (HIV Blot 2.2 WB; Genelabs Diagnostics, Singapore). Confirmed HIV cases will be tested for CD4+ T cell count. Syphilis will be screened by the toluidine red unheated serum test (TRUST) (RSbio, Shanghai, China), and samples positive for TRUST will be confirmed by treponema pallidum particle assay (TPPA) (Fuji ReBio, Tokyo, Japan). Anal and urethral gonorrhoea and chlamydia will be tested using PCR (Roche Diagnostics, Shanghai, China). Anogential warts will be checked by a doctor with the assistance of the acetic acid test.
Incentives and retention
Study participants will receive health education materials, condoms and lubricant on completion of the CASI questionnaire at enrolment and at 12 months. Participants will receive an electronic mobile phone credit of CNY50 (USD8), CNY50 (USD8) and CNY100 (USD16) on completion of the surveys at enrolment, at 6 months and at 12 months. Participants who test elsewhere will receive an additional electronic mobile phone credit of CNY10 (USD 1.5) each time they register testing results online.
Statistical methods
Power/sample size
We used the following formula to calculate sample size:

In this formula, Zα and Zβ represent the Z boundaries under the standard normal distribution; p1 and p0 represent the proportion of a parameter in the intervention and control groups, respectively; p is equal to the average of p1 and p0; q=1 p. We used two parameters in the calculation of sample size: (a) proportion of men who have HIV testing during the 12 months after baseline; (b) proportion of men who have condomless anal sex during the 12 months after baseline. We assumed a two sided hypothesis test with a 5% significance level (Zα/2=1.96), a desired power of 90% (Zβ=1.28) and that both groups will have the same number of observations.
Using parameter (a), the rate of HIV testing in the past 12 months among MSM in Wuxi in 2014 was 50% (p0), and this figure was expected to increase to 65% (p1) according to a before and after study in Australia.18 This resulted in a sample size of 225 in each group. Khosropour et al retained approximately 70% of MSM for 12 months using bimonthly follow-up surveys through text messages.30 We will adopt a number of strategies to minimise the lost to follow-up rate: educating investigators about the culture in the MSM community and developing a rapport with participants; verifying mobile phone numbers at enrolment; contacting participants on days 190 and 370 using various messaging softwares/apps such as WeChat, QQ, email, etc; and reasonable incentives. Considering a lost to follow-up rate of 30%, a sample size of 300 MSM in each group will be needed.
Analysis plan
Analyses will be performed using STATA 13.0 (College Station, Texas, USA) statistical analysis software. All effects will be estimated with 95% CI and p values from the corresponding hypothesis tests. Statistical significance will be taken as two sided p values <0.05, with no adjustment for multiple comparisons. Characteristics of groups will be summarised at baseline and across study arms. Mean duration of study follow-up will be compared by group.
The primary analysis will compare randomised groups of MSM using an intention to treat approach. Initial analyses will be simple, unadjusted comparisons of randomised groups. If there appears to be any important imbalances between the randomised groups in terms of baseline covariates, adjusted analyses will also be performed.
The primary outcome is the proportion of HIV/STI testing and detection during the past 12 months, comparing the intervention and control arms. At the end of the study we will use Cox proportional hazard models with Kaplan–Meier plots and the log rank test to explore the cumulative rate of reported HIV/STI testing and detection during the previous 12 months, comparing the two groups. Numbers of testing and detection of each infection will also be compared. We will also use the χ2 test to compare the proportion of reported HIV/STI testing and detection during the previous 12 months before intervention with that during the 12 months after intervention, within the intervention group. Numbers of testing and detection of each infection will also be compared.
The second outcome is the proportion of condomless anal sex during the past 12 months. At the end of the study we will use the χ2 test to compare the proportion of reported condomless anal sex during the previous 12 months between the two groups. We will also use the Rank sum test to compare the number of reported anal sex partners during the previous 12 months between the two groups. We will use the χ2 test to compare the proportion of reported condomless anal sex during the previous 12 months before the intervention with that during the 12 months after the intervention, within the intervention group. We will use the Rank sum test to compare the number of reported anal sex partners during the previous 12 months before the intervention with that during the 12 months after the intervention, within the intervention group.
Additional analyses
Cost and cost effectiveness evaluation
Although some studies have assessed the cost effectiveness of HIV testing methods among high risk populations in some regions,32–38 whether the intervention in this study is cost effective is unclear. As a result, the costs and incremental cost effectiveness of the intervention compared with the control will be evaluated, using standard methods of cost effectiveness analysis.39 Our analysis will include the costs of the self-registration and SMS reminding system development and maintenance, HIV/STI testing and counselling, follow-up and treatment. All costs will be measured from a societal perspective, and inflated to 2015 Chinese Yuan at a discounting rate of 3% annually.
Cost effectiveness analysis
Based on incremental cost effectiveness analysis, we will calculate the incremental cost for one additional newly identified HIV/STI case, and one additional early HIV case, using the following formula39:

Markov model based cost utility analysis
We will develop a decision model to reflect when successful HIV/STI detection, follow-up and treatment occur for a cohort of MSM with/without the intervention, and then a Markov model estimating the lifecycle of MSM from entering the cohort until death, to examine the incremental cost utility of the intervention. Effectiveness is measured as quality adjusted life years (QALYs) gained. We assume that QALYs accrue by early initiation of antiretroviral therapy (ART) following early HIV detection. According to the actual situation in China, the natural history of HIV/AIDS is categorised as the following stages: asymptomatic HIV, symptomatic HIV, AIDS and death Health states summarise current status based on CD4+ T cell count, quality of life, ART usage and resource use. ART and CD4+ T cell count combined determine the transition probabilities and mortality rates.40 41 The model will assess HIV status, stage transfer and its consequences among MSM with incident HIV infection on an annual basis. All parameters used in this model will be compiled from a variety of sources, including literature review, ongoing cohort studies and investigations, surveillance data or unpublished data from Wuxi and other parts of China.
In this study, we assume that: (1) stage transition in the Markov model happens once a year and (2) once an HIV infected man receives ART, he will complete the entire treatment procedure. To account for assumptions and uncertainties of this model, we will perform one way sensitivity analyses on all model parameters. For all the probability variables, our ranges for sensitivity analyses represent our judgement of the variation on the basis of both the literature and discussion with experts.
Sample/data storage
All electronic questionnaires and consent forms will be stored in a password protected computer at the information centre at DHSMU, as per our usual practice. The data will be stored in a format that is identifiable. This is designed to match data with individual participants in follow-up visits in this study. However, only the custodian will have access to the original data. All identifying variables, including name (a pseudonym is acceptable), initial of participant’s surname, mobile phone number and date of birth will be de-identified before the data are transferred to a data analyst in this study. The custodian will ensure that the data are stored and managed appropriately and according to the relevant privacy laws. The data custodian will only share data with researchers who are conducting HIV/STI testing related epidemiological studies and only when these projects have received separate ethics approval from a human research ethics committee. All identifying variables, including name (a pseudonym is acceptable), initial of participant’s surname, mobile phone number and date of birth will be de-identified before data sharing. Bio-specimen collected at a given site will be stored at the corresponding participatory institution.
Ethics and dissemination
The study has been approved by the ethical review committees of the University of New South Wales, Australia (HC16803), the Dermatology Hospital of Southern Medical University (GDDHLS-20160926) and Wuxi Centre for Disease Control and Prevention (WXCDC2016009), China. We anticipate that the benefits of study participation will outweigh any risks, including loss of confidentiality and privacy of clinical information. Participants will benefit from frequent testing and early diagnosis of HIV/STIs and timely treatment if positive. The findings of the study will be disseminated to local and national governments in China as well as to the wider academic audience and public health organisations through peer reviewed publications and international conferences.
Discussion
This study protocol describes a randomised controlled trial designed to increase the testing and detection of HIV and other STIs among Chinese MSM through computer assisted self-interview and automated computer generated reminders. First, we seek to develop a platform requiring limited investment and human power that could be easily replicated and deployed in other SHCs in China and beyond. As such, one of the challenges in designing the intervention was the acceptance of it among target population MSM in China, a population that has long been marginalised and discriminated against. Fortunately, in our unpublished pre-trial study, almost 80% of MSM in the community were willing to take such an intervention. It is estimated that this rate would be even higher among MSM attending SHCs. Other key challenges to this study include the need to sustain the motivation of clinic staff to participate in the study while addressing the multiple competing health priorities. Second, we will be able to understand what characteristics of MS make them more likely to take this intervention as well as barriers that prevent other MSM from taking this intervention. This will help develop an intervention that is contextualised and tailored to the characteristics of MSM. Third, if successful, this intervention with high potential cost effectiveness will contribute to the compilation of the fabric of quality SHCs and health providers that will eventually be readily available to MSM at their finger tips. This will greatly encourage and facilitate them to test for HIV/STIs on a more frequent basis. Lastly, the results from this study may facilitate the development of proactive intervention strategies targeting other at-risk populations, such as female sex workers and their clients, and drug users, to increase the testing and detection of HIV and other STIs and hence prevent the transmission of these infections.
This intervention has its limitations. First, the 12 month research period is a long commitment for MSM, as many of them are quite mobile. The retention rate could be compromised by 12 months. To tackle this problem, we will verify participants’ mobile phone numbers at enrolment and remind them to update their mobile number every 30 days. Additionally, we will use other contact information reported by participants to achieve the highest possible retention rate. Second, men could forget to register testing from other venues. To tackle this problem, we will remind them to do this in message A at enrolment. Because a similar reminder during the study would potentially contaminate the intervention, we will not send further reminders. Third, as this intervention will be conducted in metropolitan cities, the results may not apply to other settings.
In summary, the knowledge gained from this study may be used to design similar protocols with a higher number of participants and appropriate intervention strategies to reduce the burden of HIV and other STIs among MSM, a population that is heavily burdened by these infections. Additionally, if the results are positive, we will scale up this practice in more SHCs across China.
Acknowledgments
We thank Dr Qianqian Xin, Capital Institute of Paediatric, Beijing, Dr Gang Zeng, Alere Inc Beijing and Dr Jinghua Li, Sun Yat-sen University, for their comments on the protocol.
References
Footnotes
Contributors HZ and XM initiated this research plan and designed this protocol, with BY and AG consulting on ethics and the feasibility of the research. ZL, TJ, XZ, YD and LY provided expertise on recruitment and sample collection and will supervise these aspects at the three study clinics. JH, SH and HZ provided expertise on sample testing and storage. WC helped with the design of the questionnaire and recruitment methods.
Funding This work was supported by a grant from the Australian National Health and Medical Research Commission (NHMRC) Early Career Fellowship (APP1092621), and research grants from Guangdong Provincial Centre for Skin Disease and STI Control (YCS201669), Wuxi Municipal Health and Family Planning Commission(MS201613), Wuxi Municipal Science and Technology Bureau (CSZ0N1512) and Nanshan District Centre for Chronic Disease Control and Prevention. The funding bodies other than NHMRC participated in study design, data collection and analysis, preparation of the manuscript and the decision to publish.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study has been approved by the ethical review committees of the University of New South Wales, Australia (HC16803), the Guangdong Provincial Centre for Skin Disease and STI Control (GDDHLS-20160926) and the Wuxi Centre for Disease Control and Prevention (WXCDC2016009), China.
Provenance and peer review Not commissioned; externally peer reviewed.