Article Text

Statistics from Altmetric.com
P13 HIGHLY SENSITIVE ASSAY TO DETECT HEPCIDIN IN BIOLOGICAL FLUIDS: PRESENCE OF HEPCIDIN IN PLEURAL FLUID
1A. Sangwaiya, 1J. D. Arnold, 1V. Manglam, 2M. Thursz, 1F. Geoghegan, 3M. Busbridge. 1Ealing Hospital NHS Trust, London, UK, 2St Mary’s Hospital NHS Trust, London, UK, 3Hammersmith Hospital NHS Trust, London, UK
Introduction: Hepcidin is a 25 aminoacid cysteine-rich peptide predominantly formed in the liver. It acts as a central iron regulator in humans but as an antimicrobial peptide in other species. It has been proposed that hepcidin causes anaemia of chronic inflammation by suppressing iron export via ferroportin channels in macrophages, enterocytes and kupffer cells. Due to its dual role, hepcidin is a novel peptide to study. We report the levels of hepcidin in pleural fluids due to various causes.
Patients and Methods: 11 participants with pleural effusion were recruited from a single hospital with mixed ethnicity, predominantly Caucasians and south Asians. Pleural fluid was obtained for routine investigations and divided into two cohorts using Light’s criteria as exudate or transudate. Serum was collected from 25 healthy volunteers. Hepcidin-25 was measured using a novel robust radioimmunoassay developed in-house at the clinical chemistry department at Hammersmith Hospital.
Results: The mean hepcidin in exudate (n = 8, M:F 5:3) was 80.87±103.55 ng/ml (median 40.47, SE 36.61). The mean total protein level exudate was 44.31 g/l. The mean hepcidin in transudate (n = 3, M:F 2:1) was 16.71±6.68 ng/ml (median 18.9, SE 3.85). The mean total protein in transudate was <25 g/l. The mean serum hepcidin in healthy volunteers (n = 25, M:F 11:14) was 15.30±15.71 ng/ml.
Conclusion: We provide evidence for the first time presence of hepcidin in pleural fluid. A higher trend of hepcidin in exudate pleural fluid has been observed which may be a part of innate immunity preserved over evolution. More studies are needed to confirm its role and biological activity in pleural fluid.
P14 PREVENTION OF SKIN METASTASIS IN MALIGNANT MESOTHELIOMA WITH PROPHYLACTIC IRRADIATION OF TRACTS (PIT): IS THE DIFFERENCE IN RESEARCH EVIDENCE DUE TO THE DISCREPANCY BETWEEN THE DISTANCE FROM PLEURAL ENTRY POINT AND THE SKIN SCAR?
1K. L. Hambleton, 2C. Faivre-Finn, 1D. R. Baldwin. 1Nottingham University Hospitals, Nottingham, UK, 2Christie Hospital, Manchester, UK
Background: Only three small randomised controlled trials have assessed the role of prophylactic irradiation of tracts (PIT) in malignant mesothelioma after chest intervention with conflicting results reported. Boutin et al showed tract seeding in 40% of controls compared with 0% in patients treated with PIT.1 However, O’Rourke et al and Bydder et al found no significant reduction in the incidence of tract metastases when using PIT.2 3 Between these studies there was variation in dose and fractionation of radiotherapy, time after procedure before PIT and size of radiation field. We hypothesise that the skin scar does not accurately reflect the entry point into the pleura. Hence radiotherapy aimed at the skin scar may be missing areas at risk of microscopic spread along the tracts that may explain variation in success of PIT. This study looks at the difference between skin and pleural entry points of chest drains using chest radiograph measurements.
Methods: Chest radiographs were used from patients who had had medical thoracoscopies at Nottingham University Hospital between May 2007 and May 2009. We measured skin to pleural entry point using PACS workstations. 40 chest radiographs from 40 patients were reviewed by two observers working independently. Each observer took measurements twice without reference to the first measurement. The mean results from both observers were compared using a paired t test. A mean of all four measurements was calculated and expressed graphically.
Results: The mean measurements for each observer were not different (p = 0.85, paired t test). The results for the vertical distance between skin entry point and pleural entry point are shown in fig 1. The proportion of measurements that were ⩾3 cm, ⩾4 cm and ⩾5 cm was 65%, 52.5% and 32.5%, respectively.

Vertical distance form pleural entry point to skin.
Conclusions: This study shows large discrepancies between the skin scar (used to centre radiotherapy fields) and the entry point into the pleura. As field size varied in studies of PIT, this could explain the differences in the findings of the previous studies. A randomised controlled trial evaluating the role of PIT and taking our findings into account is warranted.
P15 ASSESSING A PANEL OF FIVE BIOMARKERS IN THE SPUTUM OF PATIENTS WITH AND WITHOUT LUNG CANCER
1R. Ghosal, 1K. E. Lewis, 2P. J. Kloer, 3C. Davies, 1P. D. Lewis. 1School of Medicine, University of Swansea, Swansea, UK, 2Prince Philip Hospital, Llanelli, UK, 3Singleton Hospital, Swansea, UK
Introduction: Several gene and protein biomarkers have been detected within cells of lung cancer biopsy tissue. Screening strategies using sputum cytology (with and without radiology) to improve detection rates for early lung cancer (LC) have been disappointing. We assessed if five of these tissue biomarkers could reliably diagnose LC from bronchial cells found in the sputum in a small preliminary study.
Participants: 68 consecutive patients (44 men) undergoing bronchoscopy for suspected LC, mean age 65±11.2 years, with mean 38.4 smoking pack-years. We excluded those who refused consent (n = 4) and those unable to provide sputum (n = 12). 42 patients had a final diagnosis of lung cancer (9 had adenocarcinoma, 13 squamous cell carcinoma, 3 large cell, 8 NSCLC of unknown cell type, 6 small cell, 3 clinical diagnosis). 26 had no evidence of LC at 1-year follow-up.
Procedure: Sputum was self-expectorated prior to bronchoscopy and immediately stored at −80°C, centrifuged at 3000 rpm for 10 min, then placed in paraffin blocks. The samples were cut and stained with the antibodies p16, p53, p63, EGFR and cyclin D1. Two assessors counted the number of positive cells and intensity of staining for each patient. Nuclear staining was assessed for p16, p53, p63, cyclin D1 and cell membrane staining for EGFR.
Statistics: Wilcoxon rank sum test was used to assess the differences in the number of cells staining positive for each antibody between the LC and eventual non-cancer cohorts. Analysis was performed using the R statistical software.
Results: There was no statistical difference in the number of positive cells staining for individual antibodies for each biomarker in the sputa from LC and sputa from non-cancer groups (table 1).
Conclusion: These biomarkers did not show any differences between the sputum of lung cancer patients and those who eventually did not have lung cancer. The very low sensitivities for these biomarkers in particular means they are not very good for detecting LC in sputum as opposed to biopsy tissue. There appears little potential for this non-invasive approach to LC detection as many cancers would be missed.
P16 PET SCANNING INCREASES THE NEED FOR MEDIASTINAL STAGING PROCEDURES IN LUNG CANCER
C. M. Free, A. R. L. Medford, S. Agrawal, J. J. Entwisle, J. A. Bennett, A. Nakas. Glenfield Hospital, Leicester, UK
Background: The 2005 NICE guidelines on lung cancer state that candidates for radical treatment should have a positron emission tomography (PET) scan and that histological investigation should be performed to confirm N2/3 disease where PET is positive. Since 2002, PET and transbronchial needle aspiration (TBNA) have been introduced to our staging/diagnostic algorithms. We describe the impact of PET on our service.
Methods: Prospective data from the lung cancer multidisciplinary team meetings for 2002 and 2007 were cross-referenced with information supplied by the Cancer Registry for registrations of lung cancer during the same periods. Data on histology, stage and outcome were collected.
Results: In 2002, 409 lung cancers were diagnosed (62% men, median age 73 years, histological confirmation rate (HCR) 77.8%, small cell lung cancer (SCLC) 13.2%). In 2007 there were 482 cases (59% men, HCR 75.3%, SCLC 14.6%). In 2002, 12 PET scans were performed compared with 106 in 2007. In 2007, PET upstaged 20 patients and downstaged 18. 50 patients had surgery with a subsequent pathological stage. With respect to nodal status, PET correctly identified 19/31 (61%) who were N0, 4/8 (50%) with N1 disease and 9/11 (82%) with N2 (table 1). In terms of nodal involvement, PET falsely overstaged 14/50 patients (28%) and falsely understaged 4/50 (8%). In 2007, 25 patients had a TBNA (7 had subsequent mediastinoscopy). No TBNAs were performed in 2002. There was no significant difference in numbers of mediastinoscopies performed (17 in 2002 vs 22 in 2007). However, in 2007, 40 patients had sampling of the mediastinal lymph nodes (either by TBNA or mediastinoscopy) compared with only 17 patients in 2002 (p = 0.007). There was no significant difference in the distribution of stage (NSCLC and clinical diagnosis) (stage 1, 8% vs 9.7%; stage 2, 6.3% vs 4.9%; stage 3A, 9.1% vs 9.7%; stage 3B, 24.9% vs 20.1%; stage 4, 50.3% vs 49.5%).
Conclusion: The low specificity of PET-CT for mediastinal lymph node metastases has led to an increased need to invasively stage the mediastinum in our lung cancer population. Increasing the number of staging investigations has not led to a significant difference in the distribution of stage.
P17 ROLE OF BRONCHOSCOPY IN PERIPHERAL LUNG LESIONS
T. S. Jordan, H. Tan, M. Walshaw, E. Spencer, A. Collins, M. Ledson, A. Ashish, K. Mohan. Liverpool Heart and Chest Hospital, Liverpool, UK
Introduction: In its latest guidance, NICE recommends that patients with a suspicious peripheral lung lesion should undergo percutaneous lung biopsy as the investigation of choice. However, this route requires scarce radiological resources, has a higher incidence of complications (in particular, pneumothorax and haemorrhage) than bronchoscopy and is contraindicated in patients with poor spirometry or bullous emphysema. Furthermore, this guidance ignores the potential yield of targeted bronchial washings taken at bronchoscopy. To look at this, we audited our experience of diagnosing lung cancer using targeted bronchial washings in our large cancer unit (430 cases per year).
Method: We looked at 174 consecutive patients (mean age 73 years, 32 (18%) performance status (PS) >2, 25 (14%) forced expiratory volume in 1 s (FEV1) <35% or <1.0 litre, 52% male) with an ultimate diagnosis of lung cancer who presented with a peripheral lesion (mean diameter 3.8 cm, 155 (89%) solid) to our rapid access clinic over 1 year. No endobronchial lesion was seen at bronchoscopy but, guided by CT scan, targeted washings and brushings were taken for cytology.
Results: Cytology was diagnostic in 54 (31%): 36 (67%) squamous cell carcinoma, 19 (30%) adenocarcinoma and the remainder small cell carcinoma. Of these, 11 (20%) were PS >2 and 6 (11%) FEV1 <35% or <1.0 litre. Nine patients (17%) underwent lung resection where the original histology was confirmed. In the cytology negative group, 94 (78%) underwent another procedure or were referred for resection. The remaining 26 (22%) were clinical diagnoses due to poor PS (mean 2.1), poor lung function (10 (38%) FEV1 <35% or <1.0 litre) or co-morbidity. There was no correlation between cavitation and cytology result, but more peripheral lesions (regardless of tumour size) and adenocarcinoma were less likely to give positive cytology (p = 0.009).
Conclusions: The study highlights the role for bronchoscopy in the diagnosis of patients with peripheral lung lesions. A definitive diagnosis was made in one-third of cases, obviating the need for more invasive procedures. In particular, percutaenous lung biopsy, which has a much higher incidence of complications, is not recommended in patients with poor PS and is hazardous in those with poor lung function.
P18 PREVALENCE OF CEREBRAL RECURRENCE FOLLOWING RESECTION FOR NON-SMALL CELL LUNG CANCER IN THE POST-PET ERA: IS THERE A NEED FOR PREOPERATIVE CT BRAIN SCANNING AND IS IT COST EFFECTIVE?
L. M. Jones, L. Burke, S. R. A. West, P. K. Plant. St James’s University Hospital, Leeds, UK
Introduction: NICE recommended in 2005 that patients being considered for radical treatment should have a positron emission tomography (PET) scan which is more sensitive than thoracic CT scanning at detecting lung cancer. Due to background uptake of glucose by brain tissue, PET scanning is unreliable at detecting cerebral metastasis.1 Our study aimed to clarify the need for preoperative brain imaging.
Methods: Patient databases were retrospectively examined for patients with non-small cell lung cancer (NSCLC) who had undergone PET and thoracic surgery in the period from March 2007 to March 2008. We noted if they had had a preoperative head CT scan and also their preoperative and postoperative staging. Patients were followed up to 1 June 2009 to detect evidence of brain metastases.
Results: 47 patients (20 women, 27 men) were identified. Their mean age was 70.1 years (range 48–85). Six had had preoperative CT head imaging for neurological symptoms (all normal); 41 had no head imaging preoperatively. The mean follow-up from surgery to either death or the censure date was 476 days (2–802). 15 patients died, 6 in the postoperative stage, 1 during adjuvant chemotherapy and 2 patients died from non-cancer events. 7 patients died after recurrence at distant sites (adrenal gland, bones, liver). Cerebral recurrence was seen in only one patient who also had a history of malignant melanoma at 270 days after surgery. The proportion developing cerebral metastasis was 2.12% (95% CI 0% to 6.25%). If all patients were screened with head CT scanning and assuming all metastases were detected preoperatively, the cost of each case detected is £16 450 (95% CI £5597 to incalculable (0)).
Discussion: Studies pre-PET showed cerebral recurrence rates of 5.8–8.6% in the first 12 months.2 3 This study shows a recurrence rate of 2.1% (95% CI 0% to 6.25%). This suggests that the rate of recurrence postoperatively is lower in the post-PET era. Further larger prospective studies are required to assess the cost effectiveness of head screening prior to resection.

Kaplan-Meier survival curve for patients who have undergone a resection for non-small cell lung cancer, March 2007 to March 2008.
P19 UNEXPECTED FINDINGS COMPLICATE THE USE OF FDG-PET CT SCANS IN THE INVESTIGATION OF LUNG MALIGNANCY: EXPERIENCE OF ONE CANCER NETWORK
A. Murray, M. Walshaw. Merseyside and Cheshire Cancer Network Group, Merseyside and Cheshire, UK
Introduction: FDG-PET scans, recommended in the diagnosis and staging of lung cancer, use the avidity of metabolically active malignant tissue for radiolabelled glucose to define solid tumours. Although false positive results (an SUV within the malignant range) are produced by some inflammatory conditions, their incidence in a clinical population undergoing the diagnostic pathway is unknown. In 2008, an FDG-PET CT scanning service from a private provider was commissioned for our cancer network. We looked at the incidence and cause of false positive results and also the service performance against agreed waiting time targets (5 days to scan and 2 days to report).
Method: Five lung cancer units from the Merseyside and Cheshire Cancer Network audited 160 FDG-PET CT scans carried out February 2008 to April 2009 in the diagnostic investigation for suspected lung cancer. FDG avid lesions that did not represent lung cancer and their investigation and diagnosis were noted, and waiting time data (see above) were recorded.
Results: 129 scans (81%) showed non-lung cancer FDG avidity (upper gut 14 (9%), lower gut 47 (29%), thyroid 9 (6%), head and neck 55 (34%), musculoskeletal 14 (9%), others 35 (22%)), in 39 (30%) at multiple sites. Most underwent further investigation, including upper and lower gut endoscopy, ENT examination and MRI scans. Although 14 additional malignancies were uncovered (4 head and neck, 1 lower gut, 2 breast, 1 lymphoma, 1 thyroid, 3 prostate and 2 ovary), in 115 (89%) the avidity was unexplained and delayed the diagnostic pathway. With regard to waiting times, the median time to scan was 11 days (range 3–33) and then to report was 6 days (0–21), further delaying the diagnostic pathway.
Conclusions: The introduction of this new service has brought with it a high incidence of unexpected results from FDG-PET. Although some of these represented other malignancies, 72% of patients had unexplained findings that consumed valuable investigative resource and complicated their journey; this merits further research. We are working with the provider to improve the waiting time figures.
P20 PRE-PET CT-GUIDED BIOPSY OF SOLITARY PULMONARY NODULES REDUCES THE BENIGN RESECTION RATE IN A POPULATION WITH A HIGH INCIDENCE OF GRANULOMATOUS DISEASE WITHOUT AN UNACCEPTABLE COMPLICATION RATE
J. Evans, Y. E. Ong, S. Grubnic, N. Walters, F. Chua, A. Draper. St George’s Hospital, London, UK
Introduction: Some UK multidisciplinary teams (MDTs) now adopt the “positron emission tomography (PET) then resect” approach in the management of solitary pulmonary nodules (SPNs) without first confirming tissue diagnosis. Clifton et al demonstrated a benign resection rate of 7.9%.1 Mortality rates of 0.5–1% are quoted for wedge resection and 3–7% for lobectomy. It was our hypothesis that, in our population with high endemic incidence of granulomatous disease, the benign resection rate would be significantly higher. With the significant risk attached to surgical resection, we believed that our existing approach of utilising tissue confirmation via CT-guided biopsy was more appropriate for our population. We therefore reviewed cases of consecutive SPNs investigated by our lung MDT.
Method: Patients who underwent CT-guided biopsy for SPNs between January 2003 and December 2008 were included. Imaging, final tissue diagnosis and clinical records were reviewed.
Results: 220 patients (56% male, 44% female) were identified. The final pathological findings are shown in table 1. Only seven (10%) with a benign diagnosis underwent CT-PET scanning, five of which (71%) demonstrated FDG uptake. Pneumothoraces occurred in 21 (10%) following biopsy; three (1%) required drainage. Significant parenchymal haemorrhage occurred in two patients; both were managed conservatively without subsequent complication.
Final pathological diagnosis
Discussion: Use of CT-PET scanning in our MDT is generally limited to preoperative assessment of individuals with potentially resectable malignant disease but is occasionally used when spirometry is borderline for biopsy. Of benign cases, 10% underwent CT-PET scanning. It is interesting that 71% of these were falsely positive. Extrapolating data, if we adopted a “PET then resect” approach, as many as 49 individuals may have undergone resection giving a benign resection rate of 22%. Complication rates following CT biopsy were very low in our cohort, implying that use of this technique to obtain tissue was safe.
Conclusion: We conclude that, in an area with a high incidence of granulomatous disease, it is preferable to obtain a tissue diagnosis prior to surgery in order to prevent an unacceptably high benign resection rate.
References
P21 PROSPECTIVE DATA OF CONTINUOUS HYPERFRACTIONATED ACCELERATED RADIOTHERAPY (CHART) FOR NON-SMALL CELL LUNG CANCER (NSCLC): CLINICAL OUTCOME AND PATIENT SATISFACTION SURVEY OF THE NORTHERN REGIONAL CANCER CENTRE
H. W. Loo, R. Klapper, P. Mulvenna, R. McMenemin, F. McDonald, P. Atherton, G. Mazdai. Northern Centre for Cancer Care, Newcastle upon Tyne, UK
Background: The study on non-small cell lung cancer (NSCLC) by Saunders et al has shown CHART to give significant survival benefits compared with conventional radiotherapy. NICE guidelines recommend CHART in patients with stage 1 or stage 2 NSCLC who are medically inoperable and also in patients with stage 3 NSCLC who are unsuitable for multi-modality treatment. Our institute implemented CHART in 2005 and, to date, we have treated 115 patients. We prospectively collected data for all patients treated with CHART. The clinic data for the initial 70 patients are presented here.
Method: All patients referred for CHART were identified on the Lantis system. Data were collected from radiotherapy notes and case notes prospectively for all patients. Data of the initial 72 patients treated between August 2005 and August 2007 were retrieved. Patient satisfaction surveys were performed in May 2006 and June 2007. These surveys collected information on patient opinions on the quality of CHART service with regard to information provision, hospitality, treatment delivery, management of side effects and follow-up arrangement.
Results: Seventy patients referred for CHART completed treatment and two were deemed unsuitable on the basis of poor performance status and significant co-morbidities. 62% were stage 1 and 2 and 38% were stage 3. 60% of patients had biopsy-proven squamous cell carcinoma. There were 30 women and 42 men, with a median age of 72 years. Median overall survival was 20.4 months and median progression-free survival was 17.81 months. The toxicity profile of treatment was acceptable. No clearly demonstrable correlation between the length of the oesophagus in the high dose region and the severity of oesophagitis was observed. Radiation pneumonitis was suspected in seven patients (five showed radiological and clinical evidence of radiation pneumonitis and two showed only clinical evidence). All seven required prolonged steroid treatment. Information from two patient surveys carried out over the 2-year period showed a good level of satisfaction from our patients.
Conclusion: This prospective study showed that CHART treatment is a clinically effective treatment for NSCLC patients with manageable toxicities, and a high level of patient satisfaction was demonstrated by our survey.
P22 ARE INVASIVE DIAGNOSTIC TESTS PERFORMED JUSTIFIABLY IN PATIENTS WITH SUSPECTED PLEURAL/PULMONARY MALIGNANCY?
A. O. Dunscombe, R. K. Sinha. Yeovil District Hospital NHS Trust, Yeovil, UK
Background: Obtaining a tissue diagnosis in suspected pulmonary/pleural malignancy involves invasive investigations, sometimes associated with significant morbidity. In patients with a poor performance status, advanced disease or those not wanting treatment, a tissue diagnosis may therefore not be justified.
Method: We examined the notes of patients with a tissue diagnosis of pulmonary or pleural malignancy made in 2007 and 2008 who did not receive treatment. Patient characteristics, tumour stage, investigations performed, patients’ wishes and the reasons for treatment being withheld were documented. A blinded case scenario of each patient was presented to four members of the lung multidisciplinary team. They were asked to judge whether they felt the diagnostic investigation was justified.
Results: 152 patients were diagnosed with pulmonary/pleural malignancy in 2007/8. 28 patients (19%) had a tissue diagnosis but did not receive treatment. 20 patients were included in this study. The WHO performance score at the time of referral was 2 or more in 11 of the 20 cases. Eight patients (40%) underwent two or more invasive tests to obtain the diagnosis. In only two cases had the patient’s wishes prior to investigation been documented. Eight patients (40% of those in this study and 5.26% of the total number diagnosed in 2007/8) were considered to have undergone invasive tests unjustifiably by one or more of the clinicians. In four of these, all four clinicians agreed the test was not justified.
Conclusion: This study suggests that patients with suspected pulmonary/pleural malignancy may be subjected to unnecessary invasive tests. In 8 of 20 cases (40%) at least one clinician deemed the investigations to be unjustified, yet in reality these tests were performed. Potential reasons for this include: (1) pressures to meet diagnostic targets within specified timescales; (2) reluctance of clinicians to describe a hopeless situation during the first consultation with patients of borderline performance score; (3) inadequate discussion as to how investigations will alter management; (4) anxiety about missing an alternative treatable diagnosis. Earlier discussion in the multidisciplinary team, even before seeing patients in borderline cases, may help to minimise these difficulties and reduce futile tests being performed towards the end of a patient’s life.
P23 ANALYSIS OF METHODS OF OBTAINING TISSUE DIAGNOSIS IN PATIENTS WITH SUSPECTED LUNG CANCERS
A. K. Allouni, D. Lau, T. Meagher, E. Woo, A. Prasad. Buckinghamshire Hospitals NHS Trust, Buckinghamshire, UK
Introduction: Diagnosis and staging of suspected lung cancer should be timely and minimise the number of interventions to reduce patient risk and comfort. Good practice should aim to biopsy potential metastases to obtain a tissue diagnosis and stage in one procedure. We compared data from local practice reported in 2006 to look at trends of obtaining tissue diagnosis.
Methods: Database entries for all patients investigated for suspected lung cancer in 2008 were accessed and information on different types of procedures undertaken extracted. For each case, the histology record and radiology log were also cross-checked. Current data are compiled from two hospitals within the same trust, whereas the 2006 report was based on only one (table 1).
Results: 202 patients were identified. Of these, 13 (6.5%) were not investigated and given a clinical diagnosis of lung cancer based on radiology. Of those with a tissue diagnosis, 72% were non-small cell lung cancer, 14% small cell lung cancer, 9% mesothelioma and <1% sarcoma. Failure to obtain a tissue diagnosis was limited to only 5% of patients compared with 9% reported in 2006. 23% of patients underwent more than one procedure to establish a tissue diagnosis. Pleural fluid analysis in mesothelioma only gave the diagnosis in one case.
Discussion: These data demonstrate that diagnostic rates continue to be comparable to those in the literature and also that failure to obtain a tissue diagnosis has more than halved. The overall proportion of attempts at metastatic biopsy has remained constant, reflecting the proportion of patients presenting with advanced disease. However, the diagnostic rate of this modality continues to surpass other interventions. In cases where mesothelioma is the suspected diagnosis, opting first for an image-guided pleural biopsy would prevent unnecessary thoracocentesis. Careful selection of diagnostic modality should reduce the number of interventions needed to obtain a tissue diagnosis, thus reducing both morbidity and time to first treatment.
P24 SECULAR CHANGES IN THE USE OF INVESTIGATIONS AND TRAINING OPPORTUNITIES IN A LUNG CANCER UNIT
S. P. Hanley. North Manchester General Hospital, Manchester, UK
Significant changes in the investigation of lung cancer have occurred in the past 20 years, driven by reports such as the Standing Medical Advisory Committee’s “Management of Lung Cancer: Current Clinical Practices” in 1994 and the National Institute of Health and Clinical Excellence’s “Lung Cancer Diagnosis and Treatment” in 2005. Concurrently there has been a significant expansion of the trainee work force. Few data exist on the effects of these initiatives on lung cancer investigation and training opportunities. This abstract reviews the use and relationships of fibreoptic bronchoscopy, CT scanning of the thorax, percutaneous needle biopsy (PNB) and training opportunities in a DGH setting.
Data were analysed from a lung cancer database (Unisoft Ltd) between 1994 and 2007, the latter date being the latest for possible comparison with the cancer registry. The number of bronchoscopies/year, number/trainee/year, temporal relationship of CT scanning of the thorax to bronchoscopy and number of PNB/year were studied. Data quality for CT was undertaken by comparison with the radiology department master database and needle biopsy by comparison with a consultant personal log, undertaken as both data sets were transferred manually to the Unisoft database.
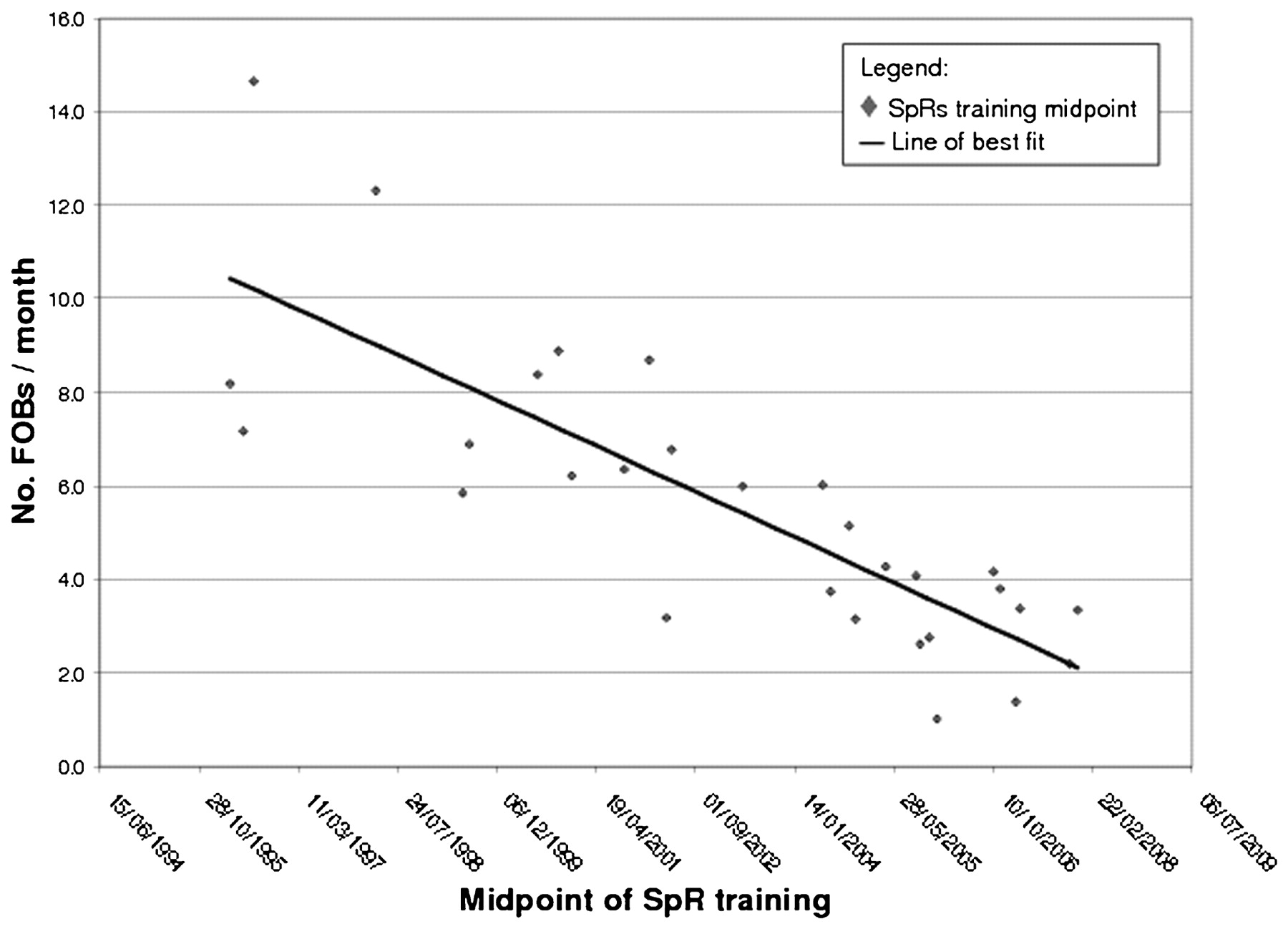
4605 first presentation bronchoscopies were performed, peaking at 445/year in 2000 and falling to 190/year by 2007. The number of bronchoscopies/month/trainee has progressively fallen from approximately 10/month in 1997 to 3/month in 2006 (fig 1). Progressively more CT scans were performed prior to bronchoscopy in the whole group (1994, <20%; 2007, >60%) and in the subset of patients with a final diagnosis of cancer (1994, <10%; 2007, >80%); the 50% breakpoint occurred in 2004. PNBs rose from <15/year in 1994 to >55/year in 2002, with a plateau thereafter. The majority of patients had a CT scan prior to PNB, the lowest proportion (85%) in 1995. Data quality assessment revealed that 88% of the CT scan reports on the radiology department database had been transferred to the Unisoft database and 95% of the PNBs from the consultants log had been transferred.
{kind=link}
{kind=link}
{kind=link}
Scatter plot to show bronchoscopy training opportunities for SPRs. FOB, fibreoptic bronchoscopy.
These data show clear trends in the timing and use of investigative techniques and significant loss of training opportunities.
P25 PERFORMANCE AND THEORETICAL COST ANALYSIS OF A RECENTLY DEVELOPED ENDOBRONCHIAL ULTRASOUND-GUIDED TRANSBRONCHIAL NEEDLE ASPIRATION (EBUS-TBNA) SERVICE IN A UK RESPIRATORY CENTRE
A. R. L. Medford, S. Agrawal, C. M. Free, J. A. Bennett. Glenfield Hospital, Leicester, UK
Background: New innovative techniques can improve patient care but may not be appropriately funded. Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) offers a minimally invasive mediastinal staging and diagnostic method for suspected lung cancer.
Aim: We report the performance and cost analysis of a newly established EBUS-TBNA service in a prospective real world cohort of patients to assess the impact of Payment by Results (PbR).
Design: Prospective cohort study.
Methods: 54 patients between June 2008 and April 2009 underwent EBUS-TBNA for evaluation of unexplained mediastinal lymphadenopathy on CT. Cost analysis was performed from local trust financial data and 2008/9 tariffs.
Results: EBUS-TBNA had a sensitivity of 89%, negative predictive value of 75% and accuracy of 92% for malignancy. EBUS coding was inaccurate in 15.6% of cases. The actual cost of an EBUS is £1252–1433 but is coded as a standard bronchoscopy (£561). EBUS reduces health community costs by £10 7824/year as a result of a Primary Care Trust (PCT) cost saving of £113 968/year and a trust cost deficit of £6144/year (table 1). Coding inaccuracies and variations further alter the PCT costs.
Conclusions: Medical innovation is fundamental to improved patient care. EBUS-TBNA is a new technique which can potentially reduce morbidity for lung cancer patients and save costs to the health community as a whole. However, with PbR the service provider delivers this at a loss due to failure of the tariffs to reflect this innovation and coding inaccuracies. We suggest the tariffs for innovative procedures need to be amended to reflect the true cost and allow patients to benefit.
P26 COMPARISON OF DEEP VERSUS LIGHT SEDATION ON DOCTOR, NURSE AND PATIENT ASSESSMENTS DURING FIBREOPTIC BRONCHOSCOPY WITH ENDOBRONCHIAL ULTRASOUND-GUIDED FNAC PROCEDURES (EBUS-TBNA)
1S. Naik, 2A. Mohan, 1M. Munavvar, 1S. Laurence. 1Royal Preston Hospital, Preston, UK, 2All India Institute of Medical Sciences, New Delhi, India
Introduction: Endobronchial ultrasound (EBUS) can be performed under both deep and light sedation. However, the superiority of one over the other as assessed by patients, doctors and nurses is not known. We conducted a prospective study to evaluate the relationship between the depth of sedation during EBUS with the quality and ease of the procedure along with patient comfort as assessed by the doctor, patient and assisting nurse.
Objective: To evaluate and compare the effect of light versus deep sedation during EBUS using a questionnaire-based assessment by doctors, nurses and patients.
Methods: Patients who underwent EBUS under light/deep sedation were included in a random manner. Deep sedation was administered by an anaesthetist using propofol, midazolam and ramifentanyl. Patients under light sedation received only midazolam and ramifentanyl. After each procedure the patient, doctor and attending nurse completed a questionnaire regarding ease of procedure, patient comfort and tolerability. All answers were marked on a score of 1–10, with a higher score indicating a better outcome. Average scores were calculated for each question and compared between the deep and light sedation groups. The total time taken for each procedure was also recorded.
Results: Eighty-eight patients were evaluated, 48 of whom received deep sedation while 40 received light sedation. The mean (± SD) duration of the EBUS was comparable in both groups (28.55±5.92 min and 30.83±4.64 min, respectively). The mean scores in the deep versus light sedation groups were 8.62 and 7.73 by doctors, 8.25 and 7.58 by nurses, and 8.70 and 6.98 by patients.
Conclusions: EBUS performed under deep sedation was ranked better by the operating doctor, nurse and, more importantly, by the patient without any significant prolongation of total procedure time. We feel that performing EBUS under deep sedation provides better patient comfort and assists the operator.