Article Text

Statistics from Altmetric.com
First-degree atrioventricular (AV) block is a relatively common electrocardiographic finding, defined as PR interval >200 ms. Traditionally, isolated first-degree AV block or PR prolongation had been considered as a benign phenomenon, but this perception has been challenged by a report from the Framingham Heart Study, suggesting that first-degree AV block was associated with increased risk of atrial fibrillation, pacemaker implantation and all-cause mortality in this population.1 This, together with the ongoing search for non-invasive risk markers for prediction of cardiovascular disease, has sparked a renewed interest in first-degree AV block, resulting in the publication of a dozen studies on its prognostic significance during the last 7–8 years. However, results have been mixed, and the clinical significance of PR prolongation has remained elusive.
Consequently, the current meta-analysis on the prognostic significance of prolonged PR interval by Kwok et al in Heart2 is a welcome addition to the literature. Their analysis was conducted from 14 studies published between 1972 and 2011, the majority in recent years, with >400 000 participants. Some of the individual studies included in the meta-analysis demonstrated increased risk of adverse outcomes associated with prolonged PR interval, while others suggested no clinical significance. When studies performed in the general population and adjusted for potential confounders were combined, PR prolongation was associated with 39% increased risk for heart failure (three studies) and 45% increase in atrial fibrillation (eight studies). Moreover, prolonged PR interval was associated with 24% increased risk in all-cause mortality (five studies), but somewhat paradoxically, with no additional cardiovascular mortality (three studies).
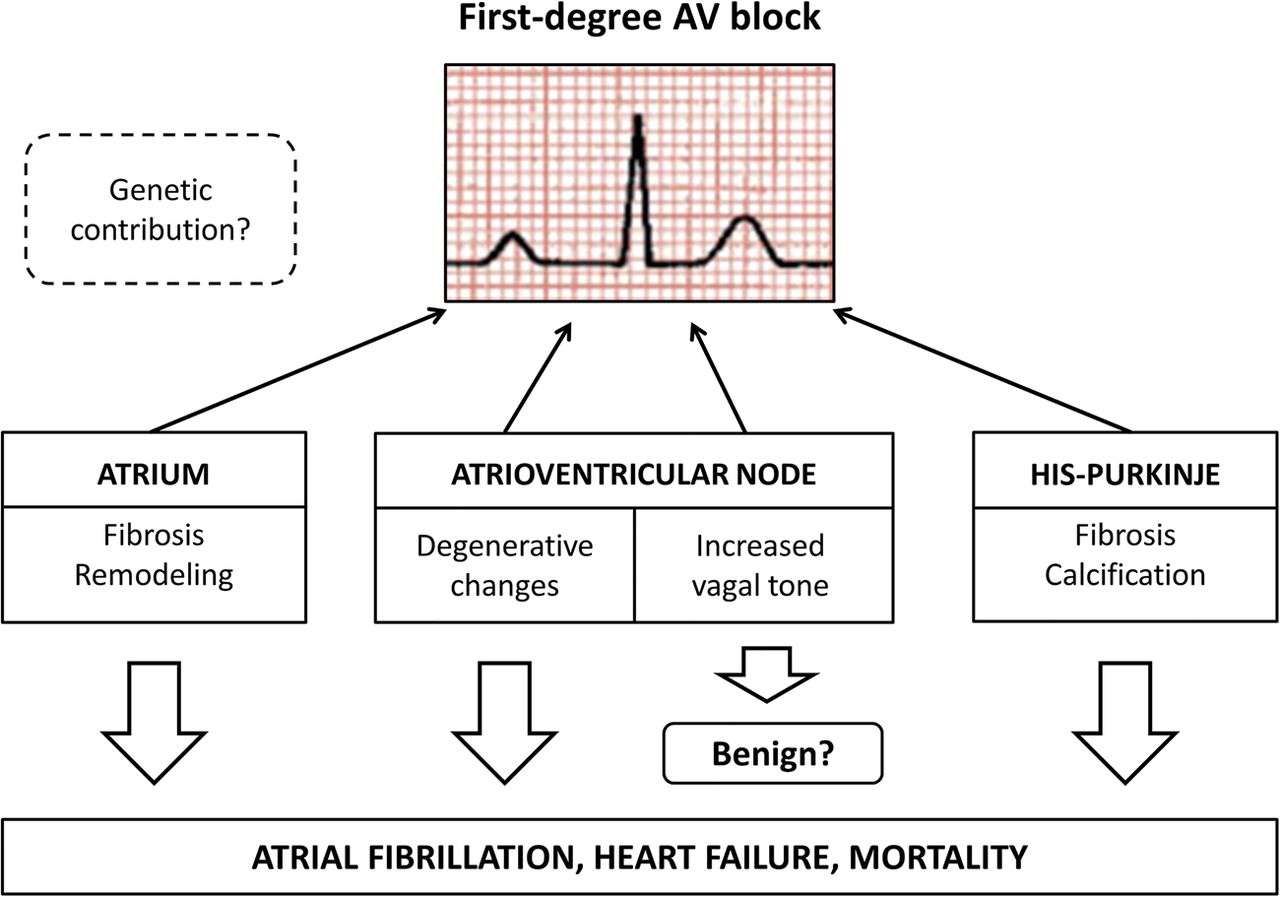
To understand the reasons behind the varying conclusions reached in different studies, one could consider the different components contributing to the PR interval. To reach the ventricles, the electrical impulse initiated in the sinus node travels from adjacent atrial myocardium to the AV node, to finally reach the bundle of His and Purkinje fibres. Thus, the PR interval is like a composite measure representing a combination of these three different components (figure 1). Consequently, a conduction delay in any of these structures can cause prolongation of the PR interval. Under normal physiological conditions, conduction delay in the AV node is the biggest contributor to the PR interval. The AV node is strongly influenced by the autonomic nervous system, and prolonged PR interval due to increased vagal tone and decreased resting sympathetic tone is a common finding in conditioned athletes. Therefore, in some populations PR prolongation may be a marker of physical activity and healthy lifestyle, thus associated with favourable outcomes. Probably largely due to this strong autonomic influence, PR prolongation is not always a permanent finding, but a transient phenomenon in a significant number of healthy individuals.3
{kind=link}
Factors associated with PR prolongation and their clinical significance. AV, atrioventricular.
Ageing is another factor associated with prolongation of the PR interval, but the underlying mechanisms are quite different. In the elderly, electrical and structural remodelling such as atrial fibrosis together with calcification and fibrosis of the conduction system may play a more important role in the development of PR prolongation. Electrophysiological studies have demonstrated that ageing results in decelerated conduction times in the atria, AV node and the distal conduction system. These degenerative changes and fibrosis of the atria and the ventricles, reflected in the ECG as PR prolongation, can predispose the individual to a higher risk of atrial arrhythmias and heart failure. Consequently, PR prolongation has been included in some algorithms for atrial fibrillation risk prediction.4
In recent years, the potential role of a genetic component that determines the PR interval has been a subject of growing interest. Genetic studies have demonstrated that the PR interval shows significant heritability and overlap with genetic variation in atrial fibrillation. In genome-wide association studies, chromosome loci of voltage gated sodium channel genes and cardiac developmental genes have been associated with the PR interval and also with atrial fibrillation.5 However, because atrial fibrillation and conduction abnormalities are likely to be multifactorial in the majority of individuals, genetic contribution is likely to play a limited role in the observed association between PR prolongation and both increased mortality as well as risk of atrial arrhythmias.
The P-wave is a major component of the PR interval, and P-wave prolongation and abnormal morphology have been constantly associated with adverse outcomes, including increased risk of atrial arrhythmias and mortality.6 ,7 There is emerging evidence, that varying contributions of P-wave duration to the PR interval may explain some of the heterogeneity in the association with PR interval with morbidity and mortality. Soliman et al using the data from the Third National Health and Nutrition Examination Survey (NHANES III) demonstrated that P-wave largely dictates the prognostic significance associated with PR prolongation. They reported that both long and short PR intervals were associated with mortality in participants with high contribution of P-wave duration to PR interval.8 However, since specific information on the P-wave has been rarely reported in the studies addressing PR prolongation, it would not have been possible to explore the implications of the relative contribution of the P-wave to PR interval in the current meta-analysis.
As for all meta-analyses, the main limitation in generalising the results of this work lies in the possible heterogeneity of the studies included. In a relatively young population, incident PR prolongation is likely to be a finding with excellent prognosis.3 In contrast, among older patients with other conduction disturbances or coronary artery disease, first-degree AV block is more likely to reflect more diffuse underlying cardiac pathology, accounting for the association of PR prolongation with mortality and increased risk of atrial fibrillation and heart failure.2 However, in the final analysis, Kwok et al remind us that measurement of the PR interval is an integral part of ECG evaluation, but the astute clinician should interpret this important variable in the context of the individual patient. In future studies, it would be useful to better define the group of patients in whom PR interval adds value to conventional risk stratification, perhaps focusing on subjects with intermediate or higher risk at baseline. Moreover, the individual contributions of the P-wave versus remaining PR interval versus total PR interval to predicting risk of atrial fibrillation and overall mortality warrants further investigation.
Footnotes
Funding Finnish Cultural Foundation.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.