Article Text

Statistics from Altmetric.com
Learning objectives
-
1. Coronary physiology
-
2. Exercise physiology
-
3. Events that precipitate acute coronary syndrome and angina
Curriculum topic
Acute coronary syndromes
Introduction
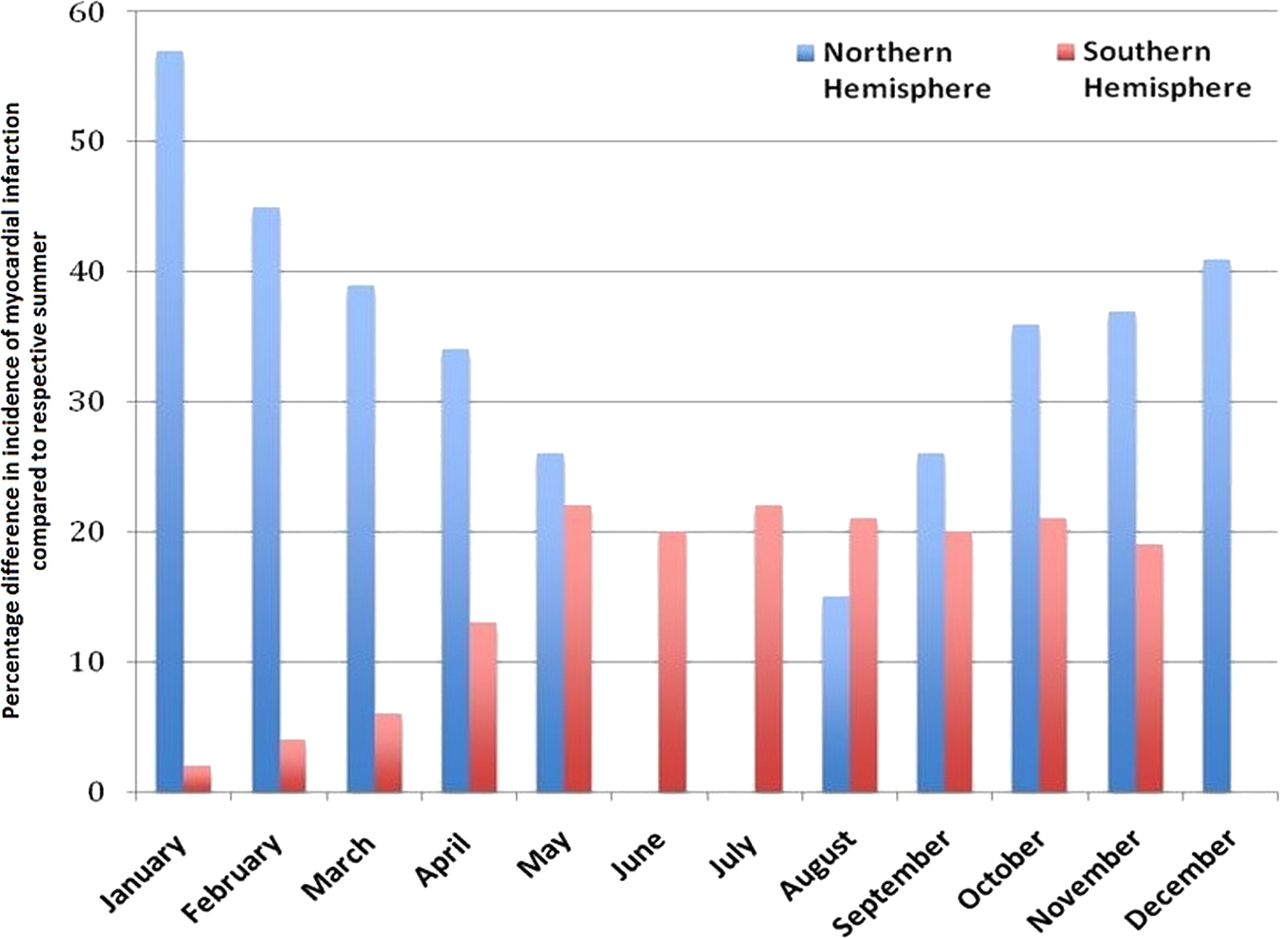
Decreased exercise tolerance and worsening of angina symptoms during the winter months is a well-documented phenomenon among patients with coronary artery disease (CAD).1 There is a significant increased risk of acute myocardial infarction (AMI) with cold temperatures,2 even when taking into account confounding factors such as altered glucose and cholesterol levels and higher incidence of respiratory infections.3 ,4 When comparing seasonal differences in the northern and southern hemispheres, a higher incidence of AMI correlates with periods of cold weather in both hemispheres (figure 1).5 ,6 The risk of AMI in cold temperatures is further increased if exercise is being performed. Notable examples are shovelling snow7 and downhill skiing,8 which involve significant isometric exercise and dynamic exercise components. While epidemiological studies suggest a strong link between exercising in the cold and AMI, a causal relationship is yet to be demonstrated.

Seasonal differences in the incidence of myocardial infarction in the northern and southern hemispheres. This figure represents data from two observational studies investigating the incidence of myocardial infarction in the northern (the USA) and southern (Australia) hemispheres. The figure demonstrates the percentage change in the incidence of myocardial infarction compared with their respective winters. Of note the average temperatures in the summer months for the northern and southern hemispheres were 21°C and 22°C, whereas the winters were significantly colder in the northern hemispheres, 2°C vs 10°C. This might explain the greater seasonal variation in the northern hemisphere. Adapted from Loughnan et al5 and Spencer et al6.
The exact mechanism by which cold increases the risk of AMI remains unclear. Proposed mechanisms include a myocardial oxygen supply and demand mismatch or an increased risk of plaque rupture. This article outlines the effects of (a) cold stress, (b) exercise stress and (c) the combination of exercise and cold stressors on the cardiovascular system in both healthy individuals and patients with CAD.
Learning objectives
1. Coronary physiology
2. Exercise physiology
3. Events that precipitate acute coronary syndrome and angina
A brief outline of coronary physiology
Even at rest, cardiac muscle has a high metabolic demand and myocardial extraction of oxygen from the blood is significantly higher than in other organs.9 Thus, any increase in oxygen demand is mainly met by modulating coronary blood flow (CBF).10 CBF is directly dependent on coronary perfusion pressure and inversely dependent on coronary vascular resistance (CVR).
Coronary autoregulation
Larger epicardial arteries conduct perfusion pressure without significant pressure loss,11 whereas in coronary resistance vessels, particularly those whose diameter is <400 μm, perfusion pressure declines rapidly. This would result in a reduction in CBF12 but for compensatory myogenic mechanisms resulting in dilatation of these arterioles to maintain flow at a steady state.10 This is known as coronary autoregulation. This ensures that, at a constant myocardial oxygen demand, CBF is relatively independent of perfusion pressure, for a physiological range of perfusion pressures (figure 2).13–15
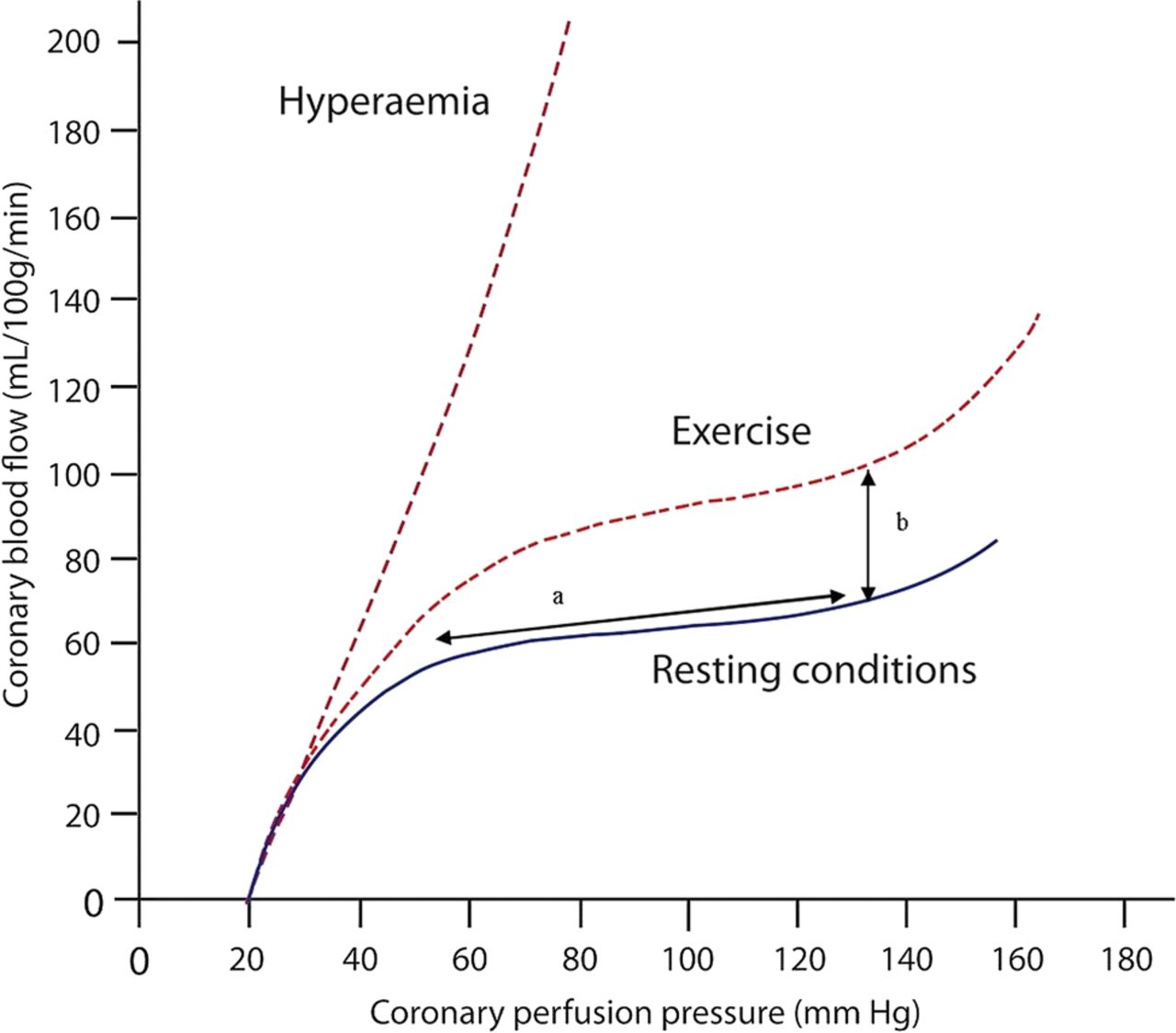
Coronary pressure–flow relationship. (A) Within a physiological range of perfusion pressure, coronary blood flow remains constant. Termed autonomic autoregulation. (B) During exercise, an increase in myocardial oxygen demand results in an increase in the autoregulatory plateau termed metabolic adaptation. Reprinted with additions, with permission from Heart. Original from van de Hoef et al.13
Metabolic adaptation
During resting conditions, as perfusion pressure rises an autoregulatory plateau is reached. However, this plateau may be augmented to meet increased myocardial oxygen demand, such as during exercise (figure 2).13 This process is known as metabolic adaptation.13–15 As myocardial oxygen consumption (MVO2) increases, the resistance of the coronary microvasculature is further decreased. This is mediated by release of endothelial factors and enhanced metabolite production in response to increased shear stress and increased cardiac work, respectively. These factors also result in vasodilatation of coronary arteries.10 Metabolic adaptation allows CBF to match myocardial oxygen demand during periods of physiological stress. However, in the context of CAD, endothelial dysfunction and coronary artery stenoses (discussed below) may disrupt metabolic adaptation.
Effect of a coronary artery stenosis
The pressure–flow relationship is altered in the presence of a flow-limiting stenosis. Friction (Law of Poiseuille) and exit losses (Law of Bernouilli) lead to a pressure drop across the stenosis.16 ,17 Compensatory vasodilatation of the resistance vessels preserves basal CBF at the expense of coronary flow reserve (CFR), which is attenuated. CFR is the ratio of maximum to basal coronary flow (figure 2).13 ,18
During hyperaemia, either physiologically from exercise or pharmacologically from administration of a potent vasodilator, the relationship between coronary pressure and flow tends more towards linearity, as the coronary vascular bed has achieved complete vasodilatation (figure 2).13 In the presence of a stenosis, CBF increases by smaller increments than would be elicited without a stenosis because of progressive exhaustion of the vasodilator reserve of the resistance vessels.13 At higher MVO2, myocardial oxygen supply may no longer be able to match myocardial oxygen demand, resulting in ischaemia.13
Effects of cold stress on the cardiovascular system
Cold leads to a range of physiological responses to prevent a fall in core temperature, which can have important consequences for subjects with CAD (figure 3).

Physiological effects of the cold. Exposure to the cold causes a range of reflex physiological responses in the human body, involving a range of systems. DBP, diastolic blood pressure; SBP, systolic blood pressure; SVR, systemic vascular resistance.
Models of cold stress
A variety of research models have been used to investigate cold stress. These include cold air inhalation (cold air applied through a facemask or mouthpiece), cold pressor (immersion of a limb in cold water), cutaneous cold application (external application of cold onto body surface, often face) and cold chamber (entire body exposure to a cold environment).
Full-body submersion in cold water with attempted breath-holding activates two powerful conflicting autonomic reflexes: the cold shock reflex and the diving reflex.19 The cold shock reflex is driven by cutaneous cold thermoreceptors that stimulate the sympathetic nervous system to cause peripheral vasoconstriction and prevent heat loss from the surface of the body.19 The diving reflex, driven by activation of facial trigeminal receptors, results in parasympathetic stimulation. This leads to decreased oxygen consumption and prolongs time underwater.19 Therefore, protocols, which involve cold application to the face, such as cold air inhalation, will likely activate both of these responses.
Of all the cold stresses described, the cold pressor test is much more easily applied within a research protocol and has therefore been most extensively studied. The cold pressor test was initially criticised as demonstrating the effects of a painful stimulus rather than a cold stimulus;20 however, the cardiovascular effects have since been shown to persist after thoracic anaesthesia, suggesting that primarily adaptation to cold was occurring.21
In healthy subjects
Myocardial oxygen demand
Cold typically produces an increase in heart rate (HR) of 5–10 bpm and an increase in systolic blood pressure (SBP) of 15–20 mm Hg.22–25 Studies in which cold air inhalation was used showed a blunted HR response26 ,27 compared with the cold pressor test,22 likely because trigeminal nerve activation resulted in vagal opposition to the sympathetic response to cold.27
Skin surface cooling causes peripheral vasoconstriction,28 increasing systemic vascular resistance (SVR)29 and diastolic blood pressure (DBP).22 ,23 ,29 The resulting increase in afterload would be expected to diminish stroke volume (SV). However, this is not found to be the case, likely because the increase in afterload is offset by an increase in preload through increased central venous pressure.29
Rate pressure product (RPP), which is calculated by central SBP multiplied by HR, is a surrogate marker of myocardial work30 and at higher HRs is one of the more accurate indices of myocardial oxygen consumption (MVO2).31 RPP increases with cold22–26 reflecting increasing MVO2.
The central pressure that LV must overcome influences wall tension and myocardial oxygen demand; this in turn is elevated by the augmentation index (AI). AI is an indicator of systemic arterial stiffness and increases with cold.32 ,33 This further increases afterload and LV work with cold.
Myocardial oxygen supply
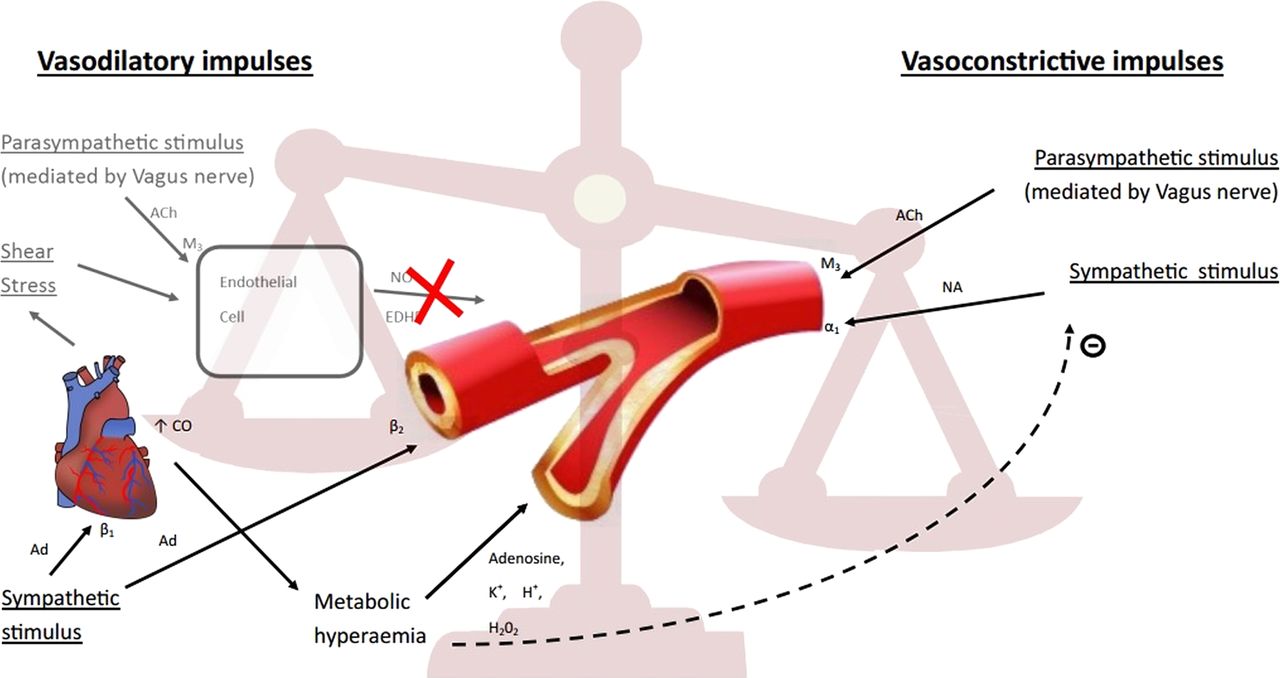
Since cold increases myocardial oxygen demand and activates the sympathetic nervous system, it would be expected to increase CBF (figure 4). Indeed, CBF has been demonstrated to increase in healthy subjects in response to a cold stress stimulus. This has been achieved with several different experimental protocols.

Vasomotor response of healthy coronary artery to cold stress. The vasodilatory impulse arises from (A) NO and EDHF released from arterial endothelial cells in response to parasympathetic stimulation of M3 ACh receptors and by increased shear stress; (B) direct β2-adrenoceptor-mediated response to increased adrenaline concentration; (C) increased cardiac work causes a metabolic hyperaemia, mediated by various metabolites (eg, adenosine, K+, H+, H2O2). This metabolic hyperaemia also reduces sympathetically mediated NA release. The vasoconstrictive impulse arises from (A) NA release via sympathetic activation of α1-adrenoreceptors and (B) direct M3 ACh receptor stimulation by the parasympathetic nervous system. In healthy coronary arteries, the vasodilatory response overcomes the concomitant vasoconstrictive impulse; vascular tone decreases, coronary blood flow increases and myocardial perfusion is maintained. Ach, acetylcholine; Ad, adrenaline; CO, cardiac output; EDHF, endothelium-derived hyperpolarising factor; M3, muscarinic receptor; NA, noradrenaline; NO, nitric oxide; α1, α1 adrenergic receptor; β2, β2 adrenergic receptor.
Myocardial blood flow (MBF) increases with cold and has been assessed through both positron emission tomography (PET)22 and cardiac magnetic resonance (CMR),34 with the higher spatial resolution afforded by CMR studies allowing discrimination of subendocardial MBF from subepicardial MBF.
Coronary sinus thermodilution has also been used to show an increase in coronary sinus flow associated with a reduction in CVR in response to the cold pressor test.35 However, conclusions drawn from this technique are limited due to subsequent data demonstrating the technique to be inaccurate and highly dependent on the position of the catheter.36
CBF can also be approximated using transthoracic Doppler echocardiography measurement of CBF velocity. In response to the cold pressor test, CBF velocity increased alongside an increase in RPP.37 However, cold air inhalation was shown to have no effect on CBF velocity.26 There are several reasons for this discrepancy: first, the cold pressor test arguably provides a more potent sympathetic stimulus than cold air inhalation. Second, the cold air stimulus was applied through a mouthpiece and therefore no stimulation of the trigeminal facial region occurred. Finally, the technique of transthoracic Doppler echocardiography to measure CBF velocity has also been criticised as having poor accuracy and reproducibility38 despite recent advances with the technique.39
Furthermore, quantitative coronary angiography has been used to demonstrate coronary vasodilatation in response to cold, alongside direct measurement of an increase in CBF with an intra-coronary angioplasty wire containing a Doppler ultrasound scan sensor on its tip.40
In subjects with CAD
Myocardial oxygen demand
As with healthy subjects, cold increases HR and SBP in subjects with CAD.25 ,41 ,42 Cold provokes angina in subjects with CAD41 ,43 and results in a higher RPP when undergoing cold air inhalation compared with rest.43 RPP at the anginal threshold during cold air inhalation is considerably lower than the anginal threshold during atrial pacing, indicating that ischaemia is occurring at a lower MVO2.43 A possible explanation for this is that even though myocardial oxygen demand is increasing, supply does not increase sufficiently to prevent myocardial ischaemia under cold stress.
Myocardial oxygen supply
Coronary artery stenosis results in exhaustion of the vasodilator reserve of the resistance vessels and a diminished flow-mediated metabolic vasodilatory response to cold. Atherosclerosis, via endothelial dysfunction, attenuates endothelial-mediated vasodilatation in response to cold (figure 5).25 ,44 A similar impairment of flow-mediated vasodilatation has also been observed in subjects with vasospastic angina when exposed to the cold.45

Vasomotor response of atherosclerotic coronary artery to cold stress. Vasodilatory impulses arise from (A) direct β2-adrenoceptor-mediated response to increased adrenaline concentration and (B) metabolic hyperaemia resulting from increased cardiac work (as per figure 4). Note there is minimal contribution from NO and EDHF due to endothelial dysfunction. Vasoconstrictive impulses are the same as in healthy coronary arteries. Due to a relative lack of NO and EDHF, vasoconstriction impulses dominate on coronary arterial vessel tone. In addition to the direct effects of a dominant vasoconstrictive vasomotor response, coronary blood flow will be further impeded by the presence of significant coronary artery stenosis. Ach, acetylcholine; Ad, adrenaline; CO, cardiac output; EDHF, endothelium-derived hyperpolarising factor; M3, muscarinic receptor; NA, noradrenaline; NO, nitric oxide; α1, α1 adrenergic receptor; β2, β2 adrenergic receptor.
Failure of vasodilatation in patients with CAD subjected to cold prevents an increase in CBF. This has been demonstrated with a number of experimental protocols.
PET studies have demonstrated no change in MBF in response to a cold pressor test compared with rest. Moreover, when corrected for RPP, subjects with CAD demonstrated a 20% reduction in MBF.46 Xenon clearance studies have also demonstrated no significant changes in CBF during cold air inhalation in subjects with CAD.43
There is also a proposed direct action of cold on the production and release of vasoconstrictive peptides in subjects with CAD, although specific substances have not been identified.42 Quantitative coronary angiography studies have supported this concept with coronary vasoconstriction demonstrated in subjects with CAD undergoing a cold pressor test compared with vasodilatation seen in healthy subjects.40 ,47
Coronary sinus thermodilution techniques have demonstrated no change in coronary sinus flow, and indeed showed a relative reduction in subjects with CAD, which was associated with an increase in CVR (calculated as mean arterial blood pressure divided by great cardiac vein flow).35 This was despite an increase in mean arterial blood pressure. However, in a different cohort with minor coronary atheroma, a small but significant increase in coronary sinus flow was demonstrated with a mild reduction in CVR.48 As mentioned previously, however, there is doubt as to the accuracy of great cardiac vein thermodilution to assess CBF.36
Studies using more accurate intracoronary measurement of CBF are needed to establish the exact mechanism underlying the diminished CBF responses to cold seen in subjects with CAD.
Risk of plaque rupture
Postmortem studies have demonstrated plaque rupture as the precipitating cause for up to 75% of AMIs.49 It has been hypothesised that cold stress may have detrimental effects on plaque stability and may account for the higher incidence of AMIs during cold conditions. However, risk of plaque rupture is not amenable to prospective physiological exploration in humans.
Animal studies have helped to share some light on this. Twenty mice exposed to a cold chamber (4°C) for 8 weeks had elevated low-density lipoprotein (LDL) cholesterol levels and a marked increase in plaque and necrotic core areas and decrease in fibrous cap thickness compared with mice exposed to 30°C.50 Interestingly these changes were nearly completed prevented by a specific β3-adrenoceptor antagonist, suggesting cold-induced sympathetic activation is a central component. The same authors demonstrated increased LDL cholesterol levels in five humans exposed to 16°C for 2 days, wearing standard semi-nude cloth, although given the extremely low numbers recruited this can only be hypothesis-generating data.50
In addition to chronic cold exposure, brief (1 h) cold exposure has long been shown to induce platelet aggregation from in vitro studies.51 A large in vivo study has also demonstrated a significant increase in coagulation factors in patients on days with a mean temperature of <20°C versus days with a mean temperature >20°C.52 However, there is no study that has specifically demonstrated an increased incidence of plaque rupture or coronary thrombosis in response to a transient cold stimulus.
Risk of cardiac arrhythmias
Sudden cardiac death is largely attributed to fatal cardiac arrhythmias. Cold water submersion, with breath holding, has been shown to induce higher incidence of cardiac arrhythmias in healthy volunteers, particularly junctional complexes and supraventricular tacchycardias.53 ,54 Indeed, it is believed that a proportion of dry drownings, when water does not appear to have entered the lungs, may have been due to cold-induced cardiac arrhythmias.19 However, the undetectable nature of arrhythmias in postmortems makes this a difficult hypothesis to prove.
The above phenomenon is believed to be due to dual activation of the sympathetic and parasympathetic nervous system by the cold shock reflex and the diving reflex.19 If indeed cold air exposure, particularly in the facial area, proves to be a pro-arrhythmic stimulus, then the vulnerability of subjects with CAD to cold due to a cardiac supply demand mismatch would be further amplified by concomitant cold precipitated arrhythmias. However, further studies are required into whether cold stress causes arrhythmias and the mechanism behind this.
Effects of dynamic exercise on the cardiovascular system
Dynamic exercise results in contraction of muscles with movement at the joint. The cardiovascular system responds during dynamic exercise to increase blood flow to the skeletal muscles and reduce blood flow to the viscera (figure 6).

Circulatory response to dynamic exercise. Dynamic exercise causes a range of cardiovascular responses mediated by activation of the sympathetic nervous system and withdrawal of the parasympathetic nervous system. CBF, coronary blood flow; DBP, diastolic blood pressure; HR, heart rate; SBP, systolic blood pressure; SV, stroke volume; SVR, systemic vascular resistance. .
In healthy subjects
Myocardial oxygen demand
Activation of the sympathetic nervous system and withdrawal of vagal control stimulates an increase in HR,55 SBP55 and contractility;9 ,56 DBP remains relatively constant.55 Despite an increase in vasomotor tone,57 ,58 β2 receptor activation59 and local metabolite production60 result in vasodilatation of muscular arteries. This reduces SVR and increases blood flow to exercising muscle. The redistribution of peripheral blood volume away from the viscera,61 and the effect of the ‘muscle pump’62 and ‘respiratory pump’,63 increase venous return.64 ,65 SV increases with exercise due to myocardial contractility increasing,9 venous return increasing64 (Frank–Starling mechanism) and afterload decreasing.66
Cardiac output (CO) therefore increases during dynamic exercise,67 with HR becoming the more significant determinant in the later phases of exercise when SV augmentation plateaus. With increasing CO and myocardial work, MVO2 increases. Indeed RPP, and therefore myocardial oxygen demand, increases with exercise.55
In subjects with CAD
Myocardial oxygen demand
Dynamic exercise increases HR and SBP, while DBP remains relatively constant in subjects with CAD;68 ,69 RPP increases, reflecting higher MVO2.68 ,69
Investigation of subjects with CAD during cardiac catherisation using supine cycle ergometers allows assessment of central arterial pressure waveforms and pulse waves during exercise. Central arterial pressure waveforms were measured using an angioplasty high-fidelity pressure wire placed in the aortic root.70 AI decreases during exercise and is used to infer afterload.70 AI is calculated from the aortic waveform as the difference in the two SBP peaks expressed as a percentage of the pulse pressure. A decreasing AI indicates a reduction in central SBP wave reflection due to vasodilatation of the systemic muscular arteries, which reduces LV work due to decreased afterload.70
Tension time index (TTI), calculated from the systolic area of the aortic pressure waveform, is proportional to myocardial oxygen demand. This has been shown to not significantly change during exercise, because although SBP increases, LV ejection time and AI also decrease.70 However, at higher HRs, RPP correlates more closely with MVO2 than does TTI.31
Myocardial oxygen supply
During dynamic exercise, vasodilatation of coronary arterioles, noted by a reduction in CVR, is required to maintain CBF velocity.70 CBF has been shown to increase even in subjects with CAD,71 but not as much as in healthy subjects.9 In subjects with CAD, the smaller residual vasodilator capacity results in a lower capacity of metabolic adaptation during exercise.9 ,13
When angina occurs during exercise, it is due to the increase in CBF being insufficient to meet the increased myocardial oxygen demand.9 ,40 This is likely due to (a) the dysfunctional endothelium being unable to produce endothelium-derived factors to cause adequate coronary vasodilatation72 and (b) a significant reduction in perfusion pressure distal to a significant coronary artery stenosis.13
Further insight into myocardial oxygen supply during dynamic exercise can be gained from the diastolic time index (DTI). Like TTI this is derived from the aortic pressure trace but is calculated from the diastolic area of the waveform. DTI is proportional to myocardial perfusion.70 As with healthy subjects, the relative diastolic time fraction is reduced with increasing HR. Indeed, DTI decreases during exercise, indicating reduced coronary perfusion drive in exercising subjects with CAD.70 Although CBF velocity does increase, perfusion to the vulnerable subendocardial layer may be compromised in the presence of a flow limiting coronary stenosis.
Effects of training
Regular exercise reduces all-cause mortality, and particularly cardiovascular morbidity and mortality.73 Dynamic exercise training leads to adaptations in the cardiovascular system to maximise efficiency by increasing maximal CO and maximal total body oxygen consumption.9 Exercise training increases basal parasympathetic tone and lowers circulating catecholamines, which reduces HR at rest and during submaximal exercise.74 This reduces myocardial oxygen demand.
AI also decreases in subjects with CAD following 12 weeks of dynamic exercise training.75 With reduced systemic arterial stiffness and therefore afterload that LV must overcome, training may result in a decrease in myocardial oxygen demand. In subjects with CAD, this may translate into achievement of a higher level of exercise before their ischaemic threshold is reached.76
A lower HR reduces systolic duration relative to the duration of each cardiac cycle. This reduces systolic compression of intramural coronary vessels and thus decreases the net impedance to CBF.9 Exercise training increases CBF for the same degree of myocardial work in healthy subjects through a variety of structural and functional adaptations in the coronary circulation.77 In particular, there appears to be a beneficial effect on arterial endothelial function, attenuation of acetylcholine-driven vasoconstriction, increased nitric oxide production and sensitisation of the microvasculature to adenosine-mediated vasodilatation.78 Furthermore, while training in subjects with CAD has been shown to increase collateral vessel growth, no such phenomenon has been observed in healthy subjects.9
Effects of isometric exercise on the cardiovascular system
Isometric exercise involves sustained muscle contraction with no change in length of the involved muscle group or joint motion. Isometric exercise causes a pressure load on the heart in contrast to the volume load exerted by dynamic exercise79 (figure 7).

Circulatory response to isometric exercise. Unlike dynamic exercise, isometric exercise causes no change in SVR and SV, and the increase in cardiac output is primarily driven by the increase in HR. CBF, coronary blood flow; DBP, diastolic blood pressure; HR, heart rate; SBP, systolic blood pressure; SV, stroke volume; SVR, systemic vascular resistance.
In healthy subjects
Myocardial oxygen demand
The cardiovascular responses to dynamic and isometric exercise differ in several important ways. Dynamic exercise results in functional hyperaemia in the exercising muscle.80 This local vasodilatation is restricted in isometric exercise due to the sustained mechanical compression of these vessels by the contracting muscle fibres.81 Both SBP and DBP increase in isometric exercise, so maintaining perfusion of the contracting muscle.55 ,80 ,82
The autonomic response to isometric exercise is biphasic, with vagal withdrawal followed by sympathetic activation.83 The SBP rise26 ,55 ,84 is driven largely by an increase in CO;85 ,86 SVR remains unchanged87 or increases.88 End diastolic volume does not change84 and SV remains constant89 or decreases.88 Therefore, the increase in CO is primarily driven by an increase in HR.90 With LV end diastolic pressure remaining unchanged and CO increasing, it is suggested that isometric exercise results in increased myocardial contractility without employing the Frank–Starling mechanism.85
Cardiovascular adjustments to isometric exercise do not reach a steady state, unlike with dynamic exercise. At levels >20% of maximal voluntary contraction, HR and mean blood pressure increase linearly until fatigue intervenes to stop the exercise.90
As would be expected, isometric exercise leads to increased myocardial work and RPP increases.26 ,84 AI was measured by invasive blood pressure monitoring and was used to infer LV work in healthy subjects performing handgrip exercise. AI increased with isometric exercise, indicating greater afterload and LV work.33
Myocardial oxygen supply
CBF velocity assessed with transthoracic Doppler echocardiography has been shown to both increase26 and remain constant37 ,91 during isometric exercise in healthy subjects. The percentage of maximum effort is not constant within these studies, which makes interpretation of the true effect difficult.
In subjects with CAD
Myocardial oxygen demand
In subjects with CAD, HR, mean arterial pressure (MAP) and CO increase as with healthy subjects and there is no change in SVR.85 Therefore, RPP and MVO2 increase.
The heart tolerates a higher pressure load less well than a higher volume load.90 As a result, subjects with established CAD are put at higher risk of ischaemia from isometric exercise than from dynamic exercise. This manifests as an earlier precipitation of angina in subjects performing dynamic exercise with arms outstretched,90 which adds an isometric component to the dynamic exercise. A direct comparison of equivalent isometric and dynamic exercises is difficult to conduct reliably.
Effects of training
Isometric exercise training does not increase volume load to the heart and, as such, the cardiovascular adaptations are different to those seen with dynamic exercise.79 Isometric training does little to improve aerobic capacity or cardiovascular efficiency96 as the poorly perfused muscles undergo mainly anaerobic glycosis. Isometric training leads to no significant sustained changes in SV or CO,97 and there is no adaptation to a lower resting HR,98 unlike with dynamic exercise. Interestingly isometric training does lower resting blood pressure, although no mechanism has currently been identified for this;99 there are likely specific roles for the sympathetic nervous system, SVR and oxidative stress.100
Effects of cold and exercise on the cardiovascular system
In healthy subjects
Myocardial oxygen demand
Individually, both cold and exercise increase indices of myocardial oxygen demand. When these two stresses are combined, the effect on myocardial oxygen demand is additive with an augmented increase in RPP.26 ,101 Cold and exercise result in a higher SVR and SBP compared with exercise alone.102 There is some indication that the increase in RPP in dynamic exercise and cold is primarily driven by the rise in SBP,102 ,103 while in isometric exercise and cold the increase in HR plays a greater role in increasing RPP.26 ,101 ,104 However, it is difficult to compare between studies because different modes of cold stresses and intensity of exercise are used.
In healthy subjects performing handgrip tests under cold conditions, AI has also been calculated from invasive blood pressure monitoring.33 AI was greater with cold and exercise compared with exercise alone, indicating greater LV work.33 ,82 If this occurs with impaired coronary perfusion, then it would follow that isometric exercise in the cold could precipitate ischaemia.33
Myocardial oxygen supply
As there is a further increase in myocardial oxygen demand with combination of exercise and cold, it would be expected that the myocardial oxygen supply would increase to meet this. PET studies have shown an overall increase in myocardial perfusion in response to exercising in the cold.42
CBF velocity was measured with transthoracic Doppler echocardiography in subjects performing handgrip tests at 30% of maximal voluntary contraction. While CBF velocity was shown to increase in response to exercise and cold, compared with exercise alone, the increase was attenuated,26 particularly in older subjects.104 Therefore, when comparing the relative changes in RPP and peak CBF velocity during the cold and grip protocol, the rise in RPP was greater than the rise in peak CBF velocity.26 ,104 This suggests that cold could be causing a relative mismatch in myocardial demand and supply during exercise even in healthy subjects.
The combined effect of dynamic exercise and cold on CBF has not been investigated in healthy subjects or subjects with CAD. Furthermore, no studies have invasively measured the effects of cold and exercise on coronary physiology, be it isometric or dynamic. Therefore, the question as to whether combined cold and exercise cause a true mismatch in myocardial supply and demand remains to be answered.
In subjects with CAD
Myocardial oxygen demand
Overall, the concept of a cold stimulus alone causing an excessive increase in myocardial work sufficient to provoke an AMI seems rather improbable. However, when a cold stimulus is combined with exercise, patients may be at risk of ischaemia at a much earlier stage in their regular exercise regimen due to excess myocardial work and insufficient myocardial oxygen supply. Indeed, subjects with CAD have reduced time to angina and reduced exercise tolerance102 ,105 ,106 under cold stress. SVR increases in exercise in the cold;102 RPP increases106–108 reflecting higher cardiac work due to increased afterload and HR.107
Myocardial ischaemia, identified by 1 mm ST depression on ECG, occurred earlier in subjects exercising in colder temperatures. Subjects were further classified as cold-tolerant and cold-intolerant according to whether they had a history of angina induced by cold. For cold-tolerant subjects, RPP at 1 mm ST depression did not vary according to the temperature in which exercise was undertaken. While for cold-intolerant patients the RPP at 1 mm ST depression was noted to be lower when exercising in colder temperatures.109 This implies that ischaemia is occurring at a lower MVO2, suggesting a greater mismatch of myocardial oxygen supply and demand when exercising in cold conditions.
Myocardial oxygen supply
Scintigraphic imaging has demonstrated increased exercise-induced myocardial perfusion abnormalities during cold in subjects with CAD.42 This was observed with no changes in maximal RPP, suggesting a direct influence on myocardial perfusion. PET imaging showed a similar disturbance of regional myocardial perfusion during exercise in the cold in subjects with CAD; however, these abnormalities occurred at RPP below the ischaemic threshold during exercise and, worryingly, many subjects did not experience symptoms.110
Conversely, cardiac vein thermodilution has been used to show a similar increase in cardiac vein flow in exercise in the cold compared with room temperature.108 It was demonstrated that exercise abolished the abnormal increase in CVR induced by cold alone when both stressors were applied simultaneously.108 However, in these experiments, exercise was performed; then after a period of rest, cold was applied, and following several minutes of this stress, exercise was resumed. It is unclear whether a warm-up effect could be contributing to these results.
The effect of exercising in the cold on myocardial oxygen supply depends on the atherosclerotic status of the coronary vasculature. In subjects with CAD, CBF fails to significantly increase in response to cold alone, resulting in a myocardial oxygen supply-demand mismatch.111 Moreover, in the presence of significant endothelial dysfunction, cold can precipitate coronary vasoconstriction.47 Intuitively it would follow that exercising in the cold would further increase the myocardial oxygen demand without sufficient increase in myocardial oxygen supply.
In conclusion, the likely mechanism by which cold increases angina in exercising subjects with CAD is through mechanisms that increase myocardial oxygen demand while blunting the metabolic adaptations that would ordinarily increase myocardial oxygen supply. These mechanisms are numerous, complex and interdependent as depicted in figure 8. However, the assumptions made about myocardial oxygen supply during exercise in the cold are all indirect as no invasive studies have been performed investigating coronary physiology.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Supply/demand mismatch in response to cold+exercise in normal and patients with CAD. In healthy subjects, the increase in myocardial oxygen demand to cold and exercise is matched by an increase in coronary blood supply. In subjects with CAD, the increase in myocardial oxygen demand is similar to healthy subjects in response to cold and exercise. However, a diminished increase in coronary blood supply may result in myocardial ischaemia. This is likely more pronounced in the presence of stenosis. CAD, coronary artery disease; CBF, coronary blood flow; HR, heart rate; MvO2, myocardial oxygen demand; MAP, mean arterial pressure; RPP, rate pressure product).
Cold tolerance
Not all subjects with CAD report susceptibility to cold-induced angina.43 ,109 ,112 Impaired baroreceptor responses, as measured by a >20 mm Hg decrease in SBP on standing, have been identified with greater frequency in the cold-intolerant group.112 Impaired baroreceptor function is associated with a steeper rise in HR and RPP, which increased MVO2 and lowered ischaemic threshold.112
The relevance of the distinction between self-reported cold-tolerant and cold-intolerant subjects highlights the importance of a patient-centred focus when advising subjects on their risks in the cold and ways to mitigate them. Although it may be that even in cold-tolerant subjects the compensatory baroreceptor-mediated attenuation in HR increase in response to cold could be overcome at extremely low temperatures.113
Limitations in comparing between cold studies
Many factors may explain the differing findings between cold studies, above and beyond the classification of subjects with CAD according to cold intolerance.112 Further differences between study protocols include differing degrees of coronary artery stenosis in the subjects, different cold stimuli, the extremes of temperature used, cardiovascular parameters measured and measuring techniques used. Moreover, the correlation between RPP and MVO230 in varying temperatures has not been formally assessed to ensure it remains an appropriate index of MVO2 in cold conditions. Contractility and wall tension, which also contribute to MVO2,9 are difficult to assess during exercise and may further contribute to inaccurate conclusions about MVO2 in cold and exercise.
Conclusion
The research performed to date suggests that cold increases myocardial work while blunting the physiological increase in MBF that should accompany exercise. This mismatch is aggravated in patients with a flow-limiting stenosis. Isometric exercise and cold stress both increase SVR, whereas dynamic exercise reduces SVR. The combination of cold and isometric exercise may therefore provide a particularly deleterious increase in afterload and myocardial work.
Clinical recommendations
While specific therapeutic interventions to counteract the effects of cold are unknown, it is still possible to provide some general recommendations.
In the first instance, exposure to cold can be limited by avoidance and dressing warmly including coverage of the face. Currently, cardiac rehabilitation programmes for patients with CAD recommend an increase in physical activity, which includes both dynamic and isometric exercise. However, patients who are carrying out this exercise in the cold may be taking an unnecessary risk, particularly with the isometric components of this rehabilitation programme. We recommend that patients should be advised that their exercise tolerance may be reduced, and risk of myocardial ischaemia increased, in cold weather. Furthermore, we recommend that patients undertake dynamic warm-up exercise indoors before cold exposure, particularly if performing partly isometric exercise.
Potential for therapeutic intervention
Medications that modify myocardial oxygen demand and improve myocardial oxygen supply should raise the ischaemic threshold and hence limit the deleterious effects of combined cold and exercise stress. Calcium channel blockers have been shown to prevent coronary vasoconstriction in subjects with CAD and improve exercise tolerance, and therefore may reduce cold-induced coronary vasoconstriction. Other coronary vasodilators such as nitroglycerin and nicorandil may have similar therapeutic effects.
Chronic sympathetic nervous system activation during the winter months may be partially responsible for plaque instability, although these data are currently only based on animal models. Should this be proven to be the case in humans, there may be a role for adrenoceptor antagonists during the winter months to prevent this adverse plaque remodelling. It is unclear whether selective β-adrenoceptor or non-selective α-adrenoceptors and β-adrenoceptors would offer more therapeutic effect.
Preferential prescription of all of these medications should be in the morning in order to achieve peak serum concentrations during the daytime when cold exposure is more likely.
You can get CPD/CME credits for Education in Heart
Education in Heart articles are accredited by both the UK Royal College of Physicians (London) and the European Board for Accreditation in Cardiology—you need to answer the accompanying multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://heart.bmj.com/misc/education.dtl
-
RCP credits: Log your activity in your CPD diary online (http://www.rcplondon.ac.uk/members/CPDdiary/index.asp)—pass mark is 80%.
-
EBAC credits: Print out and retain the BMJ Learning certificate once you have completed the MCQs—pass mark is 60%. EBAC/ EACCME Credits can now be converted to AMA PRA Category 1 CME Credits and are recognised by all National Accreditation Authorities in Europe (http://www.ebac-cme.org/newsite/?hit=men02).
Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into Heart with their journal's username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
Key messages
-
Cold temperatures are associated with worsening of angina symptoms and a higher incidence of acute myocardial infarctions.
-
Cold stress increases myocardial work but produces a relative reduction in coronary artery blood flow in patients with coronary artery disease.
-
When angina occurs during exercise, it is due to the increase in coronary blood flow being insufficient to meet the increased myocardial oxygen demand.
-
When a cold stimulus is combined with exercise, patients with coronary artery disease may be at risk of ischaemia at a much earlier stage in their regular exercise regimen.
-
Patients with coronary artery disease should be advised to limit exposure to cold and dress warmly including coverage of the face when exercising.
-
Patients with coronary artery disease should be advised that their exercise tolerance may be reduced and risk of myocardial ischaemia increased when exercising in cold weather.
References
Footnotes
-
Contributors VM-S, RPW and CDG were involved in the writing and initial critical review of the manuscript. MSM, SRR and TP were involved in subsequent critical review.
-
Funding British Heart Foundation Clinical Training Fellowship awarded to Dr Williams grant number FS/11/90/29087. National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy's and St Thomas’ National Health Service Foundation Trust and King's College London.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.