


A 53-year-old woman with a history of asthma, depression and moderate-to-heavy consumption of alcohol had presented to the emergency department with a three-month history of increasing fatigue and jaundice. She had reported consuming three or four beers on a regular basis and a few glasses of wine three times weekly. Over the past three months, she had been taking six prescription medications (Table 1)1–3 and seven natural health products (Table 2).4–12 Her bilirubin level had been elevated (281 [normal 3.4–22] μmol/L), as had her liver enzyme levels (alanine transaminase 755 [normal 8–56] U/L and alkaline phosphatase 273 [normal 42–98] U/L). An ultrasound of her abdomen had been consistent with cirrhosis, and the presumptive diagnosis had been cirrhotic liver disease. She had been advised to stop using alcohol and all of the natural health products.
Potential hepatotoxocity of prescription medications used by a 53-year-old woman who presented with jaundice and fatigue
Potential hepatotoxocity of natural health products used by a 53-year-old woman who presented with jaundice and fatigue
Despite taking this advice, the patient’s jaundice and fatigue worsened. She presented to the emergency department 12 days later, at which time she was admitted to hospital. Her physical exam showed asterixis, spider nevi and ascites, and she seemed mildly confused. A test showed that she was immune to hepatitis B. A blood test for hepatitis C was negative. Her levels of ceruloplasmin, α-1 antitrypsin, antimitochondrial antibodies, antinuclear antibody, and antismoothmuscle antibody were normal. Her immunoglobulin levels were elevated (immunoglobulin G 20.4 [normal 6.94–16.18] g/L, immunoglobulin A 6.11 [normal 0.70–4.00] g/L and immunoglobulin M 3.15 [normal 0.60–3.00] g/L). Her liver function tests remained abnormal (bilirubin 441 μmol/L, alanine transaminase 317 U/L and alkaline phosphatase 247 U/L), and a repeat ultrasound of her abdomen was still consistent with cirrhosis. There was no evidence of thrombosis in the hepatic or portal veins and no biliary dilatation. A transjugular biopsy of the liver showed submassive necrosis without the features of alcoholic hepatitis (Figure 1).

Biopsy from the central liver of a 53-year-old woman who presented with jaundice and fatigue. Areas of surviving hepatic parenchyma (arrow) and marked loss of hepatocytes can be seen. Hematoxylin and eosin stain, original magnification × 100.
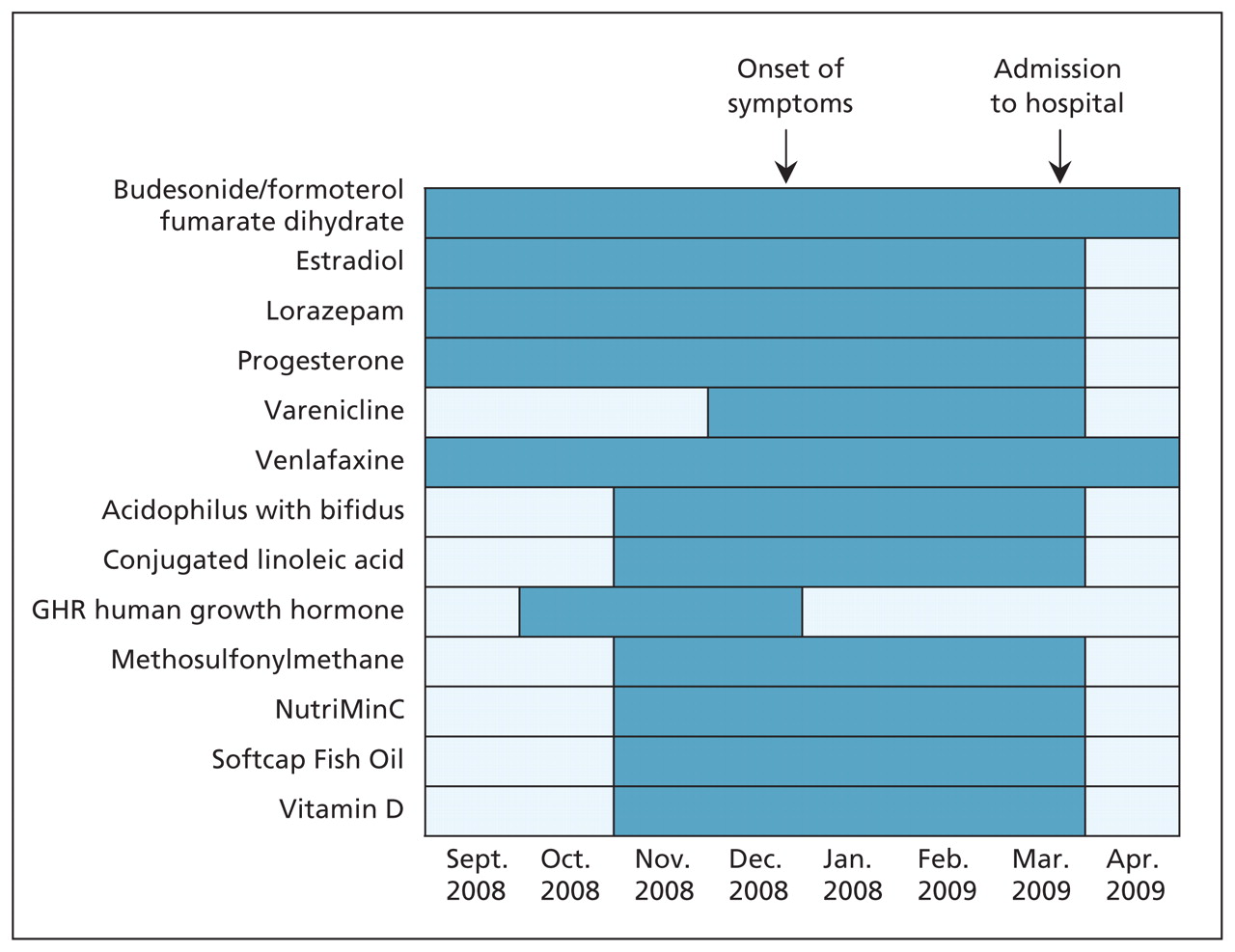
The differential diagnosis was submassive hepatic necrosis causing hepatic encephalopathy, due to either autoimmune hepatitis or drug toxicity. Liver injury as a result of alcohol use was considered unlikely because of the patient’s very high level of alanine transaminase and the results of the biopsy of her liver. A timeline showing the patient’s use of prescription and nonprescription medications is shown in Figure 2.

Timeline showing our patient’s exposure (shaded) to natural health products and prescription medications. The start of the patient’s adverse reaction and the point at which the patient was admitted to hospital are indicated.
The patient’s condition eventually improved with treatment that included diuretics, lactulose and prednisone, followed by azathioprine.
The case of this patient was evaluated through the multicentre Pharmacy Study of Natural Health Product Adverse Reactions (SONAR).13 We concluded that the entire combination of drugs, natural products and alcohol taken by our patient was possibly related to her hepatic symptoms. A single causative agent could not be isolated.
Discussion
It is important to determine potential adverse events that may be caused by medications, natural health products or illicit drugs, or combinations. Both passive and active surveillance can provide information on adverse reactions.
Passive surveillance usually requires health care professionals and patients to voluntarily report adverse events. Passive surveillance accounts for most of the postmarketing reporting of adverse events in Canada. The major drawbacks of passive surveillance are that meaningful estimates of incidence cannot be generated, the quality of reports tends to be low and it is well-known for underreporting.14 In contrast, active surveillance involves protocol-driven screening of risk groups, which in turn allows for more accurate estimates of incidence and the generation of reports that are more consistent and of a higher quality.4
This case demonstrates an example of active surveillance. This type of process can be used to assess potential adverse events caused by medications or natural health products. It also illustrates the considerable uncertainties in using case reports to determine potential adverse effects.
Step 1: Collection of information and review of adverse event databases
We completed a comprehensive review of the pubished literature (using the Medline and EMBASE search engines) on all prescription medications and natural health products used by the patient. Several of the natural health products have been associated with hepatotoxicity; however, much of the information about these associations is from studies done on animals or in vitro, and precise dosage information is limited.4–12,15 Both venlafaxine and varenicline have been reported to cause hepatotoxicity in patients, especially in those with underlying liver conditions.1–3 Tables 1 and 2 provide summaries of the patient’s medications and any published evidence of hepatotoxicity associated with their use.
Step 2: Analysis of medications
The harms associated with natural health products may be due to ingredients that are not listed on their labels (i.e., contaminants). Samples of all of the natural health products taken by our patient, with the exception of the human growth hormone product (GHR), which was no longer available in Canada, were tested for the possible presence of contaminants. Multiple samples of conjugated linoleic acid, methylsulfonylmethane, NutriMinC and Softcap Fish Oil were analyzed by gas chromatography/mass spectrometry and manually screened for steroids using ultraviolet light. None of the samples were found to contain adulterants or contaminants.
Step 3: Classifying probable adverse effects
Commonly used criteria for evaluating probable relationships between adverse events and the use of any product (or interactions between products) are summarized in Box 1.16,17 Adverse events that cannot be classified as probable can fall into one of the following three categories: possible; doubtful or unlikely; or unassessable or unclassifiable. A designation of unassessable or unclassifiable is usually due to a lack of information. Based on our review, we could not isolate a single causative agent. It is possible that it was the combination of medications, natural products and alcohol taken by our patient that led to her symptoms.
Criteria for evaluating adverse events
-
The Naranjo scale:16 A probable adverse reaction is indicated when there are previous reports of adverse reactions, when the onset of reaction is consistent with the time course of administration of the drug and when there is a positive response to withdrawal of the drug (dechallenge).
-
The Horn Drug Interaction Probability Scale (DIPS):17 A probable interaction is indicated when there are previous reports of interactions, when the reaction diminishes in a manner consistent with the time course of withdrawal of the drug, when there is a positive response to withdrawal of the drug (dechallenge) and when the interaction is consistent with the known pharmacology of the drug.
-
World Health Organization (WHO) criteria:16 A probable or likely adverse reaction is indicated if the clinical event occurs in a reasonable time frame after administration of the drug, if the event is unlikely to be due to concurrent disease and if the response to withdrawal of the drug (dechallenge) is clinically plausible.
Identifying possible adverse reactions
There are resources available to help physicians determine if a medication or natural health product is potentially causing an adverse reaction for a patient. Canada’s national passive surveillance system is MedEffect. Health Canada maintains a searchable Adverse Reaction Database accessible from the MedEffect homepage and regularly issues advisories, warnings and recalls using the information collected from voluntary reports of suspected adverse reactions (www.hc-sc.gc.ca/dhp-mps/medeff/index-eng.php). In the US, the Food and Drug Administration’s MedWatch provides a similar function (www.fda.gov/safety/MedWatch). (Additional resources for information on adverse events and natural health products are summarized in Box 2.)
Resources for information on adverse events and natural health products
-
Barnes J, Anderson LA, Phillipson JD. Herbal medicines. 3rd ed. London (UK): Pharmaceutical Press; 2007
-
Boon H, Smith M. 55 most common medicinal herbs. 2nd ed. Toronto (ON): Robert Rose; 2009
-
Canada Vigilance Program (via MedEffect)
-
European Medicines Agency
-
Evidence-based reviews of natural health products
-
General Information about natural health products
-
National Centre for Complementary and Alternative Medicine
-
Natural Health Products Directorate of Health Canada
www.hc-sc.gc.ca/ahc-asc/branch-dirgen/hpfb-dgpsa/nhpd-dpsn/index-eng.php
-
Natural health product/drug interaction tool
-
Natural Medicines Comprehensive Database (subscription required)
-
Natural Standard, The Authority on Integrative Medicine (subscription required)
-
Pediatric evidence on complementary and alternative medicine
As with other passive surveillance systems, MedEffect is subject to incomplete, inaccurate reporting and underreporting. For most reports of adverse effects, inferences regarding causality are not possible.
People often consider natural health products to be safe despite reported pharmacodynamic and pharmacokinetic interactions with conventional pharmaceuticals.18 This perception of safety may mean there are fewer reports of suspected adverse events related to natural health products than reports of adverse events related to conventional medications.17,19
Because many Canadians use natural health products (and one third of Canadians report using more than three products concurrently),20 it is prudent for physicians to ask about their use in the routine medical history and to consider potential interactions in a differential diagnosis when there is an unexpected response to treatment. Many natural health products may indeed be safe, and new Canadian regulations governing their labelling could help consumers be more well-informed when choosing treatments. Still, when these products are combined with multiple prescription and nonprescription medications, serious problems can occur and caution is warranted. Physicians can help improve knowledge about these products by reporting suspected adverse reactions to the Canada Vigilance Program via MedEffect.
Natural health products are not regulated in the same way as prescription drugs, and information on which natural health product/drug combinations are safe and which are potentially associated with adverse events remains largely unknown. Coordinated national surveillance initiatives will hopefully advance clinical knowledge in this poorly understood area.
Key points-
Natural health products such as herbs, vitamins and amino acids may interact with prescription drugs with potentially serious consequences, but establishing solid empirical links is challenging.
-
Clinicians should routinely ask patients whether they are taking any complementary or alternative medications.
Acknowledgements
All of the assays used were developed at the University of Alberta Hospital (Edmonton, Alta.). The SONAR team thanks the University of Alberta Department of Laboratory Medicine and Pathology, Division of Anatomic Pathology, for providing the biopsy image. The authors also thank Dr. Vincent Bain of the Division of Gastroenterology, Department of Medicine, University of Alberta, for his continuous and detailed input and review of this paper.
Footnotes
-
Competing interests: Dr. Sunita Vohra holds grant funding from the Canadian Institutes of Health Research, Health Canada and the Canadian Patient Safety Institute; she receives salary support as an Alberta Innovates — Health Solutions Health Scholar. No other competing interests were declared.
-
This article has been peer reviewed.
-
Contributors: Kosta Cvijovic wrote the paper and collected the data on which the paper is based. All of the authors contributed substantially to the article’s conception and design, played an important role in the interpretation and analysis of the data, revised the article and made significant contributions to it and approved the final version submitted for publication. Additional members of the SONAR group are listed in Appendix 1 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.091948/-/DC1).
References
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

