Widening participation in medicine
BMJ 2008; 336 doi: https://doi.org/10.1136/bmj.39508.606157.BE (Published 15 May 2008) Cite this as: BMJ 2008;336:1111
- Pamela B Garlick, senior lecturer in medical education and course director, extended medical degree programme1,
- Gavin Brown, lecturer in human geography2
- Correspondence to: P B Garlick pamela.garlick{at}kcl.ac.uk
- Accepted 29 January 2008
Today’s prevailing view is that tomorrow’s doctors should reflect the social and ethnic diversity of the countries in which they practise. To this end, initiatives to widen participation have been started in medical schools in several countries. Some of these initiatives include a commitment by students to return to their “area of origin” for a specified number of years after qualifying, but most have no such restrictions.1 Widening the participation of previously under-represented groups is not a straightforward process, as is highlighted by the Schwartz report.2 The widening participation initiative at the King’s College London School of Medicine began in 2001. Our remit was to enable bright students from low achieving state schools in inner London to become doctors. Students from the first cohort graduated in June 2007.
EMDP at King’s College London
In 2001, the first year of the extended medical degree programme (EMDP), 10 extra student places were allocated by the Higher Education Funding Council of England. Increases of 10 students a year were approved until the annual intake stabilised at 50.
The programme takes six years rather than five because the content of the first two years of the conventional course is spread over three years to produce gradually increasing workloads of 55%, 65%, and 80% of the conventional programme. EMDP students are integrated with the conventional students from the beginning, but in their extra available time they have tutorials in small groups (maximum of 12 students). The three predominantly clinical years are completed in the standard time.
Currently, the programme is supported by two full time academics; one part time administrator (0.5 full time equivalent); four part time academics (0.1 full time equivalent); and 15 postgraduates and academics, who provide about 130 small group tutorials per year. A conservative estimate for the total costs for this is £190 000 (€250 000; $380 000) a year.
Admissions process
It has been well documented that previous academic achievement—grades in A level examinations (taken at age 17-18), or grade point average—is a good, albeit imperfect, predictor of success at medical school, particularly in the early years.3 4 5 This can be valid only if the grades reflect the student’s true academic ability, which is not usually the case for applicants to any widening participation initiative. A detailed assessment of the candidate’s potential, together with their contextualised academic achievement, is therefore needed.6 7 Assessing potential is not easy because motivation, a key aspect, is hard to gauge and difficult to quantify.
To be eligible for the EMDP, candidates must have attended one of the 100 or so state schools or colleges in one of the 15 most educationally deprived boroughs in inner London. Almost all the eligible schools performed below the national average (in some cases as much as 70% below) in examination results in 2005-6, and only three or four students per year on our conventional medical course come from these schools.
The cognitive ability of each candidate is assessed by the mental agility test (MAT), a part of the personal qualities assessment test (PQA; www.pqa.net.au). Candidates with a sufficiently high MAT score are then invited for a 30 minute, semistructured interview. Although this is time consuming, because we routinely interview more than 150 applicants a year, we feel that this is essential for a fair assessment of these non-traditional applicants.
Successful students are offered a place on the course contingent on obtaining three C grades in their A level examinations. We accept applicants with lower grades if we think they will be successful on the course and places are available. As chemistry A level grades and MAT scores have a significant inverse correlation with having to leave the course, these are looked at carefully.
Socioeconomic status and ethnic origin
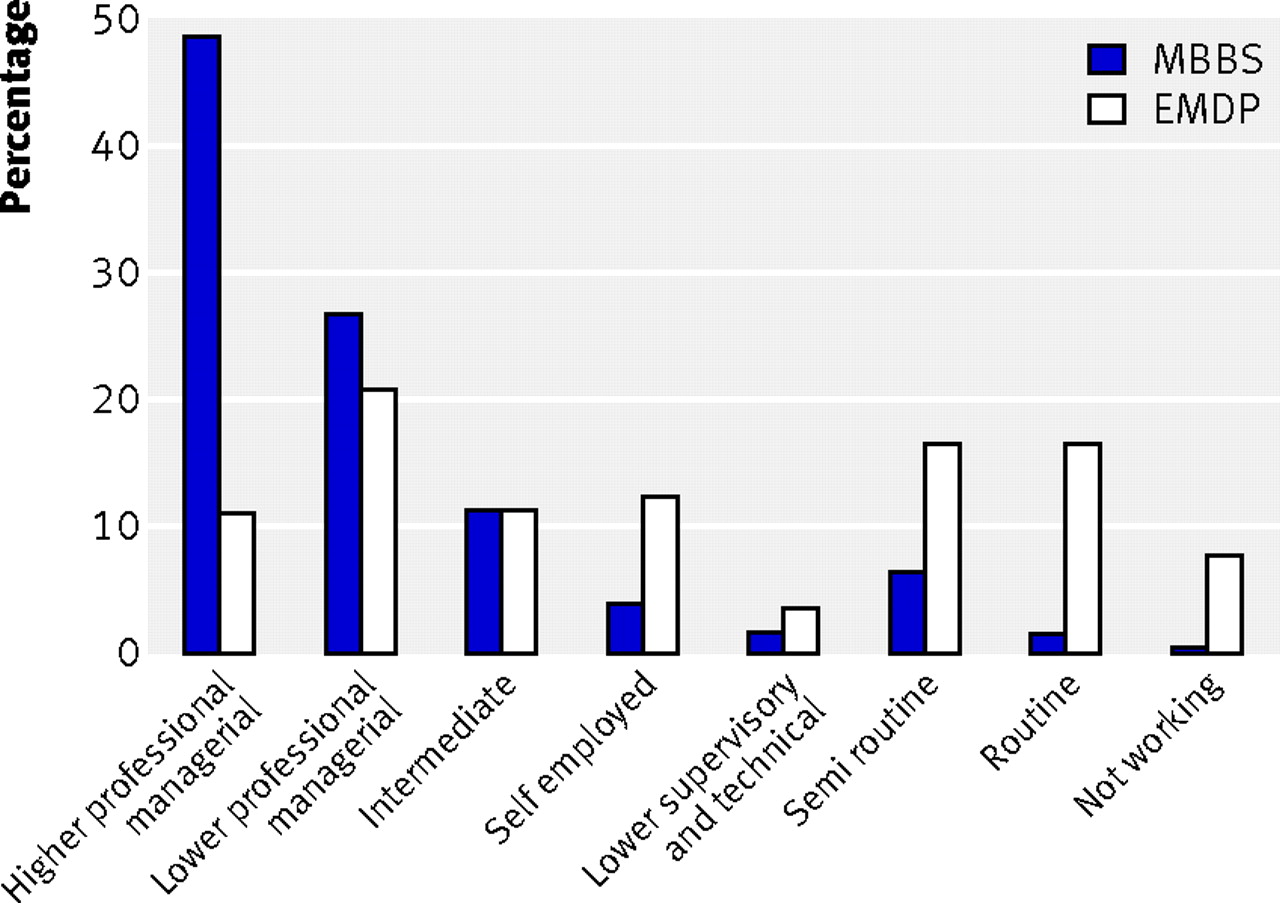
Three quarters of the medical students on our conventional course are from professional, middle class families (fig 1⇓). Only a third of EMDP students (58 students) fall into this group, with the remainder spread fairly evenly across the socioeconomic range. Many EMDP students who are from lower professional managerial groups have a Black African heritage and are from families headed by women. Their mothers tend to have embarked on higher education as mature students to enter professions such as nursing or social work. Many of the students classified as being from semiroutine and routine backgrounds are from South Asian families. Their mothers seldom work outside the home and their fathers work as cab drivers, kitchen porters, and machinists. Although generalisations like these should not be overinterpreted, they show the complex ways in which class and ethnicity are interlinked in contemporary society.

Fig 1 Socioeconomic classification of King’s College London medical students 2002-6
{kind=link}
In common with other London medical schools, the medical student population at King’s is more culturally diverse than might be expected from national figures. The ethnic mix of EMDP students is broadly representative of their age group in inner London: 91% of the EMDP students (173 students) are from minority ethnic communities, compared with half of the “conventional” students (fig 2⇓). EMDP students of Bangladeshi origin are predominantly from the London borough of Tower Hamlets, home to the largest Bangladeshi community in the UK; they are almost exclusively from working class families. EMDP students of Indian origin have a similar class profile to the Bangladeshis; this contrasts with their counterparts on the five year programme, who are mostly from professional middle class families. The large group of EMDP students classified as “other” ethnicity are predominantly of Arab and other Middle Eastern backgrounds, a group that is concentrated in some of our target boroughs.

Fig 2 Ethnic origin of the King’s College London medical students 2002-6
{kind=link}
White British and Black Caribbean groups remain under-represented among the EMDP students, with Black Caribbean students also under-represented on the conventional programme. Our research to understand this disparity suggests that fear of failure, expectations of class prejudice, and the lack of any value attached to the status of a doctor are the main reasons for not applying for medicine.8 Young people from both backgrounds aspire to gain modest financial security in the short term, without going via higher education.9 10
Curriculum
EMDP students arrive at medical school with very different cultural and social resources from their conventional peers; most of them are the first in their family to enter university, and they are often the first pupils from their schools to study medicine.11 Initially, many of them need a “safe” environment in which their individual needs and collective diversity can be respected. Our supportive features include an induction week, EMDP student mentors, dedicated rooms for studying and socialising, small group teaching sessions; personalised learning programmes, an annual prize giving ceremony, and (optional) informal discussions on cultural values and differences.
The induction week takes place while the campus is quiet, and we aim to establish an open exchange of opinions and respect for all views expressed. By the end of it, the EMDP students realise that we are interested in them as individuals and believe in their potential. We continue to foster this new self belief throughout the programme because we feel that it is key to enabling the students to succeed in what, for most, is initially an alien environment. The small group teaching sessions address scientific topics, as well as academic English, thinking skills, and presentation skills. A personal learning system provides each student with at least two one-to-one, 30 minute meetings a year with their EMDP adviser, when study skills and examination results are reviewed. The exams at the end of the first EMDP year are purely formative, so that all students have two years to adapt to medical school life before they can be asked to leave the course on grounds of academic failure.
One of the important changes in how the EMDP students are viewed (by themselves, other medical students, and less supportive members of faculty) occurred in the third year of the programme, when the EMDP cohort was 30, almost 10% of the entire medical year group. The students began “embedding from below”—they started opting to do intercalated BSc degrees, setting up new student societies, and being elected to the student medical education committee. They no longer felt that they were “different from” or “dumber than” the conventional students, and therefore were not perceived as such by others.
Student success and retention rates
The average A level grades of the EMDP students over the first years of entry were CCC, and in the past two years these have increased to BBC and BBB/C; the lowest grades of a student accepted onto the course were CDE. Despite these entry grades, their examination results are spread fairly evenly throughout the entire year group of 360-400 students. When EMDP students first sit identical papers to their conventional peers (at the end of their second year on the programme), 10% (five students) routinely gain merit awards for coming in the top 15% of the whole year group.
A level chemistry and biology grades (but not mathematics) of the EMDP students show significant correlation with marks in the first year examinations. This analysis is not possible for the conventional students because 96% of them have A grades in both chemistry and biology. We do not know whether it is the content of A level chemistry and biology or the conceptual understanding they confer that is most important.
The retention rate of students on the extended programme is 90% (135 out of the 150 who could have been asked to leave for failing summative exams), compared with 97% for students on the conventional programme. The overall graduation rate at universities across the UK in 2000 was 83%.12 First time pass rates in preclinical years are shown in table 1⇓. Interestingly, the average first time pass rates for the conventional and the EMDP students in the clinical years are identical at 93% (2205/2371 for the conventional students and 90/97 for the EMDP students) Attainment of students who opted to do intercalated BSc degrees is shown in table 2⇓.
Number (percentage) of medical students who passed preclinical exams at first sitting
Number (percentage) of students gaining intercalated BSc degrees
What the students say
“Becoming a doctor never seemed a possibility to me during secondary school. No matter how hard we worked, we were never encouraged to consider medicine. It is only since joining the EMDP that the support given to me has provided me with the confidence to perform at my best and reach my potential. Now I really believe that I can, and will, qualify as a doctor.”— Student in the second EMDP year
“Coming to university was a different experience as I had been brought up in a predominantly Bengali area and I had attended a single sex school and sixth form. Induction week was very helpful and enabled me to begin to gain different perspectives on ideas and beliefs that I held when I started.”— Student in the third EMDP year
“Studying medicine as an EMDP student, I did have initial worries regarding being labelled as “different” from the conventional medical students and being disadvantaged by this. However, I have recently become a Student Ambassador for the College and now ensure that I welcome new, potential EMDP students and reassure them that this is not the case.”— Student in the third EMDP year
“Not achieving AAB at A level meant that I still had doubts as to whether I was as good as the conventional students. Getting involved in extracurricular activities like SMEC [student medical education committee] reassured me of my own abilities and helped me realise that I could do anything I put my mind to. Being able to demonstrate that I am capable to others and myself has given me the self confidence to take on other challenges like doing a BSc.”— Student intercalating after the second clinical year
Conclusions
Students from our first cohort graduated in June 2007, and now almost 200 students are doing well in lower years of the programme. We can safely conclude that medical students can succeed without AAB at A level if these results were obtained from a low achieving school. Indeed, the highest achieving EMDP students excel in their exams. Some EMDP students, however, are hampered by uncertainty as to their place within higher education. These students need extra reassurance that their experience and beliefs are valued if they are to realise their potential. EMDP students bring different cultural assets and preconceptions about medical education to the college, and members of staff often comment that they are “fun to teach.” This is not to suggest that conventional medical students are not “fun to teach”, but to recognise that the differently “classed” expectations and assumptions that EMDP students hold can translate into behaviour in complex ways.13 14 EMDP students are often very enthusiastic, with a refreshing willingness to engage with staff in a polite but mildly irreverent manner, and show a well developed ability to “think outside the box.” As a result of this widening participation programme, a new type of doctor is being created that, among other things, better reflects the social diversity of London’s population.
Summary points
Medical students can succeed with CCC grades at A level if their results are achieved at a low achieving school or college
Extra academic and pastoral support is needed to enable these students to reach their full potential
Footnotes
Contributors: PG wrote the first draft of the paper and PG and GB then edited it. PG is guarantor.
Funding: None.
Competing interests: None declared.
Provenance and peer review: Not commissioned; peer reviewed.