Management of hypertension in pregnancy
BMJ 1999; 318 doi: https://doi.org/10.1136/bmj.318.7194.1332 (Published 15 May 1999) Cite this as: BMJ 1999;318:1332
- L A Magee, assistant professor (laura.magee{at}utoronto.ca)⇑,
- M P Ornstein, resident,
- P von Dadelszen, clinical fellow in maternal-fetal medicine.
- Correspondence to: Dr L A Magee, Department of Medicine, Mount Sinai Hospital, Toronto, Ontario, Canada M5G 1X5
- Accepted 12 March 1999
Hypertension in pregnancy is not a single entity1 but comprises:
Chronic hypertension, which complicates 1%-5% of pregnancies and is defined as a blood pressure greater than 140/90 mm Hg that either predates pregnancy or develops before 20 weeks of gestation
Pregnancy induced hypertension, which develops after 20 weeks of gestation and complicates 5%-10% of pregnancies
Gestational hypertension, which is pregnancy induced hypertension in isolation; it may reflect a familial predisposition to chronic hypertension, or it may be an early manifestation of pre-eclampsia
Pre-eclampsia, which is pregnancy induced hypertension in association with proteinuria or oedema, or both, and virtually any organ system may be affected.
Summary points
Antihypertensive treatment is well tolerated in pregnancy, with few women needing to change drugs due to side effects
Antihypertensive treatment for mild chronic hypertension benefits the mother, but the impact on perinatal outcomes is less clear, particularly for atenolol
For hypertension presenting later in pregnancy, even near term, the available data do not allow for reliable conclusions to be made about the benefits and risks of restricted activity with or without admission to hospital
Antihypertensive treatment for mild to moderate hypertension later in pregnancy benefits the mother, but the impact on perinatal outcomes may be harmful or beneficial
Women with early, severe pre-eclampsia have better perinatal outcomes if they are managed “expectantly,” but data are insufficient to estimate risks to the mother
For acute severe hypertension later in pregnancy, parenteral hydralazine is not the drug of choice as it is associated with more maternal and perinatal adverse effects than are other drugs, particularly intravenous labetalol or oral or sublingual nifedipine
Antihypertensive treatment given antenatally should probably be reordered postnatally
The types of hypertension in pregnancy differ primarily in the incidence, and not the nature, of maternal and perinatal complications. The UK confidential inquiries into maternal deaths has consistently shown an excess maternal mortality associated with hypertension in pregnancy due to intracerebral haemorrhage, eclampsia, or end organ dysfunction. Perinatal mortality and morbidity reflect both the fetal syndrome of pre-eclampsia (intrauterine growth restriction) and the consequences of iatrogenic prematurity resulting from deteriorating maternal disease or fetal condition.
Treatment aims to improve both maternal and perinatal outcomes. In this article we review randomised controlled trials of drug and non-drug treatments for hypertension in pregnancy.
Methods
We searched Medline (1966-97), Hypertension in Pregnancy (to 1997), bibliographies, and texts for articles in English or French that met several criteria (box). Data were abstracted independently by two reviewers who corroborated their findings. The most recent data were abstracted from duplicate publications.
Criteria for selection of articles
Randomised controlled trial
Drug or non-drug intervention (including bed rest and admission to hospital)
Hypertension in pregnancy
Clinical outcomes addressing maternal, perinatal, or paediatric benefit or risk: severe hypertension; additional antihypertensive treatment; pre-eclampsia; eclampsia; maternal mortality; caesarean section; placental abruption; change of drugs due to side effects; perinatal mortality; prematurity; small for gestational age infants; admission to special care baby unit; low Apgar scores; intraventricular haemorrhage; necrotising enterocolitis; respiratory distress syndrome; neonatal bradycardia, hypotension, or hypoglycaemia; jaundice; and long term neurodevelopment
Quantitative analysis was performed with the Cochrane Review Manager software (version 3.0.1) that uses the Peto odds ratio (95% confidence interval) as the summary statistic. Where it occurs, we describe differences in outcomes between trials that were greater than could be expected by chance alone. We qualitatively analysed the study design, participants, interventions, and outcome definitions.
For hypertension presenting later in pregnancy, most trials did not distinguish between pre-eclampsia, gestational, or chronic causes; therefore we classified participants as having hypertension that was either chronic or that developed later in pregnancy. Severity of hypertension was defined as mild (90-99 mm Hg), moderate (100-109 mm Hg), or severe (110 mm Hg) on the basis of diastolic blood pressure at enrolment. Most trials did not report how blood pressure was measured or whether Korotkoff phase IV or V was used.
Chronic hypertension
Seven trials enrolled 623 participants with mild chronic hypertension and compared antihypertensive treatment with no treatment. 2 3 Treatment aimed for a diastolic blood pressure less than 90 mm Hg.

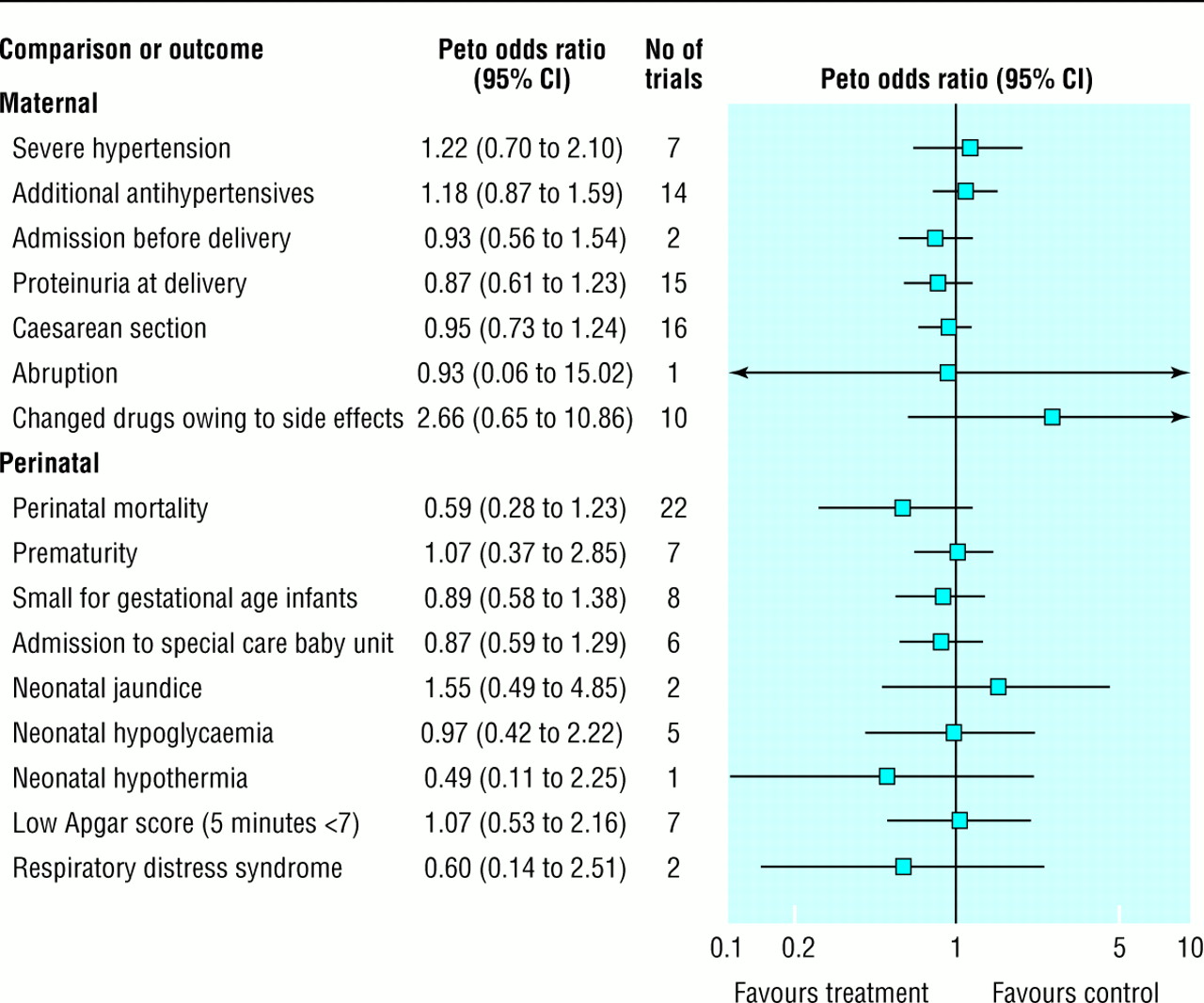
Summary odds ratios (95% confidence intervals) for antihypertensive treatment versus no treatment for mild chronic hypertension in pregnancy in seven trials
{kind=link}
Figure 1 shows that antihypertensives were more effective than no therapy in decreasing the incidence of severe hypertension (blood pressure greater than 160/100 mm Hg) and the requirement for additional antihypertensives. Methyldopa (500-3000 mg/day in 2-4 doses) and labetalol (200-1200 mg/day in 2-4 doses) have been used most commonly, although all antihypertensives seem to be equally effective. Decrease in admission to hospital before delivery was shown in only one trial,4 conducted in 1978 before the advent of obstetric day units. Although the decrease in proteinuria at delivery (a marker for pre-eclampsia) reaches borderline significance, definitions of proteinuria varied widely and trials were inconsistent, with the largest effect shown in the trial of ketanserin (a selective serotonin (5-HT2) receptor blocker with activity as an α1 blocker and inhibitor of platelet aggregation in vitro). Drugs were well tolerated, with only 3.1% (3/98) of women changing them because of side effects. No reliable conclusions can be drawn about other maternal outcomes.
Figure 1 also shows no effect of treatment on perinatal outcomes, but confidence intervals are wide, and are consistent with both benefit and risk. Trials were inconsistent in finding an impact of treatment on the incidence of small for gestational age infants; specifically, a small trial of atenolol versus placebo5 reported a dramatic increase in small for gestational age infants among the atenolol treated group (odds ratio 17.3, 95% confidence interval 3.8 to 77.9), a result that remains unexplained despite the trial's methodological problems.
Antihypertensive treatment for mild chronic hypertension benefits the mother. The impact on perinatal outcomes is less clear. If treatment is given then drugs other than atenolol may be preferable until further data are available.
Hypertension in later pregnancy
Non-drug approaches
Treatment guidelines have recommended use of non-pharmacological approaches for hypertension in later pregnancy, with or without antihypertensives, particularly for mildly increased blood pressure.6 Six trials enrolled 607 participants and compared ambulation out of hospital with bed rest in hospital 7 8 or ambulation with bed rest among women admitted to hospital with mild hypertension later in pregnancy. 9 10 No trials have enrolled women with moderate to severe hypertension. Figure 2 shows that there was no effect of restricted activity (with or without admission to hospital) on maternal or perinatal outcomes, although women managed as outpatients spent an average of 2.3 weeks (95% confidence interval 1.9 to 2.8) less in hospital.

Summary odds ratios (95% confidence intervals) for more versus less activity (ambulation with or without admission to hospital) in women with mild pregnancy induced hypertension in six trials
{kind=link}
No clinically important benefits were apparent in two small trials of psychosocial support11 (80 women) or biobehavioural training12 (45women). Data do not allow for reliable conclusions to be drawn about the benefits and risks of restricted activity with or without admission to hospital for mild hypertension later in pregnancy. Pending future data, antihypertensive treatment should not be delayed while recommending non-drug approaches. Data are needed on women with moderate to severe hypertension and those whose gestation is remote from term.

Summary odds ratios (95% confidence intervals) for antihypertensive treatment versus no treatment for mild to moderate hypertension presenting later in pregnancy in 15 trials
{kind=link}
Summary odds ratios (95% confidence intervals) for antihypertensives versus other antihypertensives (usually methyldopa) for mild to moderate hypertension presenting later in pregnancy in 23 trials
{kind=link}
Antihypertensive drug treatment
Fifteen trials enrolled 1926 participants and compared antihypertensives with no treatment for mild to moderate hypertension later in pregnancy. 1 13–16 The drugs used most commonly were methyldopa (two trials) and β blockers (eight), particularly labetalol (5/8). Treatment aimed for a diastolic blood pressure less than 90 mm Hg.
Figure 3 shows that antihypertensives decreased the incidence of severe hypertension, the need for additional antihypertensives, and the presence of proteinuria at delivery, regardless of drug or drug class. Again, the trials were conducted before the advent of obstetric day units, making the admission data difficult to interpret. In general, antihypertensives were well tolerated, with only 2.4% (11/455) of women changing drugs because of side effects. No reliable conclusions can be drawn about other maternal outcomes.
Figure 3 shows three perinatal effects worthy of comment: (a) respiratory distress syndrome was decreased without a concomitant change in prematurity; (b) more neonatal bradycardia was reported but only in trials of β blockers (bradycardia was detected only by close monitoring of neonatal heart rate and did not require intervention); and (c) there was a trend towards an increase in the incidence of small for gestational age infants. Although no adverse effects on neurodevelopment were shown, few children exposed in utero to either methyldopa17 (98 infants) or atenolol18-55 have been studied.
Clearly, antihypertensive treatment benefits the mother with mild to moderate hypertension later in pregnancy. No reliable conclusions, however, can be drawn about the overall impact of treatment on perinatal outcomes. The decrease in respiratory distress syndrome may be due to reporting bias. The increase in small for gestational age infants does not reach statistical significance.
If antihypertensive treatment is chosen, there is no clear choice of drugs. Figure 4 shows that the 23 trials19–29 (1349 participants) comparing one agent with another (usually methyldopa, 15 trials) showed no differences in maternal or perinatal outcomes; however, confidence intervals were wide, and clinically important effects have not been ruled out. By subgroup analysis, β blockers may be less effective antihypertensives than calcium channel blockers—that is, slow release verapamil or nicardipine (odds ratio for severe hypertension in three trials 2.52, 95% confidence interval 1.29to 1.52), however, this result must be interpreted cautiously as it rests on two trials with inadequate methods of randomisation.26
Severe hypertension presenting later inpregnancy
Aggressive versus expectant management
Mortality and morbidity related to prematurity remain significant problems if women with acute, severe hypertension (usually of pre-eclampsia) present before 34 weeks of gestation and are stabilised and delivered. Therefore, a more “expectant” approach has been advocated and tested in two trials 30 31 of 133 women. The average pregnancy prolongation was 2.0 weeks (95% confidence interval 1.4 to 2.6). Figure 5 shows that “aggressive” management compared with “expectant” management results in equivalent maternal morbidity, fewer small for gestational age infants, and more markers of serious neonatal morbidity. The trials, however, had low statistical power to rule out excess maternal morbidity (for example, HELLP (haemolysis, elevated liver enzymes, and low platelets) syndrome32) or mortality. The requisite close maternal and fetal surveillance may not be possible in all settings.

Summary odds ratios (95% confidence intervals) for “aggressive” versus “expectant” management of severe hypertension in women remote from term in two trials. HELLP=haemolysis, elevated liver enzymes, and low platelets
{kind=link}
Parenteral antihypertensive therapy
The 11 relevant trials with 570 participants 1 33–35 do not support recommendations favouring hydralazine.36 These trials compared intravenous hydralazine (5-10 mg bolus; infusion 3-10 mg/hour (maximum 15-80 mg/hour); or 20-40 mg intramuscularly) with other antihypertensives, most commonly intravenous labetalol (four trials; 10-20 mg boluses over 2 minutes, every 10 minutes as needed) or oral or sublingual nifedipine (four trials; 5-10mg orally, every 30 minutes as needed). Figure 6 shows that, compared with intravenous hydralazine, other agents were associated with less maternal hypotension, fewer caesarean sections, fewer placental abruptions, and fewer low Apgar scores; neonatal bradycardia was increased with labetalol, but only one of six affected neonates required treatment.

Summary odds ratios (95% confidence intervals) for parenteral antihypertensives versus hydralazine for severe hypertension presenting later in pregnancy in 11 trials
{kind=link}
A clinical advantage of nifedipine is that because it is given by mouth, midwifery staff may give it on an “as needed” basis (every 30 minutes) in the absence of a doctor. An interaction between nifedipine and magnesium sulphate has been reported to produce profound maternal muscle weakness37 as well as maternal hypotension and fetal distress,38 which have also been reported with other antihypertensive drugs including hydralazine.38 The magnitude of the risk is presumably small, given how commonly nifedipine and magnesium sulphate are used together; however, clinicians who prefer to use magnesium sulphate for prophylaxis against eclampsia may like to have other agents such as labetalol at their disposal.
Other approaches
The enthusiasm for plasma volume expansion comes from the observation that women with severe pre-eclampsia have reduced cardiac index and increased systematic vascular resistance, and that some of them respond to comparatively small doses of antihypertensives, with precipitous falls in blood pressure. Two small trials enrolled 42 participants in their third trimester, and described no serious maternal complications of plasma volume expansion when both a Swan-Ganz catheter and an arterial line were placed. The trials were not, however, large enough to rule out clinically important increases or decreases in maternal morbidity, and the treatment duration was insufficient to comment on perinatal outcomes. The safety and usefulness of plasma volume expansion must be further defined before it can be advocated for use outside the setting of a research project, unless women have a prolonged decrease in urine output or severe hypertension that responds to antihypertensives with hypotension.
Pre-eclampsia is associated with endothelial dysfunction, an excess of lipid peroxides and thromboxane: prostacyclin (PGI2) excess. Two small trials showed no effect on established pre-eclampsia with use of antioxidants39 (56 women) or PGI240 (compared with hydralazine, 47 women). These data are insufficient to allow any reliable conclusions to be drawn about treatment effectiveness.
Anaesthesia
The observed decline in maternal mortality has been credited, in part, to expanded anaesthetic resources devoted to obstetrics.41 Both regional and general anaesthesia are associated with risks: regional anaesthesia with fluid overload and hypotension, and general anaesthesia with aspiration of gastric contents. One trial randomised 80 women with severe pre-eclampsia to spinal-epidural, epidural, or general anaesthesia for caesarean section.42 General anaesthesia was associated with less maternal hypotension and crystalloid infused, but spinal-epidural anaesthesia (but not epidural) was associated with less frequent admission to a special care baby unit. The data are insufficient to allow reliable conclusions to be drawn about preference in women eligible for either route of anaesthesia. Clearly, some women are not candidates for regional anaesthesia because of falling platelet counts or a poor fetal cardiotocograph necessitating immediate delivery. One trial of 25 women with pre-eclampsia undergoing general anaesthesia found that intravenous labetalol given prophylactically attenuated the hypertensive (and tachycardic) response to intubation.43
Postpartum hypertension
Only three trials addressed the management of hypertension during the first 48 hours post partum. Women who took magnesium sulphate had an equivalent control of severe hypertension when they received oral nifedipine or placebo (30 women),44 and slightly better control of mild to moderate hypertension when given hydralazine intramuscularly compared with being given methyldopa intravenously (26 women).45 No trial data addressed whether or not antihypertensives should be restarted after delivery in women not taking magnesium sulphate, in whom methyldopa and timolol were equally effective antihypertensives (80 women).46
As blood pressure rises progressively over the first five postnatal days47 and commonly used antihypertensives are safe for breast feeding,48 pending future studies it would seem advisable to continue antihypertensive treatment after delivery, at least in women not taking magnesium sulphate. Traditionally, methyldopa has been avoided owing to depression and fatigue observed with long term treatment of non-pregnant patients, but such side effects may not be relevant over a shorter treatment interval. Although agents with short half lives (for example, labetalol) reach steady state drug levels more quickly than agents with longer half lives, clinicians are advised to use the agent with which they are most familiar. Women with pregnancy induced hypertension usually need antihypertensives for days to weeks.49
Footnotes
Competing interests None declared.