Type 1 diabetes and pregnancy
BMJ 2007; 334 doi: https://doi.org/10.1136/bmj.39154.700417.BE (Published 05 April 2007) Cite this as: BMJ 2007;334:742
- Roy Taylor, professor of medicine and metabolism, and honorary consultant physician1,
- John M Davison, consultant obstetrician, and emeritus professor of obstetric medicine2
- 1Newcastle University, and Royal Victoria Infirmary, Newcastle upon Tyne
- 2Royal Victoria Infirmary, and Newcastle University, Newcastle upon Tyne
- Correspondence to: R Taylor, Magnetic Resonance Centre, Newcastle General Hospital, Newcastle upon Tyne NE4 6BEroy.taylor{at}ncl.ac.uk
Pregnancy in women with type 1 diabetes remains a challenge for the patient and healthcare team alike. The scenario box on this page highlights some of the problems in achieving satisfactory pregnancy outcomes in women with diabetes. We discuss in the article the main areas of concern.
SCENARIO
Julie rang the diabetes specialist nurse having confirmed pregnancy with a home test kit. Her period was two weeks late. Although she recalled being advised about the need for prepregnancy care, she thought her glucose control was good enough (HbA1c concentration 7.9% at last check) and she had been taking a 400 µg tablet of folic acid daily. She had developed type 1 diabetes 16 years before (at age 8) and at her last annual review had no retinopathy or microalbuminuria. She controlled her diabetes with bedtime insulin glargine, plus insulin lispro (a rapid acting analogue) before meals.
An urgent appointment for the medical obstetric clinic was arranged, and telephone advice was given to achieve blood glucose levels of 3.5-5.5 mmol/l before meals and 4.0-6.5 mmol/l two hours after meals. HbA1c concentration decreased from 7.7% at presentation to 6.3% within eight weeks and was maintained around this level for the rest of pregnancy. The 19-20 week anomaly scan showed a cardiac abnormality, later confirmed with fetal echocardiography as a ventricular septal defect. Blood pressure increased from 102/66 mm Hg to 124/84 mm Hg. Labour was induced at 38 weeks. Blood glucose concentration was maintained at between 5.5 mmol/l and 7.3 mmol/l through use of intravenous glucose and insulin. After a normal vaginal delivery the 4100 g baby boy had Apgar scores of 7 and 9 at 1 and 5 minutes respectively. The locum neonatal senior house officer was advised by the experienced midwives not to measure blood glucose at birth, and when it was checked three hours after the first feed it was normal for age (2.8 mmol/l). Julie's baby remained with her on the ward. The paediatric cardiologist advised that no immediate cardiology intervention was required but follow-up was arranged. Julie was able to resume normal eating and subcutaneous insulin immediately after delivery.
Planning for pregnancy
The most important aim is to achieve the best possible glycaemic control before pregnancy. Over the past two decades intensive efforts to offer individual education about this have not resulted in higher prepregnancy counselling rates or even in presentation before the critical 42 day period of organogenesis.1 2 3w1 w2 The St Vincent declaration, a joint declaration by all European governments on preventing the problems of diabetes, outlined an aim of achieving similar outcomes of pregnancy in diabetic and non-diabetic women. This aim has not been met in most countries,2w3 although a “planned pregnancy” rate of 84% among diabetic women across the Netherlands has been reported.w4 A modest rise in planned pregnancy rates has been reported in one United Kingdom centre.4w5 An approach that raises awareness in the general population may be needed to promote further behaviour change in the UK.
For women with established diabetic nephropathy the chance of successful pregnancy diminishes sharply as serum creatinine increases (80% chance if 125-180 µmol/l; 75% chance if 180-220 µmol/l; and 60% chance if >220 µmol/l).w6 The higher the prepregnancy creatinine concentrations, the higher the risk of permanent loss of renal function. When albuminuria is established in a woman with type 1 diabetes, the implications for timing of pregnancy should be explained to her. Diabetic nephropathy will inevitably advance, and renal function will decline over a period of months or years. Once the creatinine concentration has increased, the chance of successful pregnancy decreases.
METHODS
In writing this review, we used published information from Medline searches, search of the Cochrane databases, and personal reference archives
How does pregnancy affect diabetes?
Control in type 1 diabetes is achieved by matching insulin dose with food intake and the changing insulin sensitivity. In early pregnancy, morning sickness may disrupt normal eating, and changes in timing or dose of insulin may be required; for women on a basal bolus-type regimen, this is relatively simple. Access to telephone advice from the diabetes team is important over this most critical phase of pregnancy.
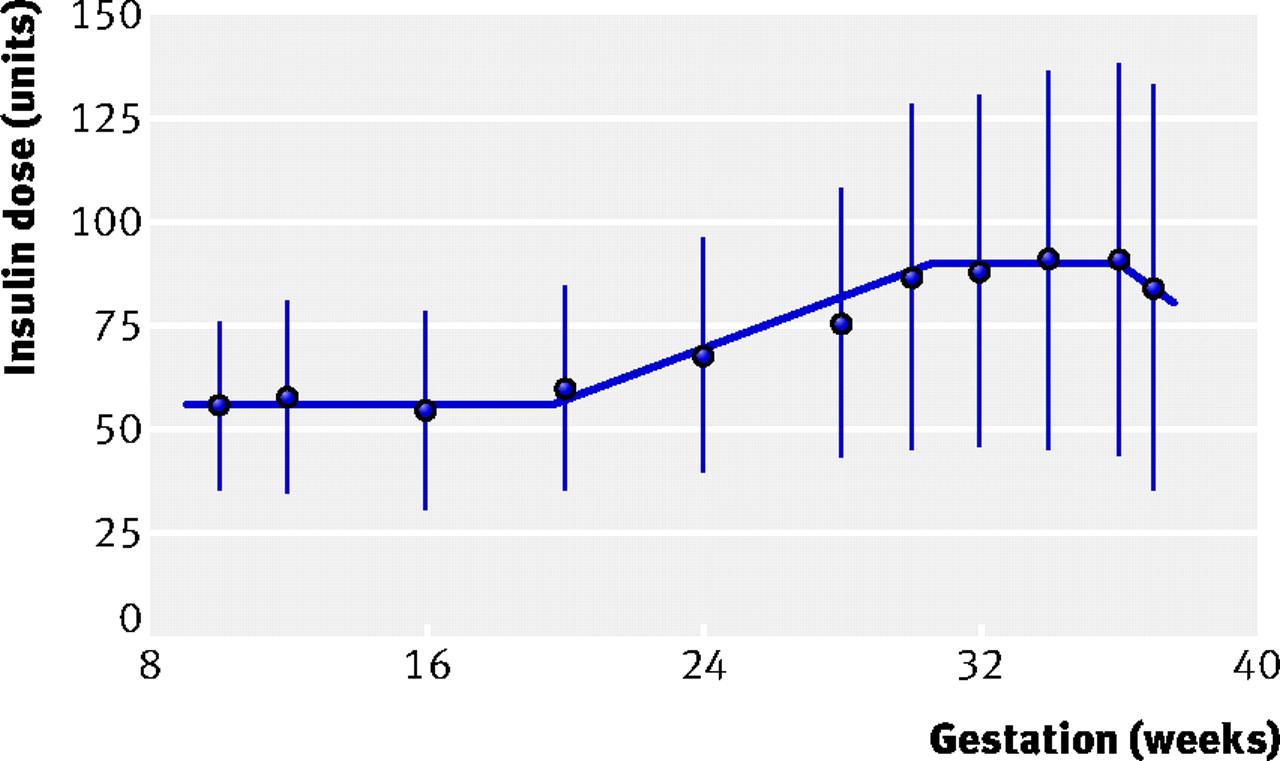
Insulin dose requirements change in pregnancy as a consequence of the physiological increase in insulin resistance. The extent of increase is determined by placental function and varies in successive pregnancies in any one woman. A five year, single centre, observational study has shown that the average increase in insulin requirement is 40%, with a wide range from no change to a higher than threefold increase.5 Figure 1⇓ shows the average time course of this change, which is helpful for advising what is to be expected from each clinic visit. Box 1 summarises the effects of pregnancy on diabetes.
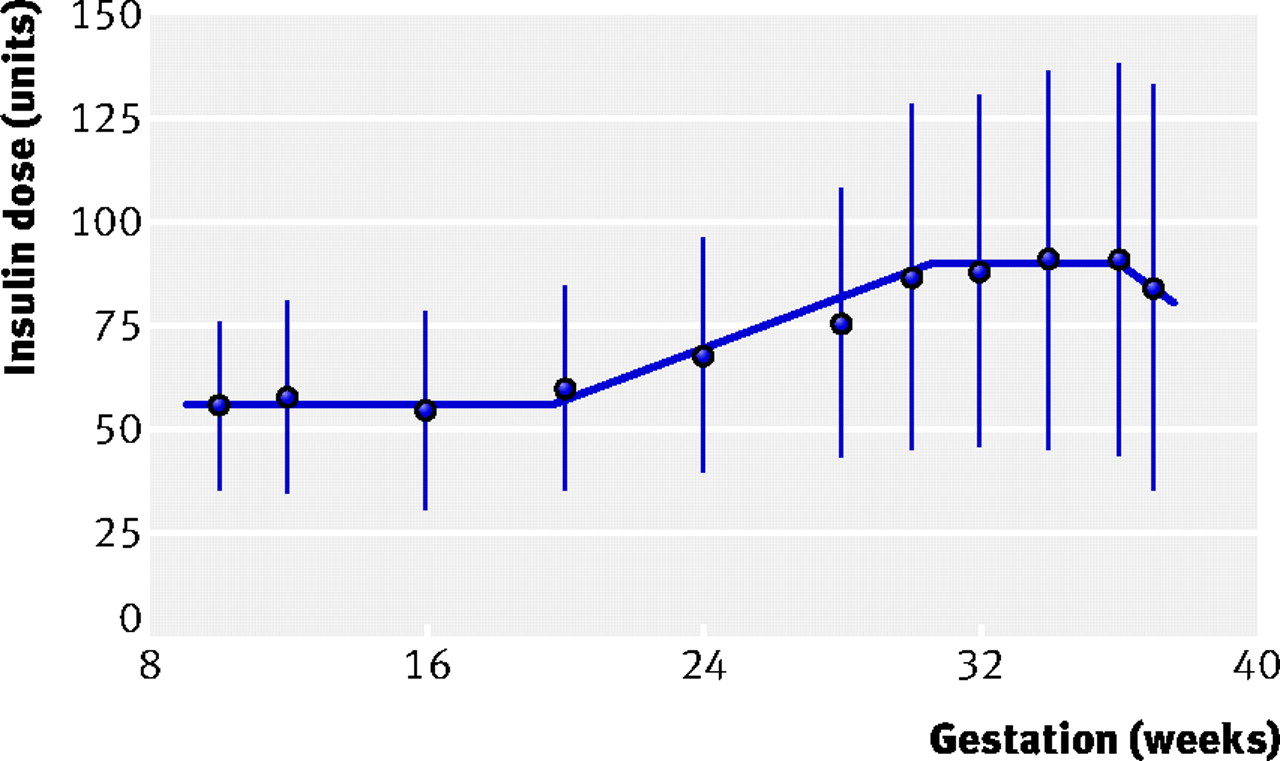
Fig 1 Data on 107 singleton pregnancies (showing means with standard deviations), from Taylor et al.5 Average insulin dose does not change until around 18 weeks' gestation and then increases steadily until around 28 weeks' gestation. The average fall in insulin dose of 5% between weeks 34 and 38 conceals wide individual variation
{kind=link}
Box 1: Effects of pregnancy on diabetes
• Change in eating pattern
• Increase in insulin dose requirements at 18-28 weeks' gestation
• Greater importance of tight glucose control (ideally HbA1c <6.1%)
• Increased risk of severe hypoglycaemia
• Risk of deterioration in pre-existing retinopathy
• Risk of deterioration of established nephropathy
• Lower renal threshold for glycosuria
One consequence of achieving near normoglycaemia is that asymptomatic hypoglycaemia will occur more frequently, and this will lead to unawareness of hypoglycaemia.w7 Women must be advised that they are at greater risk than usual of severe, unannounced hypoglycaemia and be specifically counselled about the importance of testing blood glucose concentrations before driving. Ideally a spouse or partner should be provided with a glucagon kit and trained in its use.
Retinopathy deteriorates whenever blood glucose control is suddenly tightened, as shown by several large randomised studies.6w8 In pregnancy, the extent of deterioration is strongly related to the degree of retinopathy present just before pregnancy. If retinopathy is not present on digital imaging according to the national standards for England,7 then it is highly unlikely that clinically significant change will occur during pregnancy.w9-w11 Rechecking at 28 weeks' gestation is all that is required. However, if moderate background changes are present, over half of women will develop proliferative retinopathy,w11 and full retinal screening is required at booking, 16-20 weeks, and 28 weeks.
If diabetic nephropathy is already established and serum creatinine is raised, there is an increased risk of permanent loss of renal function.w12
How does diabetes affect the pregnancy?
The most profound potential effect is the increased risk of congenital malformations. The recent UK Confidential Enquiry into Maternal and Child Health survey showed a threefold excess of cardiac and neural tube anomalies.8 Figure 2⇓ shows that very poor control of blood glucose leads to over 25% risk of malformation but that improved prepregnancy glucose control can decrease this almost to background levels.w13-w15 Even women with type 1 diabetes with normal HbA1c concentrations have intermittent, marked hyperglycaemia, and this may explain the difficulty of completely minimising the risk.w16 w17

Fig 2 The risk of all congenital malformations is increased above the background population rate of 2%, even in women with type 1 diabetes with normal HbA1c concentrations. The risk increases sharply with increasingly poor blood glucose control. Data from Rosenn et alw13
{kind=link}
Hyperglycaemia exerts its teratogenic effects during the period of organogenesis—the first 42 days of pregnancy—and pregnancy is invariably confirmed when much of this time has elapsed. This, together with delays in seeking advice from a nurse or doctor, means that frequently no effective advice to modify risk of congenital malformations can be given during the pregnancy. Diabetes confers a significant increase in risk of early spontaneous fetal loss, often as a consequence of non-viable, severe malformation.w13
Prepregnancy care from specialised multidisciplinary clinics, involving optimisation of blood glucose control and prescription of folic acid, could considerably decrease the observed rates of congenital malformation. Regrettably, however, even energetic local programmes have only modest impact at best,1 4 and data from countries round the world suggest that achieving change is very difficult.2 3w1 w18 Many patient information leaflets about pregnancy do not make clear the risks of pregnancy in diabetes. It is now routine practice to advise women to take 5 mg of folic acid daily before conception and for the first 12 weeks of pregnancy. No direct evidence supports this advice; the consensus to offer such advice w19 w20 was extrapolated from information that increased folic acid intake is more effective in preventing malformations in other conditions of high risk of neural tube defects.w21
Macrosomia (birth weight >4000 g) occurs in about a fifth of pregnancies in women with type 1 diabetes—twice the incidence for Englandw22—with the important corollary of an increased risk of birth injury to such babies. Shoulder dystocia occurs in about 8% of births to diabetic mothers (with risk of Erb's palsy), compared with 3% to the background population as shown by large, well conducted observational studies.2w4 Associated with macrosomia is the greater risk of more severe trauma to the mother, with potential future problems of poor pelvic floor function. Serial monitoring of fetal growth and size by ultrasonography is essential to allow judicious planning of delivery.
Delivery at about 38 weeks' gestation is advised for women with diabetes to minimise the risk of unexplained late fetal death. The timing and mode of delivery should be determined on an individual basis based on best possible assessments of risk to mother and baby. Macrosomia might also be a factor influencing timing of delivery, although little evidence supports this.w23 In recent published series, delivery before 37 weeks occurred in about a third of women with type 1 diabetes, with preterm caesarean section being the greatest single contributor.5 8w24
Pre-eclampsia is four times more likely to occur in women with type 1 diabetes than in women without diabetes,9 and even more likely in the presence of nephropathy (if albuminuria or microalbumuria has been established before pregnancy).w25 A large observational study has shown that poor blood glucose control before pregnancy does not in itself increase the likelihood of pre-eclampsia, although persistent poor control during pregnancy does increase the risk (odds ratio 1.65 for each 1% increase in HbA1c).w5
Box 2 summarises the effects of diabetes on pregnancy.
Box 2: Effects of diabetes on pregnancy
• Need for pregnancy planning
• Risk of congenital malformation
• Risk of macrosomia
• Need for regular clinical and ultrasound monitoring
• Increased risk of pre-eclampsia
• Increased risk of miscarriage and intrauterine death
How should drug treatment be managed?
The use of the recently introduced long acting insulin analogue glargine is one of the most important recent advances in diabetes management as it minimises the risk of hypoglycaemia despite tight control.10 Two case series totalling 174 individuals have shown no safety problems in pregnancy.w26 w27 Given that swings of blood glucose are known to be deleterious, any safety problems specific to glargine are outweighed by the beneficial effects on overall control. Like most insulins, glargine is not licensed specifically for use in pregnancy, and individuals must be advised about risks and benefits. There is no single insulin regimen that suits all in pregnancy.
If a patient is taking antihypertensive treatment such as an angiotensin converting enzyme inhibitor before pregnancy, then this should be tailed-off as soon as possible because of the risk of congenital malformations.w28 Methyldopa should be substituted providing that continuing treatment is required.
Treatment with high dose steroids may be required to mature the fetal lung if delivery is necessary before 34 weeks' gestation, for asthma, or for hyperemesis gravidarum. If treatment is indicated, the inevitable and predictable increase in insulin resistance requires a prospective increase in insulin dosage. In practice, an increase of 40% at the time of the first dose will prevent loss of control.w29 The increased dose of insulin is required until 24 hours after the last steroid dose. This will prevent the gross hyperglycaemia otherwise precipitated and is extremely unlikely to cause hypoglycaemia.
Management of mother and baby around delivery
The risk of neonatal hypoglycaemia is increased in the presence of maternal diabetes, as the maternal hyperglycaemia triggers excessive rates of insulin synthesis by the fetal pancreas. The risk does not correlate with HbA1c during pregnancy.1 5 However, controlling maternal blood glucose over the few hours before delivery is critical to minimise the risk of neonatal hypoglycaemia as blood glucose concentrations higher than 8 mmol/l will almost inevitably be associated with neonatal hypoglycaemia.5 Hence, maternal blood glucose concentrations of 4-8 mmol/l should be achieved using glucose and insulin infusion.1 As soon as the cord is cut, the rate of insulin infusion should be halved as insulin sensitivity returns to normal within minutes of shut-down of the uteroplacental circulation. Subcutaneous insulin administration can be resumed as soon as the mother is able to eat.
If the baby's blood glucose is checked as a routine precaution too early in life, then low concentrations are certain to be observed (5% of babies of non-diabetic women have a blood glucose concentration of less than 1.7 mmol/l within two hours of birthw30 w31). When faced with maternal diabetes, inexperienced staff tend to check the neonate's blood glucose, with the consequence that the baby will be unnecessarily admitted to a special care unit and the mother left alone on the ward after nine months of hard struggle with diabetes. To avoid this “empty arms syndrome” it is critical to promote early feeding, with a check of blood glucose only just before the second feed. This will decrease the current separation rate (one in three cases)—two thirds of separations are potentially avoidable. If hypoglycaemia is suspected, however, then glucose concentrations should be checked.
Conclusions
If Julie (see Scenario box) had contacted her diabetes team before going ahead with her plans to conceive and if blood glucose control had been optimised, the risk of congenital malformation would have been much reduced. Care from the combined obstetric and diabetes team during pregnancy indeed allowed early detection of problems. The induction of labour at 38 weeks avoided the potential risk of unexplained late fetal death. Good blood glucose control during labour minimised the chance of neonatal hypoglycaemia, and separation of mother and baby after delivery was avoided.
SUMMARY OF CLINICAL MANAGEMENT IN EACH TRIMESTER
First trimester
• Blood glucose control
• Folic acid 5 mg once daily
• Digital retinal screening
• Treat asymptomatic bacteriuria if present
Second trimester
• Blood glucose control
• Anomaly scan with tertiary centre assessment as needed
Third trimester
• Blood glucose control
• Serial ultrasound surveillance
• Digital retinal screening
• Discuss birth plan
• Plan for minimising risk of separation of mother and baby
• If steroids required, increase insulin dose by 40%
• Encourage breast feeding
Footnotes
This is one of a series of occasional articles about how to manage a pre-existing medical condition during pregnancy. If you would like to suggest a topic for this series please email Kirsten Patrick (kpatrick@bmj.com)
We thank Sally Marshall for discussion about this article.
Competing interests: None declared.
Provenance and peer review: Commissioned and peer reviewed.