CONSORT extension for reporting N-of-1 trials (CENT) 2015 Statement
BMJ 2015; 350 doi: https://doi.org/10.1136/bmj.h1738 (Published 14 May 2015) Cite this as: BMJ 2015;350:h1738
- Sunita Vohra, centennial professor1,
- Larissa Shamseer, PhD candidate and senior research associate2,
- Margaret Sampson, manager3,
- Cecilia Bukutu, associate director4,
- Christopher H Schmid, professor of biostatistics5,
- Robyn Tate, professorial research fellow6,
- Jane Nikles, NHMRC postdoctoral research fellow7,
- Deborah R Zucker, adjunct assistant professor8,
- Richard Kravitz, professor and co-vice chair of research9,
- Gordon Guyatt, professor10,
- Douglas G Altman, professor11,
- David Moher, senior scientist2
- and the CENT group
- 1University of Alberta, Canada
- 2Ottawa Hospital Research Institute, and University of Ottawa, Canada
- 3Library Services, Children’s Hospital of Eastern Ontario, Canada
- 4Alberta Centre for Child, Family and Community Research, Canada
- 5Center for Evidence Based Medicine, Brown University, USA
- 6Centre for Rehabilitation Research, Sydney Medical School - Northern, University of Sydney, Australia
- 7University of Queensland, Australia
- 8Tufts University School of Medicine, USA
- 9University of California, Davis, USA
- 10McMaster University, Canada
- 11Centre for Statistics in Medicine, University of Oxford, UK
- Correspondence to: S Vohra svohra{at}ualberta.ca
- Accepted 6 January 2015
Although randomised controlled trials are the ideal for establishing treatment efficacy, they have limitations.1 2 In particular, even the most rigorous and clearly reported randomised controlled trial cannot predict if a given intervention will be effective in a specific individual. For this reason, N-of-1 trials have been placed, by some, on the pinnacle of the evidence hierarchy for making decisions about treatment benefits and harms.3 4 They use key methodological elements of group clinical trials to evaluate treatment effectiveness in a single patient, for situations that cannot always accommodate large scale trials: rare diseases, comorbid conditions, or in patients using concurrent therapies.
N-of-1 trials have been used to evaluate a range of health conditions—including mental and behavioural disorders and diseases of the nervous, respiratory, circulatory, musculoskeletal, and digestive systems5—and are appropriate for a range of interventions, pharmacological or non-pharmacological, including complementary or alternative therapies. However, N-of-1 trials are not applicable for all health conditions or interventions. They are ideal for chronic stable conditions and for therapies with a relatively quick onset of action after initiation and quick termination of effect after discontinuation.
In an era that promotes patient centered research, comparative effectiveness, and personalised medicine, N-of-1 trials allow clinicians and patients to evaluate health interventions in a rigorous fashion and to re-evaluate chronic therapies to ensure therapeutic effectiveness is still achieved. N-of-1 trials are a unique tool to elicit patient preferences and to facilitate shared decision-making, hence evidence-based medicine, in real clinical practice. In addition, N-of-1 trials may also be used to assess causality of potential adverse effects. By reducing ineffective polypharmacy, N-of-1 trials may help promote patient safety.
N-of-1 methodology and reporting
N-of-1 trials provide a methodologically rigorous evaluation of treatment effectiveness in a single individual at a time, thereby helping to close the gap between evidence and practice. Unlike randomised controlled trials, which often exclude patients with comorbid conditions or concurrent therapies, N-of-1 trials allow a more flexible approach. Patients may be included as long as their health and concurrent therapies are stable during the period of evaluation; caution is necessary if combining results of N-of-1 trials because of heterogeneity between patients. As in group crossover trials, the potential for confounding by covariates is eliminated in N-of-1 trials given that each patient serves as his or her own control. The use of multiple crossovers in N-of-1 trials also increases confidence in the reliability of the results.
A recent systematic review of 100 trial reports indicates that the reporting of N-of-1 trials is largely inadequate.5 As an example, 79% of reports included in the review did not indicate which outcome was considered to be primary. Another 64% of reports did not comment on the presence or absence of adverse events. If N-of-1 trials are to be useful, these and other essential pieces of information must be included.
Among the first initiatives aiming to improve the completeness of reporting of research studies was the Consolidated Standards of Reporting Trials (CONSORT) guideline, which first emerged in 19966 and has been revised twice, most recently in 2010,7 8 to keep in line with evolving evidence and methodological standards for trials. Extensions to the main CONSORT document have been developed to address the reporting of variations in trial designs,9 10 11 interventions,12 13 14 and data.15 16 17 The CENT guideline provides a set of items, modified from the CONSORT 2010 guideline to facilitate complete reporting of N-of-1 trials. The development of CENT 2015 is in line with recent, international efforts to improve the reporting of research overall.18
For convenience, throughout this document, we refer to treatments and patients, although we recognise that not all interventions evaluated in N-of-1 trials are technically treatments and that participants are not always patients.
Terminology and scope of CENT
The single case experimental design, including N-of-1 trials, has a long history in the behavioural sciences.19 20 In the medical literature, the term “N-of-1 trial” is used to describe a prospectively planned, multiple crossover trial in a single individual—often challenge-withdrawal-challenge-withdrawal, also described as “ABAB”.20 CENT restricts itself to this use of the term “N-of-1”, rather than all possible single case experimental designs (fig 1⇓), for which a separate reporting guideline is under development.21 Consisting of repeated units of treatment comparisons (see box 1), N-of-1 trials may compare an active treatment against placebo, more than one active treatment, or perhaps multiple doses of a single treatment. The comparison depends on the question that is being asked. Definitions of methodological terminology specific to N-of-1 trials are provided in box 1.

Fig 1 Common single case designs. CENT is applicable to a subset of the “Withdrawal/reversal designs” category, which may or may not include the use of randomisation, designated by the red “N-of-1” box (adapted from 27)
{kind=link}
Box 1: Methodological terminology typical in N-of-1 trial reports
N-of-1 trial—An experimental clinical study design to determine the effect of an intervention in a single study participant. CENT is intended to be used to report repeated challenge-withdrawal (that is, “ABAB”) trials, commonly used in medicine, in which multiple crossovers between treatment(s) and control (placebo, standard care, alternate treatment) are continued for a pre-specified amount of time or until treatment effectiveness is determined. More than two treatment alternatives may be compared to each other or control (that is, “ABCABC”)
Period—The time during which a single treatment (A or B) is administered. Period length is typically determined a priori and may vary within a trial. The order of periods within a pair or treatment block may be randomised.
Block or pair—A repeated unit of a set number of period in N-of-1 trials is referred to as a block, in which the sequence of periods may or may not be randomised (for example, three repeating blocks of four periods may look like “AABB BBAA ABAB”). By convention, when the repeated unit contains only two periods (for example, three repeating pairs may look like “AB BA BA”), it is conventionally referred to as a pair.
Sequence—Multiple pairs or blocks comprise an entire sequence. The sequence is the consecutive set of periods, which may or may not indicate size of the repeated unit.
Washout period—A period in which no intervention is administered. A washout may be administered between different treatment periods or may act as a period in itself, as in a “reversal” design (to “wash out” the effects of a treatment before it is re-administered).
Run-in period—A pre-specified duration of time before a trial begins, during which trial treatments may be initiated (for example, to get to a stable therapeutic dose), to determine potential patient compliance with study regimens, or to allow for washout of a medication(s) a patient may have been taking before the trial.
Since approximately 60% of N-of-1 trial publications report on results from more than a single patient,5 the CENT reporting guidelines have been designed to facilitate the reporting of both a single N-of-1 trial or a prospectively planned series of multiple N-of-1 trials. Readers may also wish to use the checklist to facilitate the critical appraisal of published N-of-1 trial reports for completeness and transparency. This guidance is not intended to be applied by those reporting systematic reviews in which N-of-1 trials are included; future such guidance is planned.
Developing the CENT Statement
An international steering committee (DGA, Nick Barrowman, CB, GG, DM, JN, MS, RT, SV) comprising members with wide experience in clinical trial methodology and reporting guideline development, together with the project coordinator (LS), led the development of CENT. Two members of the team are practising physicians (SV and JN), and two others are members of the CONSORT and EQUATOR (Enhanced Quality and Transparency of Reporting) Network executive (DGA and DM). The EQUATOR Network is a group dedicated to “improving the reliability and value of medical research literature by promoting transparent and accurate reporting of research studies” (www.equator-network.org). The CENT Statement was developed in accordance with the process developed by members of EQUATOR executive group.22
Pre-meeting activities
In order to assess whether a reporting guideline for N-of-1 trials was indeed warranted, members of the CENT group (CB, MS, LS, SV) undertook a systematic review to assess the design and reporting of N-of-1 trials in the medical literature.5 This work confirmed the heterogeneity in N-of-1 trials, and large inadequacies in their reporting, as described above.
Between February 2009 and April 2009, a modified Delphi process was carried out to seek consensus on a set of potential reporting items (n=55) for N-of-1 trials. This initial list was developed based on the characteristics of published trials guided by our systematic review and reporting elements from the CONSORT 2010 checklist.7 A two-round survey was sent out to 56 international experts of N-of-1 trialists, biostatisticians, clinical epidemiologists, reporting guideline developers, biomedical journal editors, and health research funders, of whom 75% and 62% responded in rounds 1 and 2, respectively. Participants were asked to rank the importance of each potential checklist item on a 1 to 10 scale. After both rounds of surveying, items with a mean ranking of ≤5 were excluded from further consideration on the CENT checklist. Items ranking ≥6 or for which there was a large discrepancy between participants were carried forward for further discussion at the CENT consensus meeting.
CENT consensus meeting
In May 2009, a two day, in person meeting was convened in Banff, Canada, during which 23 experts in N-of-1 methodology, guideline development, N-of-1 study funders, and journal editors came together to further discuss and refine proposed checklist items. Discussion at the meeting yielded agreement on a set of essential concepts to be included in the guidelines; nuances of wording were not discussed at the meeting.
Post-meeting activities
After the CENT meeting, wording and organisation of concepts into checklist items was carried out and refined within the steering group and approved by meeting participants. A second round of circulation solicited feedback from those invited to the meeting but unable to attend. A flow diagram subcommittee was formed (NBG, JN, DRZ) to lead development of the CENT flow diagrams.
CENT 2015 checklist
The final CENT 2015 checklist is an extension of 14 items of the 25 CONSORT 2010 (table 1⇓) and contains a total of 44 sub-items, some of which are modifications of a standard CONSORT 2010 item and some of which are in addition. For item 1b, pertaining to the abstract, recommendations specific for N-of-1 trials are proposed in table 2⇓. Since N-of-1 trials may be conducted for an individual or a series of individuals, where pertinent, the checklist indicates specific items where different or additional information is required for series of N-of-1 trials. The recommendations within CENT may require more words or space than N-of-1 trialists are accustomed to. Providing detailed descriptions for some trials will facilitate transparency and future reproducibility, in line with emerging journal policies aimed at facilitating reproducibility.23
CENT 2015 checklist*; CONSORT 2010 checklist items with modifications or additions for individual or series of N-of-1 trials; empty items in the CENT 2015 column indicate no modification from the CONSORT 2010 item
CENT abstract considerations (modifications or additions to CONSORT Statement for Abstracts)
We recognise that improved reporting must be balanced against patient confidentiality in situations when the condition is rare. Authors must be mindful of this, and if there is any doubt as to whether complete reporting could be identifying, they should seek consultation with their institutional ethics board. This issue is of heightened importance in N-of-1 trials of rare conditions or when the potential societal stigma is high. Caution should be taken when reporting a combination of identifying information pertaining to CENT items 4a, 4b, 14a, and 15.
CENT diagrams
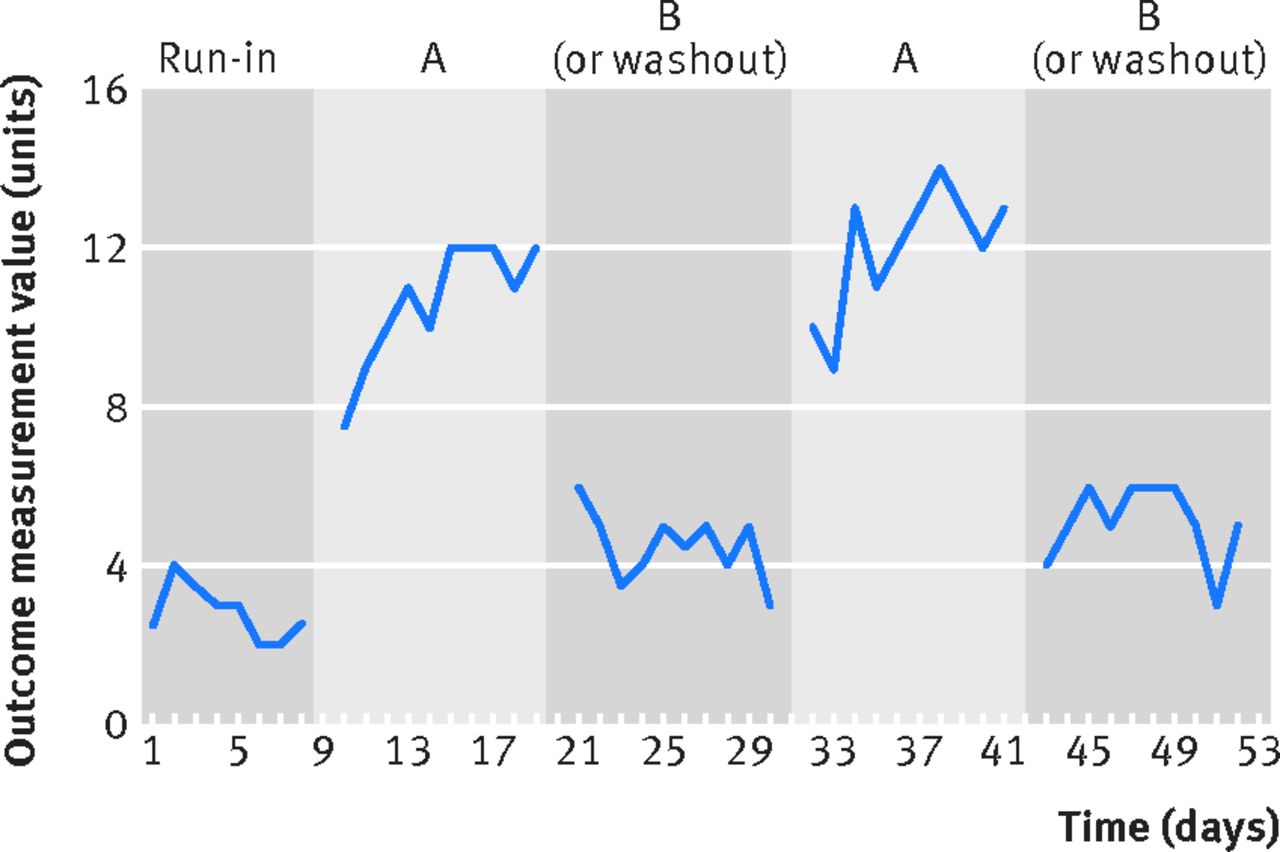
Diagrams have been developed to help authors visually depict both an individual participant’s progress through an N-of-1 trial (fig 2⇓, CENT trial pictorial) and the flow of multiple participants through a series of trials (fig 3⇓, CENT flow diagram). Authors are encouraged in include the relevant diagram(s) in their N-of-1 reports. Specific guidance on the information that should be included in each diagram is provided in the CENT Explanation and Elaboration document.24

Fig 2 N-of-1 trial pictorial; suggested visual representation of data from an individual N-of-1 trial
{kind=link}

Fig 3 CENT flow diagram; suggested representation of the flow of participants in a series of N-of-1 trials
{kind=link}
CENT 2015 Explanation and Elaboration (E&E) document
Once the CENT checklist was drafted, the steering committee and members from the larger CENT group prepared a rationale and examples of good reporting for the final set of checklist items. These can be found in the CENT 2015 Explanation and Elaboration (E&E) document.24 The principles addressed in this document were largely derived from existing literature, the CONSORT 2010 E&E document8 where applicable, and from discussions at the CENT meeting, which was recorded and summarised.
We strongly recommend that authors preparing N-of-1 trial reports and those charged with reviewing them use the CENT 2015 checklist to guide or assess their reporting. Authors are urged to read and use the CENT 2015 E&E document together with the checklist, as it provides examples of good reporting and evidence and consensus based rationale and guidance on how to report each item.24
Post-publication activities
Post-publication activities are planned around CENT 2015, including collecting feedback from the broader scientific community on the CENT initiative and specific checklist items. We also plan to seek endorsement from medical journals known to publish N-of-1 trials (see below). The CENT 2015 Checklist, Statement, and E&E documents are available through the CONSORT website (www.consort-statement.org) and accessible through the Enhancing the Quality and Transparency of Health Research (EQUATOR) Network library of reporting guidelines (http://www.equator-network.org/resource-centre/library-of-health-research-reporting/).
Endorsement
The CONSORT Statement is likely the best known reporting guideline. It has been well received by several scientific organisations (including the International Committee of Medical Journal Editors, Committee on Publication Ethics, and World Association of Medical Editors) and many biomedical journals, over 600 of which currently endorse CONSORT. Endorsement is typically demonstrated by way of an editorial statement in a journal’s “Instructions to authors” section, supporting the use of one or more reporting guidelines. Following this model, we plan to seek endorsement from journals that publish N-of-1 trials and work with these journals to ensure author adherence to reporting CENT 2015 items. To help journals ensure optimal use of the CENT 2015 by authors, we propose the following wording:
“[This journal] requires a completed CENT 2015 checklist as a condition of submission of reports of individual N-of-1 trials or a series of N-of-1 trials. We recommend that, while completing this form, you consider amending your manuscript to ensure your article, at a minimum, addresses each item listed on the CENT 2015 checklist. Taking the time to ensure your manuscript meets these basic reporting requirements will greatly improve your manuscript, potentially enhancing its chances for eventual publication.”
Registering N-of-1 trials
N-of-1 trials can be prospectively registered in existing trial registries (albeit with some modifications). Eventually, we plan to work with clinicaltrials.gov and all of the primary registries within the WHO Registry Network (www.who.int/ictrp/network/primary/en/index.html), in accordance with the International Clinical Trials Registry Platform, to enable a broader audience to more easily register their N-of-1 trials. This will help to increase the transparency of N-of-1 trial reporting and facilitate appraisal of trial reports for potential biases (selective reporting). Although it is possible to register N-of-1 trials in existing registries few published N-of-1 trials have been registered or indicate being registered in their published report.
Evaluation
As with other reporting guidelines, the impact of CENT can be evaluated by comparing the completeness of reporting of checklist items between N-of-1 trial reports published in journals endorsing and not endorsing the CENT checklist as well as before versus after endorsement in endorsing journals. This approach reflects methods previously used to evaluate CONSORT and other reporting guidelines.25 26
Conclusions
N-of-1 trials offer a pragmatic approach to evidence based clinical practice. Rather than forcing patients into an all or none fit with a rigid parallel group-based trial protocol, N-of-1 trials can be flexible and adapt around the individual to help assess treatment effectiveness under real world circumstances. They facilitate shared decision making between patients and practitioners, thereby bringing evidence based medicine into real clinical practice. While N-of-1 trials can be flexible enough for clinical use, they can also be standardised for the purpose of research, which may allow outcomes to be combined for population estimates. By improving the clarity of N-of-1 trial reporting, the CENT 2015 guidelines offer an opportunity to improve the interpretation and usefulness of N-of-1 trials.
The CENT 2015 guideline is primarily intended to be used by authors and reviewers who report and assess N-of-1 trials, respectively. It may also be helpful earlier in the research process as researchers design protocols for N-of-1 trials.
Notes
Cite this as: BMJ 2015;350:h1738
Footnotes
We thank Kris Cramer for her early work on developing the scope and helping to acquire funding support for this project.
Members of the CENT Group (listed alphabetically):
Douglas G Altman, professor, Centre for Statistics in Medicine, University of Oxford, UK; Cecilia Bukutu, associate director, Child and Youth Data Laboratory, Alberta Centre for Child, Family and Community Research, Canada; Jocalyn Clark, executive editor, icddr,b, Bangladesh; Elise Cogo, research consultant, Canada; Nicole B Gabler, biostatistician, Center for Clinical Epidemiology and Biostatistics Perelman School of Medicine, University of Pennsylvania, USA; Gordon Guyatt, professor, Department of Clinical Epidemiology & Biostatistics, McMaster University, Canada; Richard Kravitz, professor and co-vice chair of research, Department of Internal Medicine, University of California, Davis, USA; Janine Janosky, vice provost for research, Central Michigan University, USA; Bradley C Johnston, assistant professor, Department of Anesthesia and Pain Medicine, The Hospital for Sick Children, University of Toronto, Canada, and Institute of Health Policy, Management and Evaluation, Dalla Lana School of Public Health, University of Toronto, Canada; Bob Li, scientific advisor (retired), Office of Science, Therapeutic Products Directorate, Health Canada, Canada; Jeff Mahon, professor, Medicine and Epidemiology and Biostatistics, University of Western Ontario, Canada; Robin Marles, senior scientific advisor, Bureau of Nutritional Sciences, Food Directorate, Health Canada, Canada; David Moher, senior scientist, Clinical Epidemiology Program, Ottawa Hospital Research Institute ; University of Ottawa, Canada; Jane Nikles, NHMRC postdoctoral research fellow, University of Queensland, Australia; Margaret Sampson, manager, Library Services, Children’s Hospital of Eastern Ontario, Canada; Christopher H Schmid, professor of biostatistics, Department of Biostatistics and Center for Evidence Based Medicine, Brown University, USA; William R Shadish, professor, University of California, Merced, USA; Larissa Shamseer, senior research associate, Clinical Epidemiology Program, Ottawa Hospital Research Institute; University of Ottawa, Canada; Robyn Tate, professorial research fellow, Centre for Rehabilitation Research, Sydney Medical School - Northern, University of Sydney, Australia; Sunita Vohra, centennial professor, Department of Pediatrics, Faculty of Medicine and Dentistry, University of Alberta, Canada; Deborah Zucker, adjunct assistant professor, Tufts University School of Medicine, USA.
Contributors: SV, LS, MS, DGA, and DM conceived of this paper. SV and LS drafted the article and all authors critically revised it for important intellectual content. All authors approved the final version of this article. SV is the guarantor of this work.
Competing interests: All authors have completed the ICMJE uniform disclosure form and declare: the development of CENT was funded by Alberta Advanced Education and Technology, Alberta Heritage Foundation for Medical Research (now Alberta Innovates - Health Solutions (AHIS)), Boiron, CV Technologies (now Afexa Life Sciences), Hecht Foundation, HEEL, Pfizer USA, Schwabe Pharma, and in part, through operational funding awarded by the Canadian Institutes for Health Research (Reference No 86766); no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; representatives from industry partners were present and participated at the CENT consensus meeting and were offered the opportunity to provide input on this manuscript, which none did. SV receives salary support from AHIS as a health scholar.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/