Diarrhoea and vomiting caused by gastroenteritis in children under 5 years: summary of NICE guidance
BMJ 2009; 338 doi: https://doi.org/10.1136/bmj.b1350 (Published 22 April 2009) Cite this as: BMJ 2009;338:b1350
- Rajesh Khanna, senior research fellow 1,
- Monica Lakhanpaul, clinical codirector 1, senior lecturer in child health 2,
- Shona Burman-Roy, research fellow1,
- M Stephen Murphy, consultant paediatric gastroenterologist and senior lecturer in paediatrics and child health 3
- on behalf of the Guideline Development Group and the technical team
- 1National Collaborating Centre for Women’s and Children’s Health, London W1T 2QA
- 2University of Leicester, Leicester LE1 9NH
- 3Birmingham Children’s Hospital NHS Foundation Trust and University of Birmingham, Birmingham B4 6NH
- Correspondence to: M S Murphy M.S.MURPHY{at}bham.ac.uk
Why read this summary?
Gastroenteritis is common, with many children having more than one episode a year. The characteristic symptoms—sudden onset of diarrhoea with or without vomiting—are unpleasant and affect both the child and family or carers. Although the illness usually resolves without treatment and can be managed in the community, many children are admitted to hospital each year.1 2 In the absence of national guidance, clinical practice is thought to vary considerably across the United Kingdom, with a major effect on the use of healthcare resources.3 This article summarises the most recent recommendations from the National Institute for Health and Clinical Excellence (NICE) on the diagnosis, assessment, and management of diarrhoea and vomiting caused by gastroenteritis in children under 5 years.4
Recommendations
NICE recommendations are based on systematic reviews of best available evidence. When minimal evidence is available, recommendations are based on the Guideline Development Group’s opinion of what constitutes good practice. Evidence levels for the recommendations are given in italics in square brackets.
Diagnosis
Clinical diagnosis
Suspect gastroenteritis if stools suddenly change to a loose or watery consistency or onset of vomiting occurs suddenly (or both). In suspected cases, ask about recent contact with someone with acute diarrhoea or vomiting (or both), exposure to a known source of enteric infection (possibly contaminated water or food), and recent travel abroad. Notify and act on the advice of the public health authorities if you suspect an outbreak of gastroenteritis.
Any of the features given below are possible indicators of diagnoses other than gastroenteritis:
-Fever:
Temperature of 38°C or higher in children under 3 months
Temperature of 39°C or higher in children aged 3 months or more.
-Shortness of breath or tachypnoea
-Altered state of consciousness
-Neck stiffness
-Bulging fontanelle in infants
-Non-blanching rash
-Blood or mucous in stool
-Bilious (green) vomit
-Severe or localised abdominal pain
-Abdominal distension or rebound tenderness.
[All recommendations based on moderate quality observational studies and the experience and opinion of the Guideline Development Group (GDG)]
Laboratory investigations
Microbiological investigation of stools:
-Consider this if the child has recently been abroad, diarrhoea has not improved by day seven, or the diagnosis of gastroenteritis is uncertain
-Perform this if you suspect septicaemia, if blood or mucous is present in the stool, or the child is immunocompromised.
Blood culture:
-Perform this if you are planning to give antibiotics.
Monitoring for haemolytic uraemic syndrome:
-Seek specialist advice on monitoring for this syndrome in children with Escherichia coli O157:H7 infection.
[All recommendations based on moderate quality observational studies and the experience and opinion of the GDG]
Assessing dehydration and shock
Clinical assessment
The following children are at increased risk of dehydration:
-Children under 1 year, particularly those younger than 6 months
-Infants whose birth weight was low
-Children who have passed more than five diarrhoeal stools in the previous 24 hours
-Children who have vomited more than twice in the previous 24 hours
-Children who have not been offered or have not been able to tolerate supplementary fluids before presentation
-Infants who have stopped breast feeding during the illness
-Children with signs of malnutrition.
Use fig 1⇓ to detect clinical dehydration and shock after taking into account the risk factors for dehydration.

Fig 1 Symptoms and signs of clinical dehydration and shock
{kind=link}
Suspect hypernatraemic dehydration if any of the following are present:
-Jittery movements
-Increased muscle tone
-Hyper-reflexia
-Convulsions
-Drowsiness or coma.
[All recommendations based on moderate to high quality observational studies and the experience and opinion of the GDG]
Laboratory investigations
Do not routinely perform blood biochemical testing.
Measure plasma sodium, potassium, urea, creatinine, and glucose concentrations if intravenous fluids are needed or clinical features suggest hypernatraemia.
[All recommendations based on the experience and opinion of the GDG and low quality observational studies]
Fluid management
Use the flow chart (fig 2⇓) to help in the fluid management of a child with gastroenteritis.
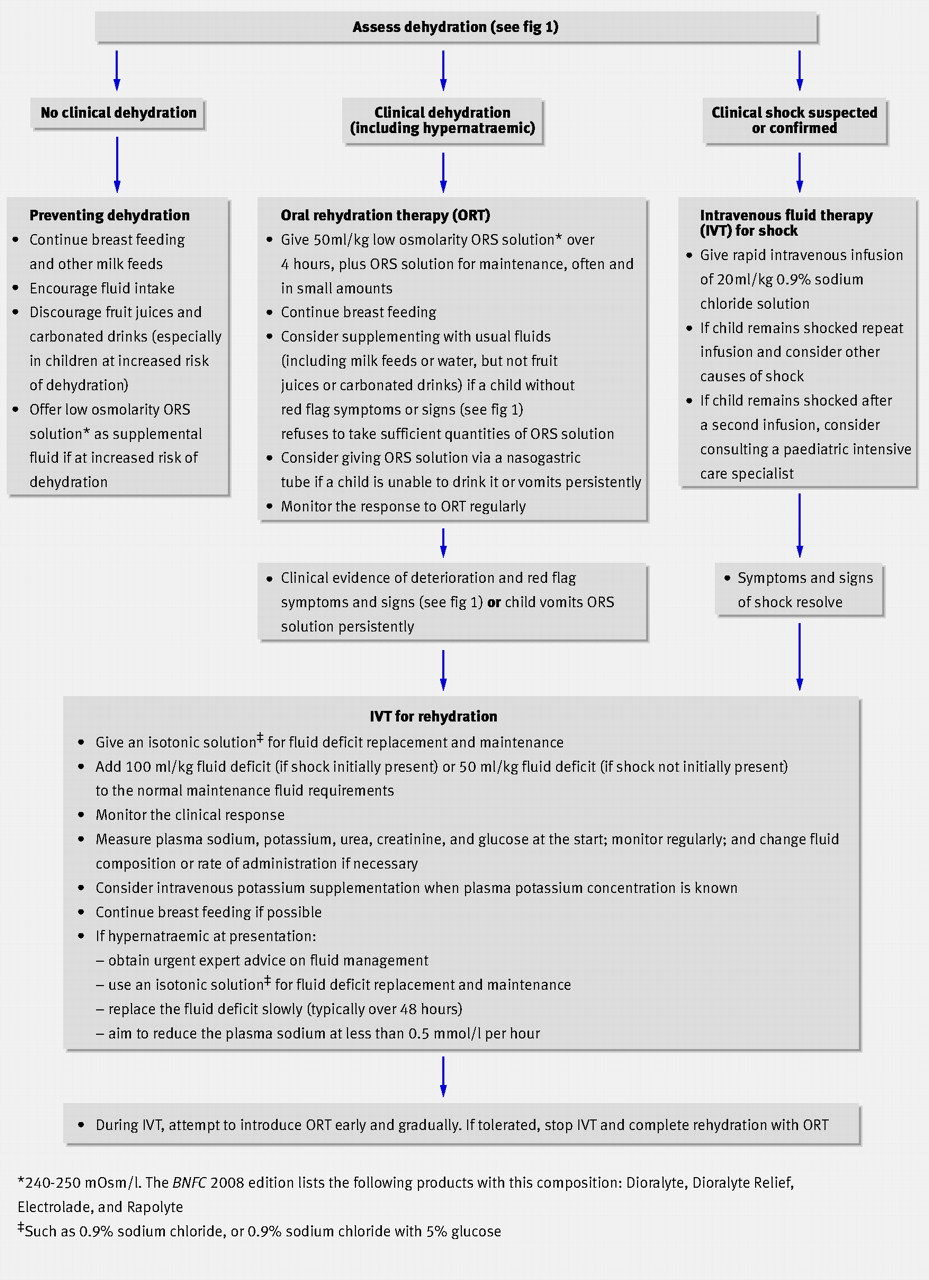
Fig 2 Flow pathway for fluid management of children with gastroenteritis. ORS=oral rehydration salt
{kind=link}
Fluid management after rehydration
Encourage breast feeding, other milk feeds, and fluid intake.
Consider giving 5 ml/kg oral rehydration salt (ORS) solution after each large watery stool to:
-Children younger than 1 year (especially those younger than 6 months)
-Infants who were of low birth weight
-Children who have passed six or more diarrhoeal stools in the past 24 hours
-Children who have vomited three times or more in the past 24 hours.
If dehydration recurs, start oral rehydration therapy again.
[All recommendations based on high quality meta-analyses of randomised controlled trials (RCTs), moderate quality RCTs, and the experience and opinion of the GDG]
Nutritional management
During rehydration treatment:
-Continue breast feeding
-Do not give solid foods
-In children with red flag symptoms or signs, do not give oral fluids other than ORS solution
-In children without red flag symptoms or signs, do not routinely give oral fluids other than ORS solution; however, consider supplementation with the child’s usual fluids (including milk feeds or water, but not fruit juices or carbonated drinks) if they consistently refuse ORS solution.
After rehydration:
-Give full strength milk straight away
-Reintroduce the child’s usual solid food
-Avoid giving fruit juice and carbonated drinks until the diarrhoea has stopped.
[All recommendations based on moderate quality RCTs and moderate quality observational studies]
Treatment with antibiotics
Do not routinely give antibiotics to children with gastroenteritis.
Give antibiotics to all children:
-With suspected or confirmed septicaemia
-With extraintestinal spread of bacterial infection
-Younger than 6 months with Salmonella gastroenteritis
-Who are malnourished or immunocompromised with Salmonella gastroenteritis
-With Clostridium difficile associated pseudomembranous enterocolitis, giardiasis, dysenteric shigellosis, dysenteric amoebiasis, or cholera.
Seek specialist advice for children who have recently been abroad.
[All recommendations based on moderate quality RCTs and the experience and opinion of the GDG]
Other treatments
Do not use antidiarrhoeal drugs. [Based on moderate quality meta-analysis of RCTs and moderate quality RCTs]
Escalation of care
During remote assessment
Arrange emergency transfer to secondary care for children with symptoms suggesting shock
Refer the following children for face to face assessment:
-Those with symptoms suggesting an alternative serious diagnosis
-Those at high risk of dehydration after taking into account the risk factors
-Those with symptoms of clinical dehydration
-Those whose social circumstances make remote assessment unreliable.
Provide a “safety net” for children who do not need referral, including information for parents or carers on how to:
-Recognise developing red flag symptoms
-Get immediate help from an appropriate healthcare professional if red flag symptoms develop.
During face to face assessment
Arrange emergency transfer to secondary care for children with symptoms or signs of shock
Consider repeat face to face assessment or referral to secondary care for children:
-With clinical features suggesting an alternative serious diagnosis
-With red flag features
-Whose social circumstances require continued involvement of healthcare professionals.
Provide a safety net for children who will be managed at home, including:
-Information for parents and carers on how to recognise developing red flag symptoms
-Information on how to get immediate help from an appropriate healthcare professional if red flag symptoms develop
-Arrangements for follow-up at a specified time and place, if necessary.
[All recommendations based on the experience and opinion of the GDG]
Advice for parents and carers
Caring for a child at home
Advise parents and carers:
-That most children with gastroenteritis can be safely managed at home, with advice and support from a healthcare professional if necessary
-About symptoms that may indicate dehydration, and that they should contact a healthcare professional if such symptoms develop
-About fluid management and nutritional management when treating dehydration and in the post-rehydration phase, and that they must take into account the risk factors for dehydration and the clinical assessment (fig 1)
-About the usual duration of diarrhoea (five to seven days, with most cases resolving within two weeks) and vomiting (one or two days, with most cases resolving within three days), and to seek advice from a specified healthcare professional if symptoms do not resolve within these time frames.
[All recommendations based on the experience and opinion of the GDG]
Preventing primary spread of gastroenteritis
Advise parents, carers, and children that:
-Washing hands with soap (liquid if possible) in warm running water and carefully drying them afterwards are the most important factors in preventing spread
-Hands should be washed after going to the toilet (children) or changing nappies (parents and carers) and before preparing, serving, or eating food
-Children with gastroenteritis should not share towels
-Children should not attend school or another childcare facility while they have diarrhoea or vomiting; they should not return until at least 48 hours after the last episode of diarrhoea or vomiting
-Children should not swim in a swimming pool for two weeks after the last episode of diarrhoea.
[All recommendations adapted from the guidelines commissioned by the Department of Health]
Overcoming barriers
The new approach to clinical assessment of dehydration is innovative and unfamiliar to clinicians: it does not imply that the degree of dehydration is uniform but acknowledges the difficulties in accurately assessing the severity of dehydration. It also links directly to fluid management; it recommends a standardised fluid regimen for all (non-shocked) children with dehydration, with subsequent adjustments based on regular reassessment during rehydration. This approach is simple, easy to implement, and it provides the clinical information necessary for appropriate fluid management. By emphasising oral rehydration with low osmolarity ORS solution (given orally or via a nasogastric tube) as the firstline treatment of dehydration and limiting intravenous fluids to selected children, the guideline will help avoid the complications and distress associated with intravenous canulation and reduce hospital costs. It also standardises advice on nutritional management during and after the episode of gastroenteritis and the escalation of care from the community to various hospital settings.
Further information on guidance
Over the past three decades, global mortality attributable to gastroenteritis in children under 5 years has dropped significantly, although gastroenteritis still causes 1.6-2.6 million deaths worldwide in this age group.5 Deaths associated with gastroenteritis are now rare in developed countries, but the condition itself puts a considerable burden on health service resources. In a multicentre European study, about 10% of children under 5 presented to healthcare services with gastroenteritis each year.6 In a UK study, diarrhoeal illness accounted for 16% of medical presentations to a major paediatric emergency department.7 A community based study from England estimated that each year 9.4 million cases of gastroenteritis occur in the community and 1.5 million cases present to primary care.8
What’s new?
The management of gastroenteritis in children is multifaceted and changing. New therapeutic agents (such as antiemetics, antidiarrhoeals, and probiotics) and management strategies (rapid rehydration with intravenous fluids) are being proposed, but their efficacy and safety are unclear. Various approaches to the clinical assessment of the severity of dehydration and hence to the calculation of fluid deficits have been proposed. Against this changing background, and despite the existence of several guidelines, clinical practice is thought to vary considerably regarding the use of oral versus intravenous fluids for rehydration, administration of fluids via a nasogastric tube, nutritional management of infants and children during and after an episode of gastroenteritis, and the approach to escalation of care from the community to hospital settings. Inconsistent advice is also offered to parents on the types of oral fluids and feeds to be given and when to start solid feeds.
This guideline aims to standardise clinical practice in England and Wales by providing evidence based guidance on the diagnosis, assessment, and management of diarrhoea and vomiting caused by gastroenteritis in children under 5 years who present to a healthcare professional for advice in any setting.
Methods
The guideline was developed by the National Collaborating Centre for Women’s and Children’s Health in accordance with the NICE guideline development process as outlined in the NICE technical manual (www.nice.org.uk/aboutnice/howwework/developingniceclinicalguidelines/clinicalguidelinedevelopmentmethods/GuidelinesManual2009.jsp). A guideline development group was established, with two paediatric gastroenterologists (including the chair), two general paediatricians (including one community paediatrician), one paediatric specialist in infectious diseases, one emergency department paediatric specialist, three general practitioners, three nurses (including one emergency nurse practitioner), one nurse with expertise in remote assessment through NHS Direct, and two parent or carer members. The technical team from the collaborating centre, led by the clinical codirector who is a community paediatrician, provided methodological support for the guideline development process, undertook systematic literature searches, retrieval, appraisal, and synthesis of the evidence; the team also undertook health economics modelling and, together with the chair, wrote successive drafts of the guideline. The guideline scope at initial development and the final guideline draft were both revised to take into account comments received from registered stakeholder organisations. Future updates of the guidance will be prepared according to the NICE guideline development process.
Areas of future research
Research recommendations have been submitted for inclusion in the UK database of uncertainties about the effects of treatments (DUETs; www.library.nhs.uk/DUETS/) and the NICE research recommendations database (www.nice.org.uk/research/index.jsp?action=rr) to help prioritise new research within the UK.
Assessing dehydration and shock
In children with gastroenteritis, what is the predictive value of clinical symptoms and signs in assessing the severity of dehydration, using post-rehydration weight gain as the reference standard, in primary and secondary care settings?
Administration of oral rehydration salt solution by nasogastric tube
In children who do not tolerate oral rehydration, how does the administration of oral rehydration salt solution via a nasogastric tube compare with intravenous treatment in terms of cost effectiveness, safety, and acceptability?
Fluid management
In children who need intravenous fluids to treat dehydration, is rapid rehydration safe and cost effective compared with the common practice of rehydration over 24 hours?
Other treatments: ondansetron
In children with persistent vomiting caused by gastroenteritis, is oral ondansetron cost effective and safe compared with placebo?
Other treatments: probiotics
Are probiotics effective and safe compared with a placebo in treating children with gastroenteritis in the UK? Which probiotic is most effective and in what treatment regimen?
Notes
Cite this as: BMJ 2009;338:b1350
Footnotes
This is one of a series of BMJ summaries of new guidelines, which are based on the best available evidence; they highlight important recommendations for clinical practice, especially where uncertainty or controversy exists.
The members of the Guideline Development Group are M Stephen Murphy (chair), senior lecturer and consultant paediatric gastroenterologist; Ed Abrahamson, consultant in paediatric emergency medicine; Richard Churchill, general practitioner and clinical associate professor; Dianne L Cook, community advanced nurse practitioner; John Crimmins, general practitioner; Saul Faust, senior lecturer and honorary consultant in paediatric immunology and infectious diseases; Alastair Hay, consultant senior lecturer in primary health care; Naryndar Johal, parent or carer member; Julie Marriott, parent or carer member; Nigel Meadows, consultant paediatric gastroenterologist and honorary senior lecturer; Simon Minford, advanced paediatric nurse practitioner and lecturer; Robert Moy, senior lecturer in community child health; Enid Povey, national clinical development manager in NHS Direct; Gyanranjan Sinha, consultant paediatrician; Jenny Taylor, advanced paediatric nurse practitioner.
Members of the technical team at National Collaborating Centre for Women’s and Children’s Health are Shona Burman-Roy, research fellow; Rosie Crossley, work programme coordinator; Sjokvist Garcia-Stewart, research fellow; Alyson Huntley, freelance researcher; Itrat Iqbal, health economist; Paul Jacklin, senior health economist; Rajesh Khanna, senior research fellow; Angela Kraut, research fellow; Monica Lakhanpaul, clinical codirector and senior lecturer in child health; Ana Palanca, research fellow; Edmund Peston, document supply coordinator; Andrew Welsh, freelance editor; Danielle Worster, information scientist.
Contributors: All the authors wrote the initial draft of the article using material developed collectively by the Guideline Development Group and contributed to the revision and the final draft of this article. They have all approved this version. MSM is guarantor.
Funding: The National Collaborating Centre for Women’s and Children’s Health was commissioned and funded by the National Institute for Health and Clinical Excellence to write this summary.
Competing interests: All authors were members of the Guideline Development Group (RK was the senior research fellow, ML was the clinical codirector, SB-R was the research fellow, and MSM chaired the group).
Provenance and peer review: Commissioned; externally peer reviewed.