Is streaming patients in emergency departments to primary care services effective and safe?
BMJ 2020; 368 doi: https://doi.org/10.1136/bmj.m462 (Published 25 February 2020) Cite this as: BMJ 2020;368:m462
- Alison Cooper, clinical research fellow1,
- Andrew Carson-Stevens, clinical reader in patient safety and quality improvement1,
- Thomas Hughes, emergency medicine consultant2,
- Adrian Edwards, professor of general practice1
- 1Division of Population Medicine, School of Medicine, Cardiff University, UK
- 2John Radcliffe Hospital, Oxford, UK
- Correspondence to A Cooper CooperA8{at}cardiff.ac.uk
What you need to know
Co-located primary care services have been introduced in emergency departments in the UK to reduce crowding and improve patient care and safety
There is limited, outdated evidence to show whether streaming emergency department patients to primary care services improves patient flow and reduces costs; and evidence is lacking for patient safety outcomes
Commissioners and service providers should consider whether governance systems are clear and reflect whether general practitioners in emergency departments are encouraged to function more as primary care or emergency medicine clinicians to suit the local patient demographic profile, demand patterns, and staff recruitment needs
Between 10% and 43% of patients presenting to emergency departments can be managed in primary care, according to estimates from observational studies.1234 Increasing demands on emergency healthcare systems have led to the development of different healthcare models, including “streaming” patients presenting with non-urgent conditions to primary care services.5 These strategies are intended to improve patient flow and reduce crowding in the emergency department. In 2017 NHS England made substantial investments for all emergency departments to have co-located primary care facilities so they are “free to care for the sickest patients.”67
However, the evidence for this initiative is weak.89101112 Different service models are described in different contexts using ambiguous terminology. A “co-located” primary care service may deliver patient care in a separate unit to the emergency department, without access to acute diagnostics, thus similar to normal general practice settings. Alternatively, general practitioners may work within the emergency department, with responsibilities beyond usual primary care.13 It is uncertain if national implementation of streaming, considering the heterogenous nature of emergency medicine case mix and practice, improves patient care and safety.
What is the evidence of uncertainty?
There are few large scale evaluations of healthcare delivery models offering co-located primary care services. Studies have heterogeneous designs, making it difficult to draw conclusions on safety and effectiveness. Table 1 describes findings from reviews.89101112 A Cochrane review found few studies on effects of general practitioners seeing non-urgent patients in hospital emergency departments. The results were inconsistent and highlighted a lack of evidence for effectiveness outcomes, with no data available for mortality or safety events. 8
Summary of evidence for effectiveness and safety of primary care services co-located with emergency departments
A narrative review described an increase in attendances at emergency departments with co-located primary care services that was attributed to the service creating its own demand—provider induced demand. There was little evidence on improved patient flow or costs to recommend this model.11A rapid realist review found little evidence that general practitioner services in emergency departments influenced the care and throughput of the sickest patients, with other factors, including delayed patient transfers to wards and inadequate staffing, also contributing.12 Factors such as how staff interpret the streaming system and the roles adopted by general practitioners (whether they function in their traditional role or adopt an emergency medicine approach) could influence effectiveness of service models.
Given the limited, outdated clinical and cost-effectiveness evidence and concerns about the feasibility of staffing the workforce, the National Institute for Health and Care Excellence (NICE) chose not to make a recommendation for general practitioners to work within or on the same site as emergency departments, and called for further research in this area.
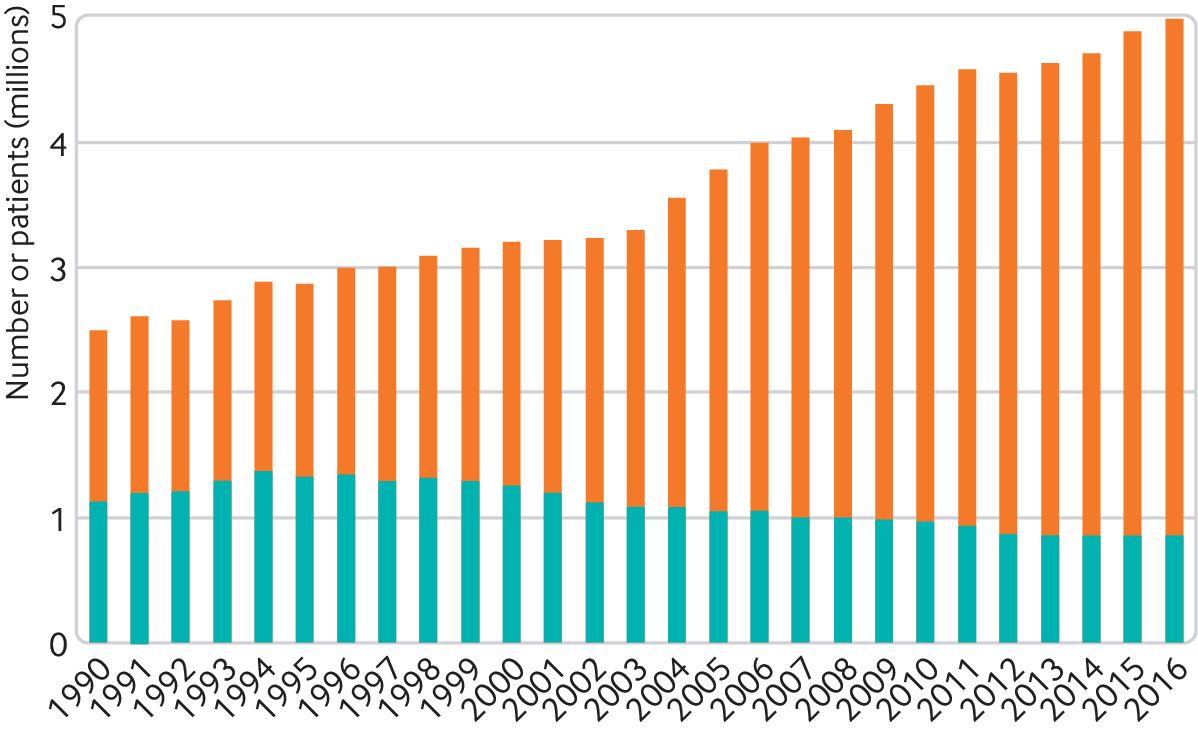
NHS England hospital episode statistics data show increasing numbers of hospital admissions from emergency departments rather than general practices (fig 1). Should interventions in emergency departments, which may include the expertise of general practitioners focussing on specific patient groups, prioritise preventing these admissions rather than treating patients with non-urgent conditions?
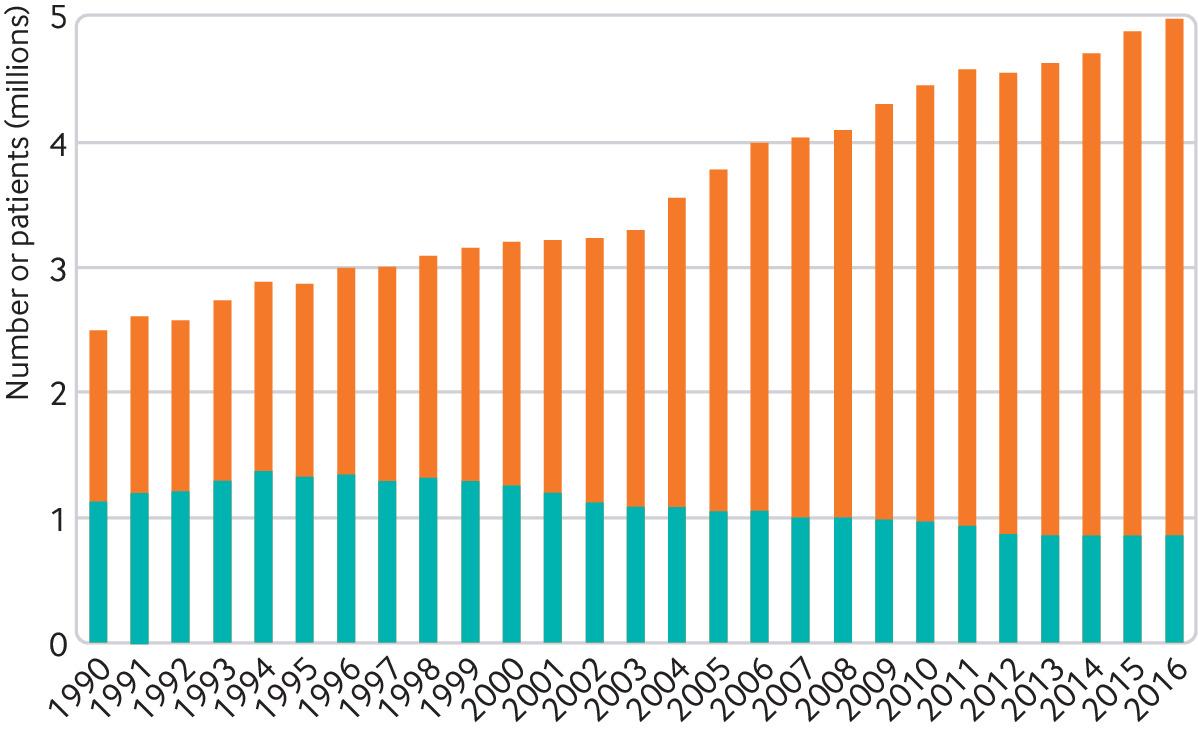
UK National Health Service hospital episode statistics showing emergency admissions from emergency departments (orange) and general practice (blue). Source: NHS Digital, 2017
{kind=link}
Is ongoing research likely to provide relevant evidence?
We searched EU Clinical Trials Register, ISRCTN Registry, ClinicalTrials.gov, and ICTRP, and identified a Belgian study on effectiveness of a triage system for patients presenting to emergency departments with referral to primary care.14
The UK National Institute for Health Research has commissioned two observational studies (HS&DR Projects 15/145/04 and 15/145/06) to evaluate the effectiveness, safety, patient experience, and system implications of the different models of general practitioners working in or alongside emergency departments.1516 Effectiveness will be evaluated by waiting times, admission rates and (re)attendances, patient satisfaction, and cost-consequence analysis, with patient safety incident reports analysed for patient safety outcomes. The teams have collaborated to update the taxonomy to ensure consistency of terminology and classification of models, and to include the wider primary care workforce.13Figure 2 shows the form these service models take, inside and outside emergency departments.13 The studies, due to be completed in 2021, will attempt to identify service models that may be better suited depending on local demographics and contexts.

The form of primary care service models in or alongside emergency departments. Adapted from Emerg Med J 2019;36:625-30
{kind=link}
What should we do in the light of the uncertainty?
Clinicians, service directors, managers, and commissioners should acknowledge the current evidence gap for effectiveness and safety in this area. The function of these service models is complex and influenced by many variables at multiple levels including: wider system determinants (eg patient demand, staffing); department level (eg access to investigations, governance); and individual level (eg, experience, skill set and interest).13
Emergency department and primary care clinical leads should jointly consider which patients are appropriate for their local primary care service model and whether their model functions as usual primary care or is more integrated with the emergency medicine service. Clarification of governance processes is important. Where these models are operational, staff can reflect on how and why the service works well, for example through the patient safety incident reporting system, and identify what can be learned from this to continue to deliver safe patient care.
Education into practice
In what ways does your emergency department primary care service meet the needs of the local population and local context?
What data do you already have to support this assessment?
What data do you need to identify how to improve the service?
How patients were involved in the creation of this article
Patient representatives were involved as public collaborators and co-applicants on the NIHR funded study of GPs working in or alongside emergency departments. They have given feedback on findings from the realist review and on taxonomy. No patients were directly involved in writing or reviewing this article.
Recommendation for further research
How can individual primary care services at emergency departments be most effective for local needs?
What are the patient safety implications for primary care services co-located with emergency departments? How can these be mitigated?
What interventions in emergency departments can safely reduce the number of acute hospital admissions?
Footnotes
This is one of a series of occasional articles that highlight areas of practice where management lacks convincing supporting evidence. The series advisers are Sera Tort, clinical editor, Nai Ming Lai, clinical editor, and David Tovey, editor in chief, the Cochrane Library. You can read more about how to prepare and submit an Education article on our Instructions for Authors pages:https://www.bmj.com/about-bmj/resources-authors/article-types
Acknowledgments The authors would like to thank Prof Matthew Cooke for his contributions towards this article.
Competing Interests AC, AC-S, TH and AE are all co-applicants on the NIHR HS&DR study Project: 15/145/04—A realist evaluation of effectiveness, safety, patient experience and system implications of different models of using GPs in or alongside Emergency Departments.
Disclaimer This study is funded by the National Institute for Health Research (NIHR) HS&DR Project 15/145/04. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Provenance and peer review: commissioned; externally peer reviewed.