Article Text

Abstract
Background Respiratory complications remain a leading cause of morbidity and mortality in people with acute and chronic tetraplegia. Respiratory muscle weakness following spinal cord injury-induced tetraplegia impairs lung function and the ability to cough. In particular, inspiratory muscle strength has been identified as the best predictor of the likelihood of developing pneumonia in individuals with tetraplegia. We hypothesised that 6 weeks of progressive respiratory muscle training (RMT) increases respiratory muscle strength with improvements in lung function, quality of life and respiratory health.
Methods Sixty-two adults with tetraplegia participated in a double-blind randomised controlled trial. Active or sham RMT was performed twice daily for 6 weeks. Inspiratory muscle strength, measured as maximal inspiratory pressure (PImax) was the primary outcome. Secondary outcomes included lung function, quality of life and respiratory health. Between-group comparisons were obtained with linear models adjusting for baseline values of the outcomes.
Results After 6 weeks, there was a greater improvement in PImax in the active group than in the sham group (mean difference 11.5 cmH2O (95% CI 5.6 to 17.4), p<0.001) and respiratory symptoms were reduced (St George Respiratory Questionnaire mean difference 10.3 points (0.01–20.65), p=0.046). Significant improvements were observed in quality of life (EuroQol-Five Dimensional Visual Analogue Scale 14.9 points (1.9–27.9), p=0.023) and perceived breathlessness (Borg score 0.64 (0.11–1.17), p=0.021). There were no significant improvements in other measures of respiratory function (p=0.126–0.979).
Conclusions Progressive RMT increases inspiratory muscle strength in people with tetraplegia, by a magnitude which is likely to be clinically significant. Measurement of baseline PImax and provision of RMT to at-risk individuals may reduce respiratory complications after tetraplegia.
Trial registration number Australian New Zealand Clinical Trials Registry (ACTRN 12612000929808).
- exercise
- pulmonary rehabilitation
- respiratory muscles
- respiratory measurement
- respiratory infection
- perception of asthma/breathlessness
Statistics from Altmetric.com
- exercise
- pulmonary rehabilitation
- respiratory muscles
- respiratory measurement
- respiratory infection
- perception of asthma/breathlessness
Key messages
What is the key question?
Does progressive respiratory muscle training increase respiratory muscle strength in people with tetraplegia?
What is the bottom line?
Increased respiratory muscle strength could reduce respiratory complications, which are one of the leading causes of morbidity and mortality in people with tetraplegia.
Why read on?
Respiratory muscle training can increase muscle strength with consequential physiological effects.
Introduction
Respiratory muscle weakness following spinal cord injury-induced tetraplegia has profound consequences. First, impairment of the inspiratory muscles affects ventilation and lung volumes. Second, ineffective expiratory muscles impair cough and secretion clearance. As a result, respiratory morbidity for individuals with tetraplegia is high with a lifetime of recurrent respiratory tract infections (2/year/person) that often progress to pneumonia.1 2
After tetraplegia, the highest incidence of mortality occurs in the first year with respiratory causes accounting for 28% of deaths.3 The annual incidence of hospital admissions due to pneumonia and atelectasis are 16% in the first year and 12% at 5 years postinjury.2 For those who survive 1 year, tetraplegia has a lifetime cost of $A9.5 million, much of which is attributed to respiratory-related complications.4 Consequently, respiratory muscle weakness is a leading cause of morbidity and mortality in people with tetraplegia.1 5
A common measure of respiratory muscle strength is maximal inspiratory pressure (PImax) or maximal expiratory pressure (PEmax). PImax may be a discriminator of pneumonia in individuals with tetraplegia with those below threshold values at increased risk.6 Therefore, strengthening the respiratory muscles, in particular the inspiratory muscles would be of significant benefit for people with tetraplegia.
Respiratory muscles are skeletal muscles and studies both in able bodied subjects7 and in neuromuscular disorders8 have shown that training can improve inspiratory and expiratory muscle strength as well as lung function. Volitional training cannot improve the function of completely paralysed muscles. However, training has the potential to strengthen the activation and coordination of those respiratory muscles that are partially paralysed through incomplete injury and also muscles that remain fully innervated. Several techniques of respiratory muscle training (RMT) in people with tetraplegia have been described with the aim to strengthen and improve the endurance of inspiratory and expiratory muscles. These techniques include breathing against abdominal weights,9 resistive and threshold loading devices,9–15 incentive flow spirometry,16 positive expiratory pressure devices,17 glossopharyngeal breathing18 19 and singing.20 Although many of these techniques improved lung function, there is no conclusive evidence to support one method over another. A relatively recent Cochrane review concluded that further research was required on the effectiveness of RMT in tetraplegia.21 A meta-analysis of randomised controlled trials (RCTs) showed there is potential for training to improve respiratory function. However, previous studies were limited with a majority having low power, inadequate group allocation concealment and/or blinding of participants and assessors. Some studies had very short training programmes with other studies having incomplete data.22
The aim of the current study was to conduct an RCT with adequate power to assess the effect of RMT, using a low-cost threshold respiratory muscle trainer and a progressive training regimen. We hypothesised that 6 weeks of progressive RMT increases respiratory muscle strength with improvements in lung function, quality of life (QoL) and respiratory health (respiratory symptoms and complications).
Methods
Study participants
Sixty-two people with tetraplegia were recruited from Prince of Wales Hospital, Sydney, Australia, and from the community. Trial eligibility criteria are outlined in box 1. We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during this research. All participants provided informed written consent with an aid of a family member or independent third party prior to enrolment.
Trial eligibility criteria
Inclusion
Aged ≥18 years.
Spinal cord injury-induced tetraplegia between C4 and C8 with related respiratory deficits.
American Spinal Injury Association Impairment Scale grades A, B or C defined by the International Standards for Neurological Classification of Spinal Cord Injury.
Medically stable as deemed by treating physician.
At least 4 weeks after initial injury date.
Exclusion
Mechanically ventilated.
Pregnancy.
Significant chest trauma such as flail ribs or pneumothorax.
Diagnosis of a major coexisting respiratory or neurological illness or a cognitive impairment.
Study design
A single-site randomised double-blind placebo (sham) controlled trial was undertaken.
Randomisation and blinding
A computer-generated adaptive random allocation schedule was created by a person not involved in data collection or recruitment. Participants were allocated to sham or active treatment in a 1:1 ratio (concealed). The allocation algorithm implemented in Stata minimised imbalances in two prognostic factors: American Spinal Injury Association Impairment Scale grade (A and B vs C) and time since injury (<6 months vs >1 year). At completion of each participant’s baseline assessment, an allocation request was placed to an independent person who revealed the participant’s group allocation. A participant was considered to have entered the trial at this point. Participants, treating therapists and assessors were blinded to the allocated treatment group throughout the trial.
Procedures
All participants performed supervised RMT with a single threshold RMT device (Threshold IMT, Respironics, New Jersey, USA). The sham device was modified to hold the pressure valve permanently open. A ring of tape encircled each device to disguise the valve position. Thus, the sham device was identical in appearance to the active device. All devices had the appearance of the resistance being altered depending on participant respiratory strength, but the sham device resistance did not change. Training followed a non-linear exercise regimen, which increased the training intensity as strength improved. Three to five sets of 12 breaths, separated by quiet breathing for 2 min, were performed twice daily, 5 days a week for 6 weeks. All participants commenced with inspiratory training each session and progressed to expiratory training after 2 min of quiet breathing. Participants inspired from end-tidal volume, through a mouthpiece attached to the inspiratory end of the device, and the resistance was set initially to 30% of each participant’s baseline PImax. This setting was subsequently increased each week by 10% weekly measured PImax if tolerated (capped at 80% weekly measured PImax), otherwise the resistance was increased by 5%. The protocol for expiratory training was identical except that participants exhaled through the opposite end of the same device from total lung capacity (TLC). The expiratory resistance was set at 30% baseline PEmax and increased each week as above. The training intensity, duration and frequency were based on limb muscle protocols and protocols used to effectively train respiratory muscles in patients with chronic obstructive pulmonary disease and motoneurone disease.8 23 Tolerance to the training was measured using the Modified Borg score for ‘difficulty to breathe through the device’, participant score of ‘severe’ (5) or greater was considered as non-tolerance.
Outcomes
The apriori primary outcome was inspiratory muscle strength at 6 weeks, indicated by PImax adjusted for pretraining PImax, between the active and sham training groups. Voluntary PImax was measured at functional residual capacity (FRC) using a portable lung function machine (Hyp’air, Belgium) according to American Thoracic Society guidelines. Secondary outcomes of lung function included measures of inspiratory capacity (IC), vital capacity (VC), FVC, FEV1, peak expiratory flow while coughing (PEFc), TLC and PEmax at TLC. A minimum of three attempts of each measure was made, within 5% error, and the best performance recorded for analysis. Perceived breathlessness was rated at rest and during respiratory loading (15 cmH2O) using the Modified Borg Scale. Respiratory-related morbidity was recorded as the number of respiratory infections (verified by participant’s medical practitioner) and infections requiring hospitalisation (verified by radiological evidence) within 1 year after the completion of the intervention. Respiratory health was assessed by the St George Respiratory Questionnaire (SGRQ).24 QoL was measured using the Short Form Health Survey: walk/wheel (SF-36ww) validated for people with SCI25 and the EuroQol-Five Dimensional Visual Analogue Scale (EQ-5D VAS).26 All measures were made at baseline, 6 weeks and 1 year. At the completion of the 1-year follow-up, participants were given a new unaltered device to continue training, but were not told their group allocation.
Statistical analysis
A minimum of 32 participants per group was calculated apriori to be sufficient to detect a clinically meaningful improvement (on the advice of respiratory staff specialists) of a between-group difference of 10 cmH2O in the primary outcome measure at 6 weeks. Recruitment of 80 participants would allow for an estimated 20% dropout. Power calculations were based on published data where baseline PImax ranged from 40 to 63 cmH2O (SD=14 cmH2O,14 16 27 power=0.8, two-tailed α=0.05). A 10 cmH2O increase in PImax represents a potential 16% to 25% increase in strength reported in the literature, a worthwhile improvement for people with a low PImax.
Data were analysed on an intention-to-treat basis.28 Missing data were deleted on a case-wise basis. Primary outcome data and lung function measures were analysed with analysis of covariance, adjusting for the baseline measures with a linear regression approach. We conducted a sensitivity analysis on the primary analysis to determine if the findings were sensitive to parametric assumptions and CIs were estimated using non-parametric bootstrapping (1000 bootstrap replicates). The treatment effect size was estimated with the between-group mean difference and 95% CIs. Data from the questionnaires were analysed using t-tests and categorical data were analysed using χ2 or Fisher’s exact tests. P values <0.05 were considered statistically significant.
Results
Sixty-two people with tetraplegia were recruited between November 2013 and November 2016 (1-year follow-up ceased in December 2017), figure 1 shows participant flow. Baseline characteristics were well matched between groups (table 1). The training protocol was adhered to by all participants, a median of 4.1 sets of 12 breaths were performed twice daily (IQR 3.8–4.5) for 6 weeks. There was no difference between the groups in RMT frequency (table 2). There were no reported adverse events over the course of this trial.

Participant flow throughout trial duration. RMT, respiratory muscle training.
Participant characteristics at baseline
Respiratory muscle training parameters per group allocation after 6 weeks
The sham device generated pressures between 1 and 7.7 cmH2O during inspiration and between 1 and 5.3 cmH2O during expiration, with corresponding flow rates between 0.5 and 2 L/s. Using the mid-flow rate (1.25 L/s) as representative, the pressure generated during inspiration and expiration was 3.6 cmH2O with a mean resistance of 4.1 cmH2O/L/s, linear across the flow range. The mean baseline, maximum and average RMT pressures were different, and the active group were trained at significantly higher pressures than the sham group (table 2). The mean work performed and corresponding Borg scores were different, and the active group had significantly higher values than the sham group (table 2). During the 6 weeks, the training intensity of the active group (measured as percentage of initial pressures) increased at a decreasing rate and stabilised after ~4 weeks (figure 2).

Mean respiratory muscle training (RMT) intensity (±SD) per week represented as percentage of initial maximal inspiratory pressure or initial maximal expiratory pressure.
Primary outcome
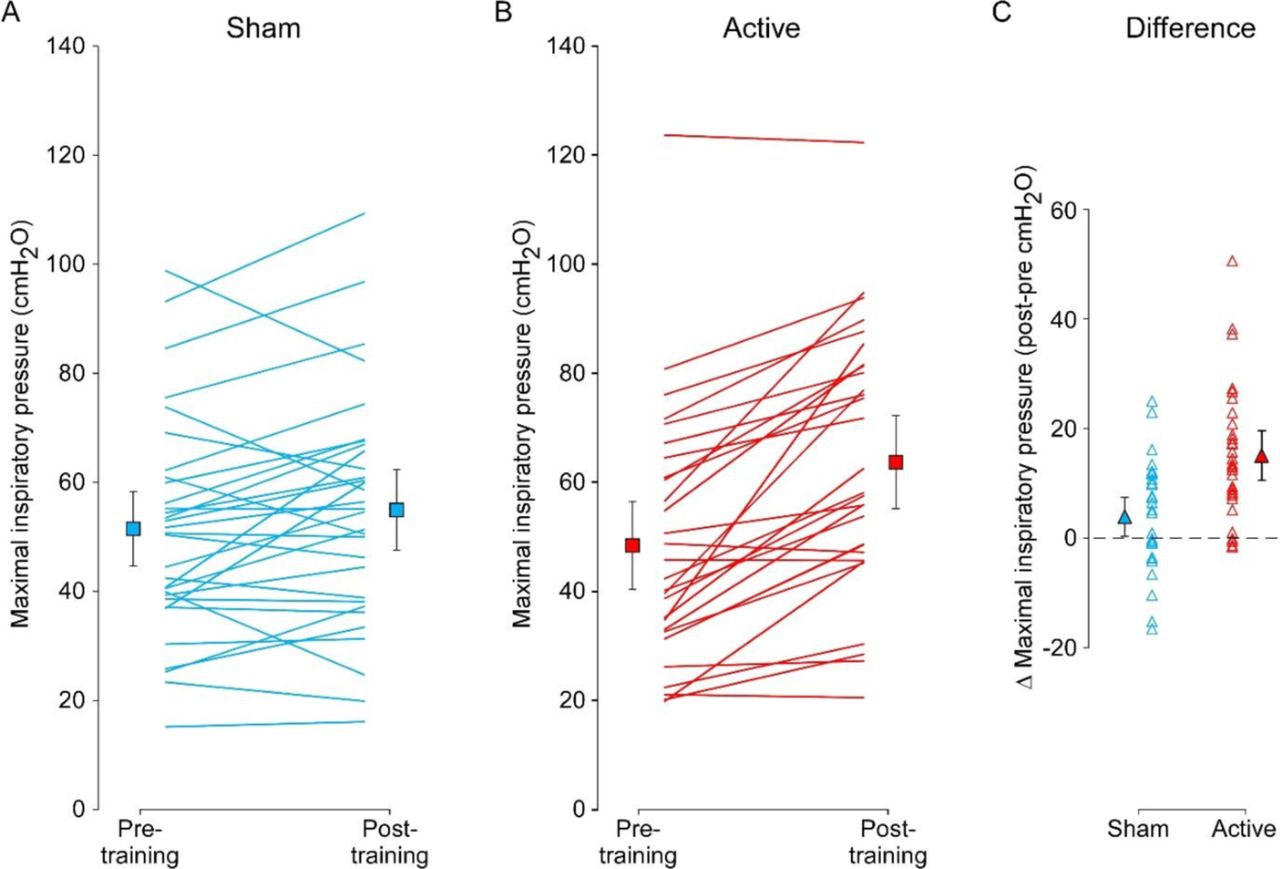
After 6 weeks of RMT, PImax was significantly greater in the active group compared with the sham group (table 3). The mean between-group difference for all participants was 11.5 cmH2O (95% CI=5.6 to 17.4, p<0.001). The confidence limits from the sensitivity analysis were similar to those in the primary analysis (5.81 to 17.01). Individual and group data at baseline and 6 weeks are shown in figure 3. Compared with mean baseline measures, PImax increased by 31.6% in the active group compared with 6.7% in the sham group. There were significant increases in mean PImax in both acute (difference between groups 12.3 cmH2O, 95% CI=2.1 to 22.3, p=0.021) and chronic groups (difference between groups 11.2 cmH2O, 95% CI=3.3 to 19.1, p=0.011) (table 4). There were also increases in mean PImax in the motor-complete (difference between groups 12.3 cmH2O, 95% CI=4.7 to 20.0, p=0.002) and motor-incomplete groups (difference between groups 10.8 cmH2O, 95% CI=−0.06 to 21.7, p=0.051) (table 5). Using predictive modelling calculators developed by Mueller et al, 29 our mean tetraplegia-predicted PImax for motor-complete tetraplegia are 66% at baseline and 91% after 6 weeks of RMT.

Maximal inspiratory pressures before and after 6 weeks of RMT for individual participants in the sham group (blue lines, panel A) and the active group (red lines, panel B), the solid squares represent group mean±SD. Panel C plots the individual participant changes (open triangle) in maximal inspiratory pressures after 6 weeks of RMT, with mean group change (±95% CI) in the solid triangle.
Outcome measures at baseline, after 6 weeks of RMT and after 1 year of unsupervised training
Outcome measures at baseline and after 6 weeks of RMT for groups divided by time since injury (acute group less than 1 year and chronic group greater than 1 year since injury)
Outcome measures at baseline and after 6 weeks of RMT for groups divided by AIS classification (motor complete group classified as AIS A and B and the motor incomplete group classified as AIS C)
Secondary outcomes
After 6 weeks of training, respiratory symptom severity (SGRQ) score for all participants improved more in the active group compared with the sham group (mean between-group difference 10.3 points, 95% CI 0.01 to 20.65, p=0.046; table 3). The chronic active group had a lower mean score on the EQ-5D VAS, compared with the chronic sham group (mean between-group difference 14.9, 95% CI 1.9 to 27.9, p=0.023; table 4).
Borg scores for breathlessness during 10 inspiratory loaded breaths reduced more in the active group compared with the sham group for all participants (mean between-group difference 0.96, 95% CI 0.01 to 1.91, p=0.049; table 3), and for participants with a chronic injury (mean between-group difference −1.92, 95% CI −0.6 to −3.3, p=0.009; table 4), but not during 10 expiratory loaded breaths. Borg scores at rest were greater in the sham group for all participants (mean between-group difference 0.64, 95% CI 0.11 to 1.17, p=0.021; table 3) and for participants with an acute injury (mean between-group difference 0.94, 95% CI 0.2 to 1.8, p=0.025; table 4).
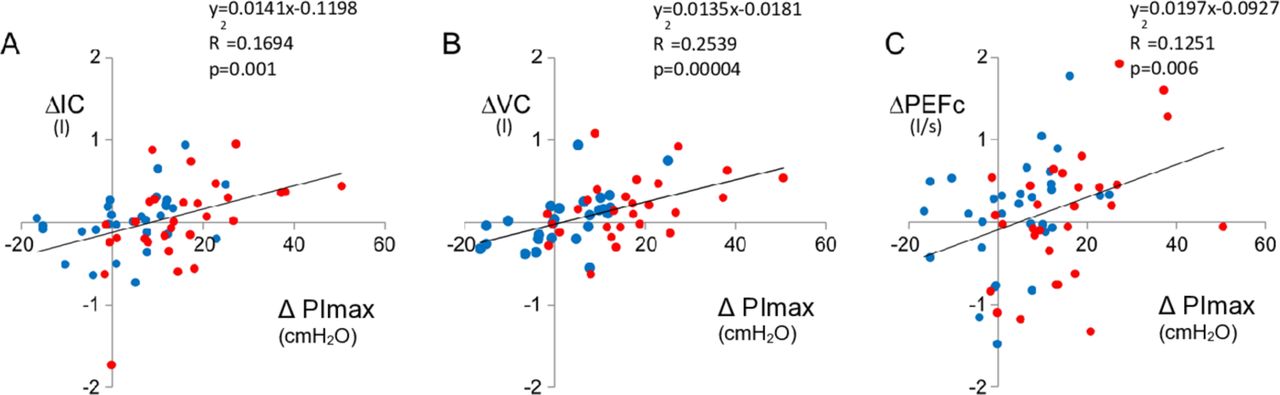
There was no significant difference between the sham and active groups in PEmax, lung function, number of respiratory complications, remaining SF-36ww fields and SGRQ domains (table 3), nor when analysed by time since injury (table 4) or degree of injury completeness (table 5). However, there were significant correlations between the change in PImax and the change in IC, VC and PEFc (figure 4). For every 10 cmH2O improvement in PImax, there was a 140 mL increase in IC (figure 4A), 135 mL increase in VC (figure 4B) and 200 mL/s increase in PEFc (figure 4C).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Change in maximal inspiratory pressure (PImax) after 6 weeks of respiratory muscle training plotted against change in inspiratory capacity (ΔIC, panel A), vital capacity (ΔVC, panel B) and peak expiratory cough flow (ΔPEFc, panel C) for individual participants. Blue dots represent participants in sham group and red dots represent participants in active group. Equations, R2 and p-values represent all data points.
Outcomes at 1-year follow-up
Comparison of baseline data with that collected after 1 year of unsupervised training showed no significant difference between active and sham groups in any outcome measures (table 3) except for the incidence of respiratory complications. There was a greater total number of respiratory complications during the 1-year follow-up period in the sham group (n=10) compared with the active group (n=3), p=0.017. The self-reported frequency of training and benefits of RMT and barriers that prevented participants from using RMT independently are listed in table 6.
Training frequency of participants over 1 year along with self-reported benefits of RMT and barriers preventing RMT use independently (33 participants completed survey after 1 year)
Discussion
This is the first large-scale study to demonstrate conclusively that 6 weeks of daily RMT improves inspiratory muscle strength in both acute and chronic tetraplegia. As a consequence, respiratory-related morbidity declined and QoL improved.
Inspiratory muscle strength
Six weeks of twice-daily RMT increases inspiratory muscle strength but not expiratory muscle strength in people with tetraplegia. This increase in strength occurred in people with acute and chronic tetraplegia, and regardless of the degree of injury completeness. This is supported by studies where no consistent training paradigms exist between the different study populations.21
Retrospective analysis of lung function data identified inspiratory muscle strength as the best predictor of the likelihood to develop pneumonia in individuals with tetraplegia.6 The proposed pneumonia risk threshold is based on lesion-specific reference values calculated by predictive modelling using measured absolute respiratory function values.29 For individuals with motor-complete tetraplegia, a PImax less than 115% tetraplegia-predicted have a 50% probability of suffering pneumonia. If PImax is greater than 115%, there is a 94% probability of not contracting pneumonia.6 For individuals with motor-incomplete tetraplegia, the threshold is 93.5 cmH2O. Using the predictive modelling calculator supplied,29 which is specific to an individual’s level of lesion and time since injury, the mean baseline PImax in our study for motor-complete tetraplegia are 66% tetraplegia-predicted. Post-RMT, mean PImax increased to 91% tetraplegia-predicted. Our lower than published values may be due to PImax being measured at FRC and seated, compared with residual volume in supine which can return a higher value. Despite our PImax values not reaching proposed thresholds, we did show a reduced pneumonia risk with active RMT, which increased inspiratory muscle strength. The incidence of respiratory complications over the year of our trial was three times greater in the sham group (53%) than the active group (14%). This provides evidence that RMT may reduce respiratory-related morbidity and mortality in tetraplegia.
Between 12 weeks and 1 year post-injury, 23% our participants reported a respiratory complication. However, during the first 6 weeks after injury, Jackson and Groomes30 found that 68% patients with tetraplegia developed a respiratory complication. Our participants were not recruited during this period, thus RMT in this susceptible acute stage of tetraplegia warrants further investigation to determine its effects on respiratory complications, a more important determinant of hospital costs than injury severity.31
Quality of life
Daily RMT can affect QoL in people with chronic tetraplegia. Current health status measured via the EQ-5D VAS showed the active group reported 12% improvement compared with no change for the sham group. Recent reviews21 22 indicated further research was needed into the effect of RMT on the QoL of people living with tetraplegia. This is the first study to demonstrate that RMT can improve the perceived QoL compared with sham training, although there are many factors that impact QoL over 6 weeks, thus the effect seen here may not be attributable to RMT alone. However, when questioned about current respiratory health via the SGRQ, 56% participants in the active group reported improved respiratory health compared with 27% in the sham group. Similar responses were observed for the participants with acute injuries (60% and 43%, respectively).
Respiratory symptoms
Respiratory symptoms in people with tetraplegia declined after 6 weeks of RMT. Currently, there is no validated measure to evaluate respiratory symptom severity in tetraplegia. The SGRQ is a validated measure used for respiratory diseases such as COPD24 and although many domains are not applicable to people with tetraplegia we hypothesised that the symptoms domain may be appropriate. This was measured in all participants and reflected significant improvements after RMT. Previous studies in asthma and COPD indicate that a change of 4 points of the total score of the SGRQ is clinically significant.32 As a 10-point difference between the groups was observed in symptom severity alone in the current study, this domain of the SGRQ may be a way to evaluate respiratory health in tetraplegia. An additional SGRQ question explores current respiratory health, and 58% participants in the active group and 35% participants in the sham group reported improved respiratory health post-training.
Breathlessness
The reduction in Borg scores after RMT also indicates improved symptom severity as it assesses breathlessness or perceived exertion.33 This improvement was only noted at rest, particularly for people with recent injuries. This reduction supports the commonly held idea that people with tetraplegia have dyspnoea21 34 due to the increased load on remaining intact respiratory muscles, thereby increasing the work of breathing.35 Interestingly, the Borg score during inspiratory-loaded breaths was only reduced after RMT in the chronic population, which may indicate that the muscles have adapted to the required increased work of breathing. Thus, the feeling of breathlessness during a respiratory infection could be reduced by RMT in the chronic population. Further investigations are warranted to determine if breathlessness can be ameliorated by RMT with more robust measures of dyspnoea, particularly with different degrees of inspiratory loading.
Lung function
Contrary to previous literature,22 active RMT did not improve lung volumes compared with sham RMT. However, there was a strong positive correlation between PImax and IC, VC and PEFc, which in this population with very low lung volumes and weak respiratory muscles may make a significant difference to breathlessness, the extent of atelectasis, effective mucus expectoration and the development of pneumonia. This association between increased PImax and lung function supports PImax being the strongest predictor of pneumonia in people with tetraplegia.6 Expiratory muscle training did not result in greater increases in PEmax for the active group over the sham group. This may have been due to the high number of participants with complete cervical injuries (n=41) resulting in complete paralysis of the main expiratory muscles (internal intercostals and abdominals). With no innervated muscle to train, both active and sham complete groups only increased PEmax by 1–3 cmH2O. Innervated accessory muscles of expiration (pectorals, latissimus dorsi and serratus anterior) could have increased in strength, but participants were instructed not to brace their upper limbs while performing the assessments of lung function and PEmax. For the group of participants with an incomplete injury (n=21), the small resistance of the sham tube and the manoeuvre of 36–60 exhalations twice daily may have been enough training to increase the PEmax group mean by 8–10 cmH2O in both the active and sham groups. This would indicate that the active training intensity was no more effective than sham training intensity. The possible reasons for the lack of significant changes in lung volume despite increases in PImax may be (1) long-term changes in chest wall stiffness, which have not reduced with training and (2) partial atelectasis, which prevents increases in lung volume. These hypotheses are yet to be tested.
Training
Recruitment ceased at 62 participants, rather than the target sample size of 80, due to funding but this had little effect on statistical precision because the sample size of 80 allowed for a 20% dropout rate. The active group trained at a ‘moderate’ to ‘somewhat-severe’ intensity (Borg score 3–4) which was the designated a priori perceived level of exertion. Training at a moderate level of effort is consistent with training intensities used for exercise groups and cardiovascular training. The protocol indicated that the maximal training intensity was capped at 80% weekly measured PImax or PEmax. The training protocol was achieved by the active group, but did not reach maximal. Active group participants commenced training at 30%/40% and progressed to maximal training pressures of 80%/83% baseline PImax/PEmax, respectively. The sham group’s actual training intensity was maintained between 8% and 13% baseline PImax/PEmax, and their perceived training effort was a ‘very-slight’ to ‘slight’ intensity (Borg score 1–2). The work performed by the active group was significantly higher and supports the progressive training paradigm was suitable to achieve a training effect for inspiratory muscles, however ineffective for expiratory. Recent pilot studies investigating progressive RMT36 37 also showed this training paradigm to be feasible and effective in people with tetraplegia. The frequency of the training was supervised twice daily and labour intensive. Recent studies of RMT in healthy populations have indicated that three sessions of training per week were as effective as five times a week.38 The intensive frequency of training in this trail may have resulted in the poor compliance when individuals were encouraged to continue training after 6 weeks.
One-year follow-up
The loss to follow-up after 1 year was high for this study, and only 62% of participants agreed to reassessment (figure 1). Only 48% people contacted had continued training independently after the initial 6 weeks. These participants were able to continue training with carer or family assistance or had sufficient hand function to train independently. However, despite being asked to record training frequency and intensity, participants found this too burdensome on top of the training and usual daily activities. Common reasons for not continuing RMT independently included lack of time, self-reported laziness, forgetfulness and poor hand function to use without carer assistance. Of those contacted, 84% reported benefits of RMT including increased strength, improved breathing and feeling better as they felt there was more air in their lungs. The 53% incidence of respiratory-related morbidity or mortality in the sham group is triple the incidence in the active group (14%), thus continued RMT regardless of the training intensity may reduce respiratory complications.
Strengths and limitations
This is the first study of RMT in tetraplegia with a high number of participants which are retained at the primary endpoint. The addition of examining QoL, respiratory symptoms and the number of respiratory complications are relevant clinical implications for people with tetraplegia. The relatively high loss to follow-up after 1 year is a limitation as it may have contributed to a positive selection bias for the number of respiratory complications during this year. However, there were still differences in the QoL and respiratory symptom measures between active and sham groups. Some participants with higher near-normal initial PImax may not have trained with a high enough resistance as the training device is restricted in the maximal level of resistance it can provide. Despite this, PImax still increased for the active group. In practice, people with a higher initial PImax may benefit from a device which can deliver higher levels of resistance. This study has also highlighted, through the lack of independent training in the 1 year follow-up, that unless training is incorporated into routine care it is unlikely that people will be able to maintain a beneficial RMT regimen.
Conclusion
Progressive RMT over 6 weeks increases inspiratory muscle strength in people with tetraplegia, irrespective of time since injury and degree of injury completeness. This training paradigm improves respiratory symptom severity, reduces respiratory-related incidence, breathlessness at rest for those with recently acquired injuries and QoL for those people with a longer-standing injury. RMT should be implemented as a routine therapy for people with tetraplegia. The use of RMT to reduce respiratory-related mortality and morbidity has potential and could be further investigated after clinical roll out.
Acknowledgments
The authors acknowledge Professor Rob Herbert for his statistical advice, Paraquad and Ferguson Lodge for their assistance with recruitment, Katlyn Anderson for data entry and also acknowledge all participants for their contributions to the study.
References
Footnotes
CLB-R and CRHL are joint first authors.
Contributors All authors contributed equally.
Funding This trial was supported by grants from the National Health and Medical Research Council (NHMRC) and The Prince of Wales Hospital Foundation (POWHF). The NHMRC and POWHF had no role in the design of the study nor the collection, analysis and interpretation of data or in writing the manuscript.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval New South Wales Government Health, South Eastern Sydney Local Health District, Human Research Ethics Committee, HREC Ref No: 12/192 (LNR/12/POWH/409). University of New South Wales, Human Research Ethics Committee, HREC Ref No: HC13388.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request from the corresponding author.