Article Text

Abstract
BACKGROUND Airway hyperresponsiveness, induced sputum eosinophils, and exhaled nitric oxide (NO) levels have all been proposed as non-invasive markers for monitoring airway inflammation in patients with asthma. The aim of this study was to compare the changes in each of these markers following treatment with inhaled glucocorticosteroids in a single study.
METHODS In a randomised, double blind, placebo controlled, parallel study 25 patients with mild asthma (19–34 years, forced expiratory volume in one second (FEV1) >75% predicted, concentration of histamine provoking a fall in FEV1 of 20% or more (PC20) <4 mg/ml) inhaled fluticasone propionate (500 μg twice daily) for four weeks. PC20 to histamine, sputum eosinophil numbers, and exhaled NO levels were determined at weeks 0, 2, and 4, and two weeks after completing treatment. Sputum was induced by inhalation of hypertonic (4.5%) saline and eosinophil counts were expressed as percentage non-squamous cells. Exhaled NO levels (ppb) were measured by chemiluminescence.
RESULTS In the steroid treated group there was a significant increase in PC20, decrease in sputum eosinophils, and decrease in exhaled NO levels compared with baseline at weeks 2 and 4 of treatment. Subsequently, each of these variables showed significant worsening during the two week washout period compared with week 4. These changes were significantly different from those in the placebo group, except for the changes in sputum eosinophils and exhaled NO levels during the washout period. There were no significant correlations between the changes in the three markers in either group at any time.
CONCLUSIONS Treatment of asthmatic subjects with inhaled steroids for four weeks leads to improvements in airway hyperresponsiveness to histamine, eosinophil counts in induced sputum, and exhaled nitric oxide levels. The results suggest that these markers may provide different information when monitoring anti-inflammatory treatment in asthma.
- airway hyperresponsiveness
- asthma
- fluticasone propionate
- inhaled corticosteroids
- nitric oxide
- induced sputum
Statistics from Altmetric.com
- airway hyperresponsiveness
- asthma
- fluticasone propionate
- inhaled corticosteroids
- nitric oxide
- induced sputum
Asthma is an inflammatory disease of the airways associated with airway hyperresponsiveness to various bronchoconstrictor stimuli such as histamine.1 The accompanying inflammation is characterised by the presence of inflammatory cells such as T lymphocytes, neutrophils and eosinophils and their cytokines in the airway mucosa, as demonstrated in bronchial biopsy specimens.2 ,3 The current treatment of asthmatic patients is based on the belief that reducing airway inflammation is essential, and that control of such inflammation can be indirectly assessed by optimising symptoms and lung function.1 ,4 However, monitoring airway inflammation more closely by measurement of non-invasive and sensitive markers of inflammation, such as airway hyperresponsiveness,5 sputum eosinophils,6 or exhaled NO levels,7 may provide additional information for assessing asthma control.
Inhaled glucocorticosteroids are currently the most effective treatment for asthma, not only reducing symptoms and airway hyperresponsiveness8 but also leading to an improvement in airway inflammation.9 However, recent evidence has suggested that such treatment often provides only partial suppression of airway inflammation, as shown by persisting eosinophilic inflammation in the bronchial (sub)mucosa after long term inhaled steroid treatment in some patients.5
Among the non-invasive techniques, hypertonic saline induced sputum has been shown to be a reliable method for measuring eosinophilic airways inflammation.6 ,10 ,11 The number of eosinophils in sputum is associated with asthma severity10 and decreases following treatment with inhaled steroids.12 In addition, nitric oxide levels in exhaled air have also been proposed as a marker for disease severity in asthma.7 ,13 Indeed, inhaled glucocorticosteroids decrease the levels of exhaled NO in patients with asthma14 in a dose dependent way.15
Although the effects of inhaled steroids on sputum eosinophils and exhaled NO have been well established, comparative analysis is required before any of these markers can be recommended in the monitoring of asthma treatment. In the present study we investigated treatment induced changes in airway hyperresponsiveness, sputum eosinophils, and exhaled NO levels in asthma. To that end we performed histamine challenge, induced sputum, and exhaled NO measurements before, during, and after four weeks of treatment with fluticasone propionate or placebo in steroid naive patients with asthma.
Methods
SUBJECTS
Twenty five non-smoking atopic patients (16 men, age range 19–34 years) with mild persistent asthma1 volunteered to participate in the study (table 1). Symptoms of episodic chest tightness and wheezing were treated by on-demand usage of inhaled salbutamol alone, which was discontinued at least eight hours before the measurements. Two weeks before the study all subjects were free from symptoms of respiratory tract infection. Atopy was indicated by a positive skin prick test (>3 mm weal) to one or more of 10 common airborne allergen extracts (Vivodiagnost, ALK, The Netherlands). The forced expiratory volume in one second (FEV1) was more than 75% of the predicted value16 and all subjects were hyperresponsive to inhaled histamine (provocative concentration causing a fall in FEV1 of 20% or more (PC20) of <4 mg/ml).17 The study was approved by the medical ethics committee of the Leiden University Medical Center and written informed consent was obtained from all volunteers.
Characteristics of the subjects
DESIGN OF STUDY
The study was of a randomised, double blind, placebo controlled, parallel design. During screening the selection criteria were checked for all subjects. Before entering the treatment period baseline values of PC20 histamine and percentage eosinophils in induced sputum were determined. These two measurements were carried out on two separate days with a 2–4 day interval between them. Prior to histamine challenge and sputum induction, baseline values of FEV1 and exhaled NO were recorded. This sequence of measurements was used at all time points during the study.
Immediately after the second baseline visit the subjects were treated with inhaled fluticasone propionate (500 μg twice daily) or placebo for a period of four weeks. The measurement of PC20histamine, sputum eosinophils, FEV1, and exhaled NO were repeated during the treatment period (at weeks 2 and 4) and during the washout period at two weeks after the treatment period.
HISTAMINE CHALLENGE
Histamine challenges were performed according to a standardised methodology.17 Histamine-di-phosphate (Sigma Chemicals, St Louis, MO, USA) in phosphate buffered saline (PBS) was stored at 4°C and administered at room temperature. Doubling concentrations between 0.06 and 16 mg/ml were used. The aerosols were generated by a DeVilbiss 646 nebuliser (output 0.13 ml/min), connected to an inspiratory and expiratory valve box with an expiratory aerosol filter (Pall Ultipor BB50T). Each dose was inhaled through the mouth by tidal breathing for two minutes at five minute intervals with the nose clipped.17
The airway responses to the inhaled aerosols were measured using FEV1, recorded by a dry rolling seal spirometer (Morgan Spiroflow, Morgan UK) and monitored on-line by a personal computer with a special software program. Before each test FEV1 was measured in triplicate for calculation of mean baseline levels.17 The airway response was recorded at 30 and 90 seconds after each dose. After each inhalation the lowest technically satisfactory FEV1 value was applied in the analysis to calculate the percentage fall in FEV1 from baseline. The test was discontinued if FEV1 decreased by 20% or more. The PC20 was calculated by log-linear interpolation of the final two data points.
SPUTUM INDUCTION
Sputum was induced and processed by the so called full sample method18 according to a protocol that has been validated in our laboratory.6 Hypertonic saline aerosols (NaCl 4.5%) were generated at room temperature by a DeVilbiss Ultraneb 2000 ultrasonic nebuliser with a calibrated particle size (MMAD 4.5 μm) at maximal output (2.5 ml/min). The aerosols were administered to the subjects through a 100 cm long tube with an internal diameter of 22 mm and inhaled via the mouth through a two way valve (No. 2700; Hans-Rudolph, Kansas City, MO, USA) with the nose clipped. Before inhalation of the aerosols baseline FEV1 was recorded and, for safety reasons, 400 μg salbutamol was administered through a metered dose inhaler (Volumatic). The subjects then inhaled hypertonic saline aerosols during 2 × 5 minute and 1 × 10 minute intervals. After each inhalation, or as soon as the subjects started coughing, they were asked to blow their nose, to rinse their mouth and throat with water, and to expectorate sputum into a clean plastic container by coughing. After testing, FEV1 was measured and salbutamol was administered if needed.
SPUTUM PROCESSING AND CELL DIFFERENTIAL COUNTS
The volume of the induced sputum samples was determined and mixed with an equal volume of 0.1% sputolysin (dithiotreitol, Calbiochem, USA).6 To ensure complete homogenisation the samples were placed in a shaking water bath at 37°C for 15 minutes and then gently mixed. The homogenised sputum was centrifuged (350g) for 10 minutes at room temperature. The cell pellet was resuspended in PBS to a final volume of 2–5 ml, then filtered through a gauze (pore size approximately 1 mm) to remove clumps. Total cell counts were performed in a haemacytometer (Tamson, Zoetermeer, The Netherlands). The sample was then diluted with PBS to a final concentration of ±0.3 × 106 cells/ml which was used for preparation of the cytocentrifuge slides (1500 rpm, three minutes, 50 μl/slide; Shandon 3, Life Sciences International, Veldhoven, The Netherlands).
Differential counts of eosinophils, neutrophils, lymphocytes, macrophages, epithelial and squamous cells were performed on Diff-Quik stained cytospins by a qualified cytopathologist. To correct for the variable salivary contamination, differential leucocyte and cylindrical epithelial cell counts were expressed as a percentage of 250 nucleated cells, excluding squamous cells. For each sample differential cell counts were performed twice by the same observer and the mean values were used in the analysis. A sputum sample was considered adequate when the percentage squamous cells was less than 80%. The reproducibility of the sputum cell counts obtained by this method has been shown to be satisfactory.6 To ensure a blind analysis of the sputum samples all cytocentrifuge slides were coded before analysis by an investigator who was not involved in the counting.
EXHALED NO
Exhaled NO levels were measured by a chemiluminescence analyser (Sievers NOA 270B) according to a standardised procedure7which has previously been used by our laboratory.19 The subjects were connected to a closed system to avoid contamination of the measurements with ambient NO. Pressurised air with a low NO concentration (<1 ppb) was administered through a 150 litre reservoir connected to the inspiratory side of a Hans-Rudolph three way valve. The subjects performed a slow vital capacity manoeuvre with a constant expiratory flow of 10 l/min against an expiratory resistance of 3–4 cm H2O. The expiratory NO concentration was sampled continuously from the centre of the mouthpiece at a flow rate of 440 ml/min and the average concentration (in parts per billion; ppb) was determined for a period of 10 seconds.7 Baseline values of exhaled NO were obtained from the mean values of the two NO measurements recorded before histamine challenge and sputum induction because their reproducibility was good (intraclass correlation coefficient, R i >0.92).
ANALYSIS OF DATA
PC20 was log transformed before statistical analysis and expressed as geometric mean (SD) doubling doses. Based on their close to normal distribution, the percentage of eosinophils in sputum and the levels of exhaled NO were expressed as mean (SD). To test for differences between and within the treatment groups in general, multivariate analysis of variance (MANOVA) was applied for FEV1 and log PC20, whilst the Kruskal-Wallis test was used for sputum eosinophils and exhaled NO. The changes in PC20 (expressed in doubling doses), sputum eosinophils, and exhaled NO levels within each treatment group were analysed using the Student’s paired t test whilst changes in PC20, sputum eosinophils, and exhaled NO levels between both groups were tested using the Student’s unpairedt test, providing the 95% confidence intervals (95% CI). Finally, Pearson correlation analysis was used to examine the relationship between the changes in PC20, sputum eosinophils, and exhaled levels of NO. The results were considered significant if the p value was <0.05. All statistical analyses were performed using the SPSS program.
Results
Three of the subjects dropped out during the washout period between weeks 4 and 6 because of a history of respiratory tract infection (nos 5 and 6) or because they were taking an antihistamine (no. 11). Three subjects (nos 9, 18 and 23) did not produce adequate sputum at baseline, whilst subjects 21 and 7 were not able to produce sputum at week 2 and week 4, respectively. These time points were handled as missing data.
LUNG FUNCTION AND HISTAMINE CHALLENGE
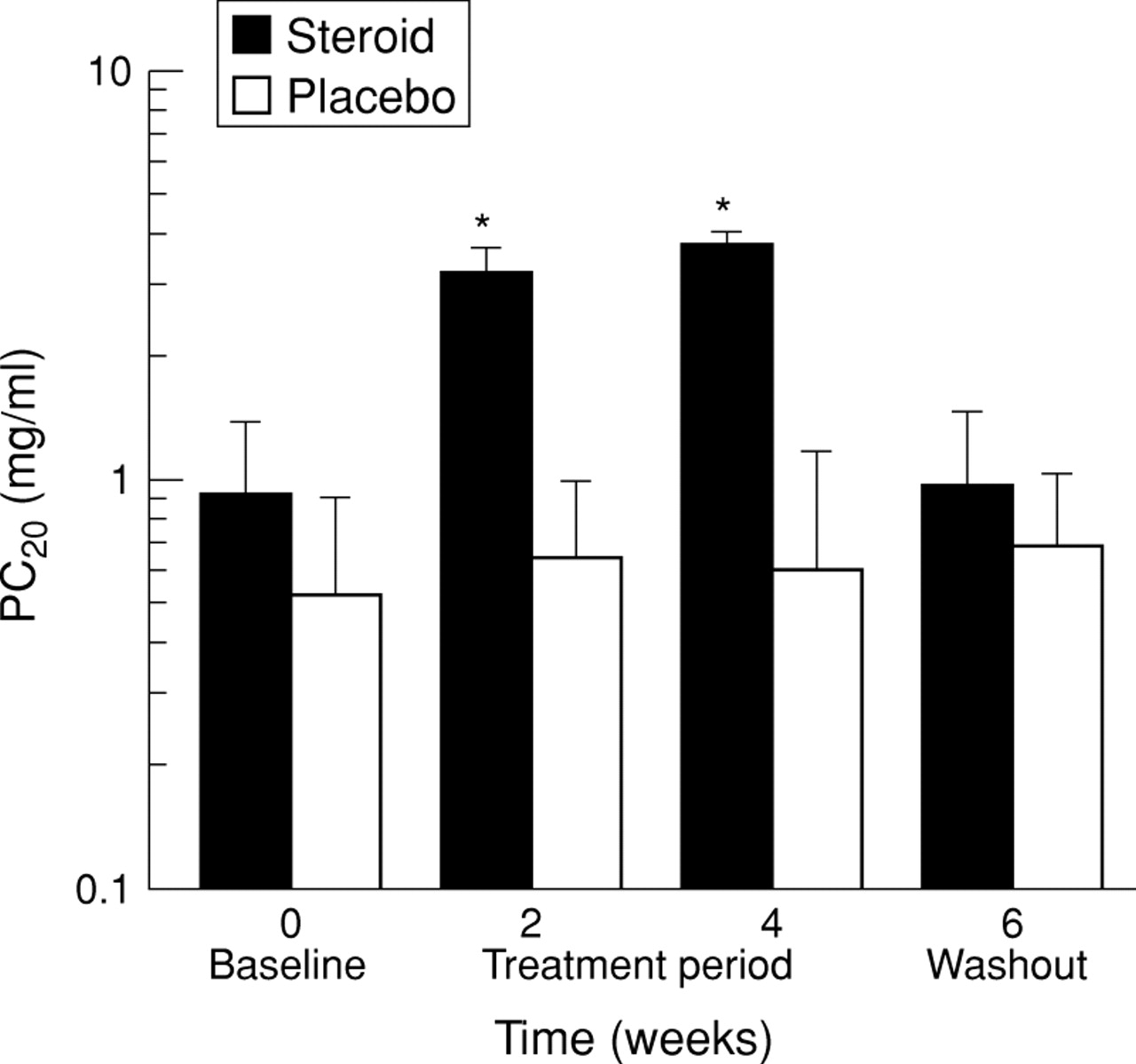
At baseline there were no significant differences in FEV1 and PC20 between the groups (p>0.19; table 1). During the study there were no significant changes in FEV1 in the two groups (p>0.96, MANOVA). In the placebo group there were no significant changes in PC20 (p = 0.92, MANOVA) while in the steroid treated group PC20 increased significantly at week 4 compared with baseline values (mean change 2.01 (95% CI 0.683 to 2.090); p = 0.001; fig 1). After a two week washout period PC20 decreased again compared with week 4 by –1.75 (–1.831 to –0.582) doubling doses (p = 0.002; table 2, fig 1). These changes were significantly different from the changes in the placebo group (p<0.003; table 3).

Airway hyperresponsiveness to histamine (PC20) at baseline, at weeks 2 and 4 of treatment, and after two weeks of washout in the steroid treated (closed bars) and placebo groups (open bars) shown as geometric mean doubling doses; *significant difference between the two groups.
Airway hyperresponsiveness, sputum eosinophils and exhaled nitric oxide (NO) levels during and after steroid and placebo treatment
Changes in airway hyperresponsiveness, sputum eosinophil counts, and exhaled NO levels between steroid and placebo treatment groups
SPUTUM EOSINOPHILS
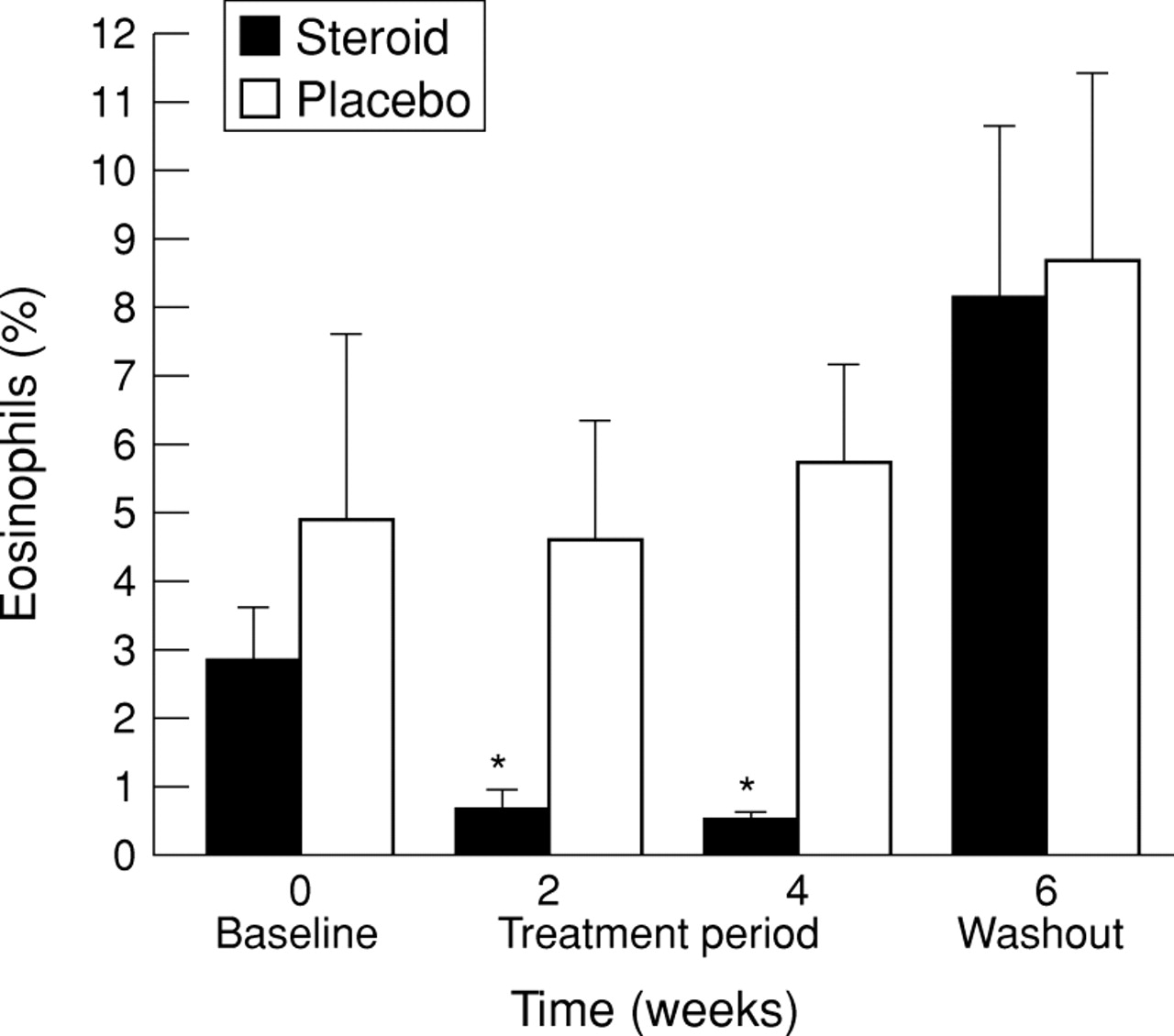
The mean (SD) percentage of squamous cells in this study was 33.4 (17.6)%. Baseline sputum eosinophils were not significantly different in the two groups (p = 0.31; table 1). There were no significant changes in sputum eosinophils within the placebo group (p = 0.85, MANOVA), but in the steroid treated group a significant decrease in sputum eosinophils was observed compared with baseline values (mean change at week 4 –2.46 (95% CI –4.260 to –0.660)%; p = 0.01) with a subsequent worsening in the washout period compared with week 4 (mean change 6.13 (95% CI 0.804 to 11.459)%; p = 0.03; table 2, fig 2). The changes in sputum eosinophils were not significantly different between the two groups when baseline values were compared with week 4, or week 4 values were compared with those in the washout period (table3).

Mean eosinophil counts in induced sputum at baseline, at weeks 2 and 4 of treatment, and after two weeks of washout in the steroid treated (closed bars) and placebo groups (open bars); *significant difference between the two groups.
EXHALED NO
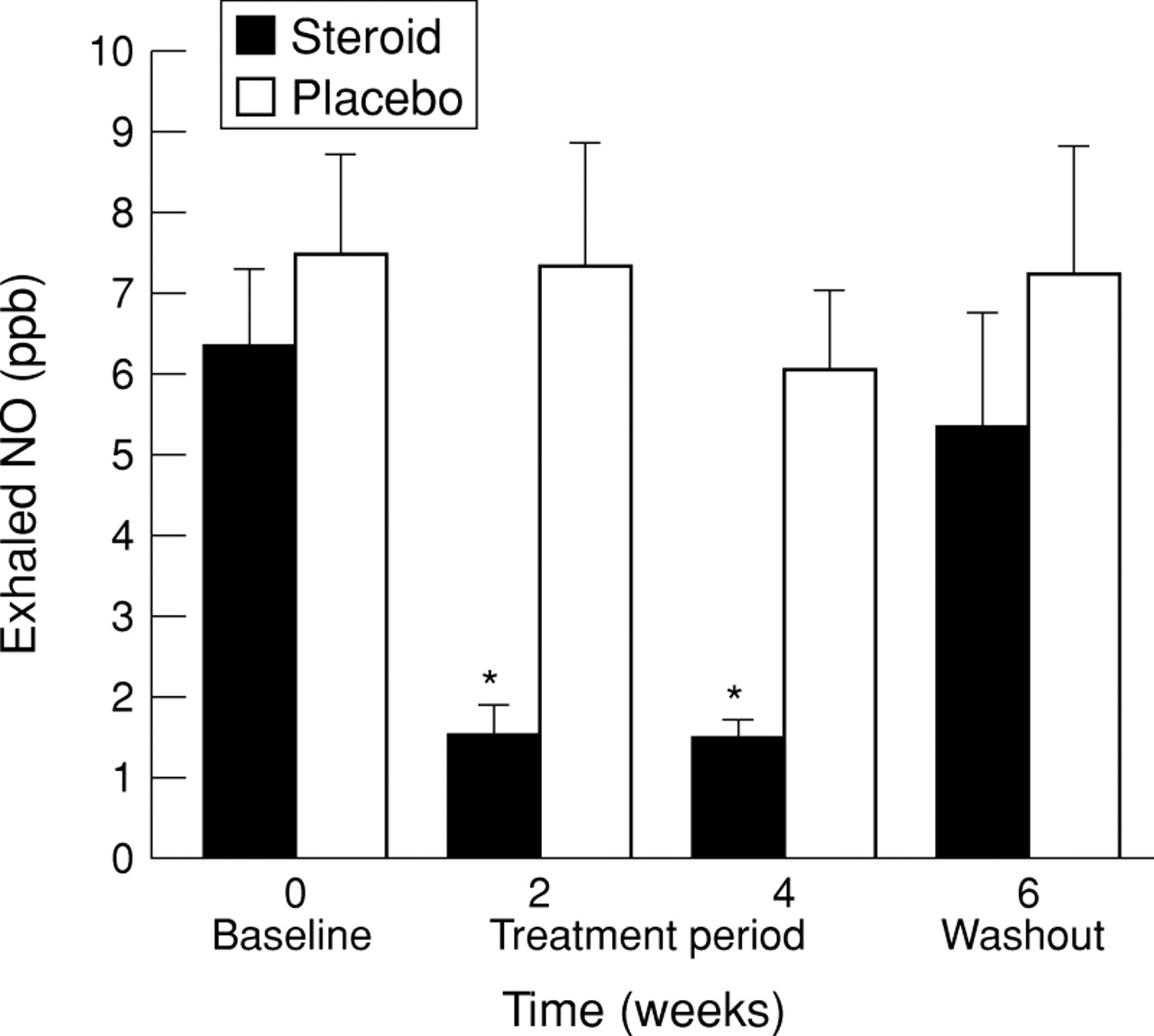
At baseline exhaled NO levels were not significantly different in the two groups (p = 0.55; table 1). During the study there were no significant changes in exhaled NO levels in the placebo group (p = 0.54, MANOVA; table 2) but in the steroid treated group the levels of exhaled NO decreased significantly at week 4 compared with baseline values with a mean change of –4.88 (95% CI –6.862 to –2.892) ppb (p < 0.001), with a subsequent increase during the washout period compared with week 4 of 3.65 (95% CI 0.882 to 6.423) ppb (p = 0.016; table 2, fig 3). These changes in exhaled NO levels were significantly different from the changes in the placebo group between baseline and week 4 (p = 0.005; table 3).

Mean levels of exhaled nitric oxide (NO) at baseline, at weeks 2 and 4 of treatment, and after two weeks of washout in the steroid treated (closed bars) and placebo groups (open bars); *significant difference between the two groups.

Relationship between the change in sputum eosinophils and the change in PC20 histamine at week 4 compared with baseline (• steroid group; ○ placebo group).

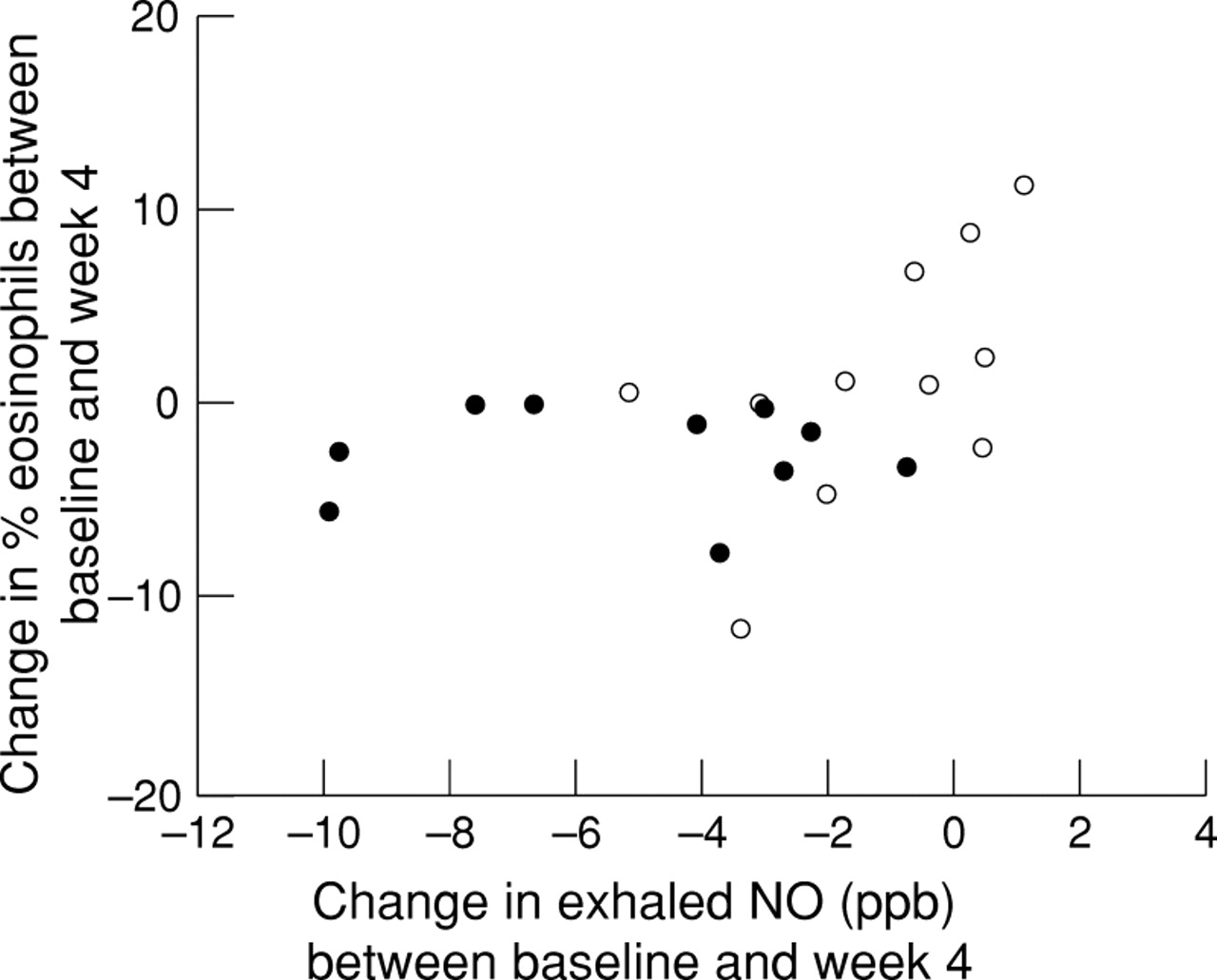
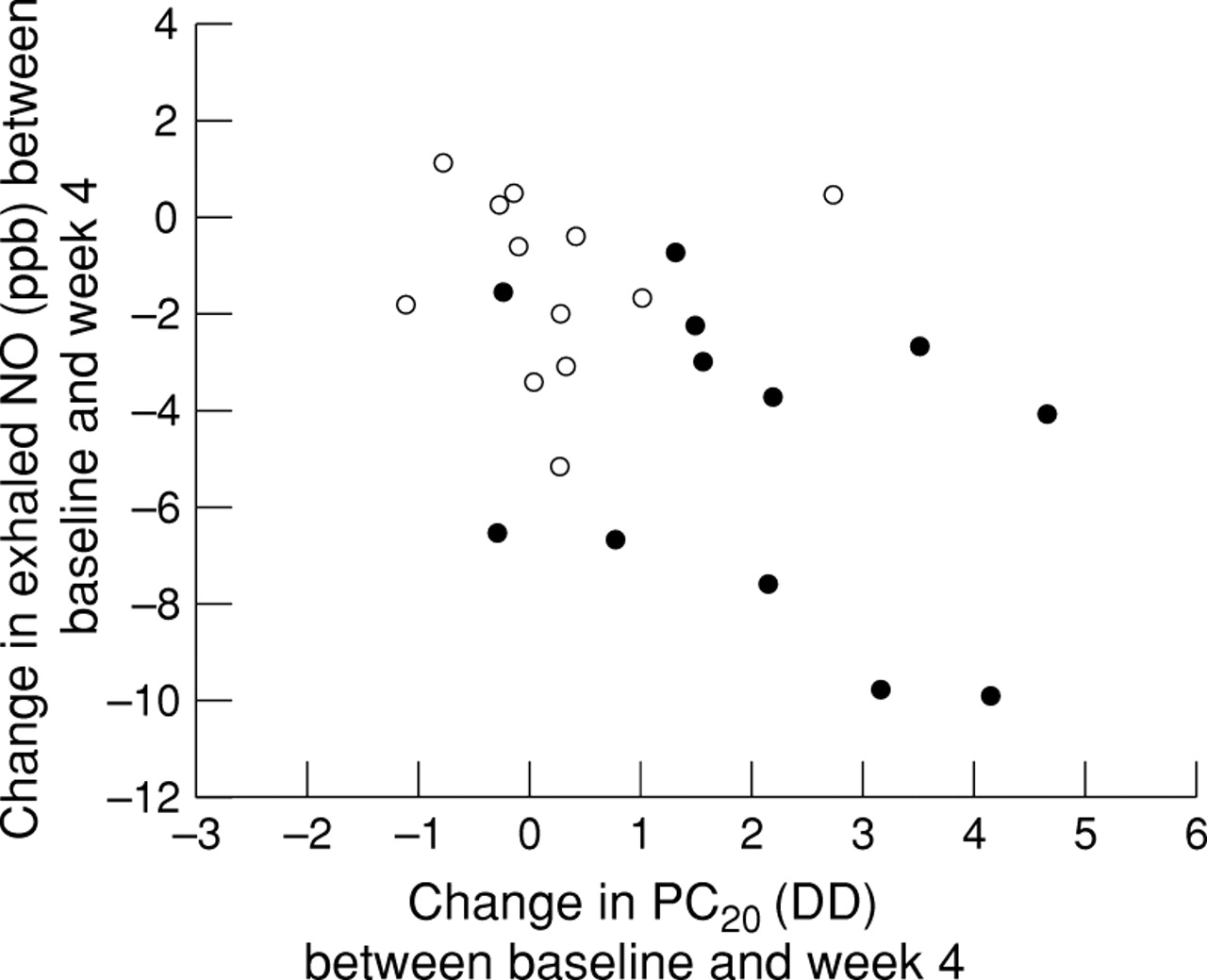
Relationship between the change in exhaled NO levels and the change in PC20 histamine at week 4 compared with baseline (• steroid group; ○ placebo group).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relationship between the change in sputum eosinophil numbers and the change in exhaled NO levels at week 4 compared with baseline (• steroid group; ○ placebo group).
RELATIONSHIPS BETWEEN CHANGES IN PARAMETERS
Within the steroid group there were no significant correlations between the changes in PC20, sputum eosinophils, and exhaled NO at any time point (Pearson’s r<0.56, p >0.15; figs 4-6).
Discussion
The results of this study indicate that four weeks of treatment with inhaled steroids leads to improvements in airway hyperresponsiveness, sputum eosinophil numbers, and levels of exhaled NO in patients with mild atopic asthma. In addition, it appears that the improvements in these markers are lost two weeks after cessation of treatment. This suggests that each of these markers may be useful for monitoring patients with asthma, even though there might be small differences between the markers in their earliest response to anti-inflammatory treatment.
To our knowledge this is the first study to compare the treatment induced changes in airway hyperresponsiveness to histamine, eosinophil counts in induced sputum, and exhaled NO levels in a group of asthmatic patients. Our study confirms and extends the results of others who have shown the beneficial effect of glucocorticosteroids on each of these markers separately. Like Kraan et al, we found an improvement of two doubling doses in airway hyperresponsiveness after four weeks of treatment with inhaled steroids.20 Furthermore, our findings are in agreement with those of Keatings et al 12and Kharitonov et al 14 who demonstrated a decrease in sputum eosinophils and exhaled NO levels, respectively, after treatment with inhaled steroids.
Although cross sectional relationships between airway hyperresponsiveness, sputum eosinophils, and exhaled NO levels in patients with asthma have been reported previously,10 ,21only limited data are available on the comparison of within subject changes in these markers during treatment follow up. Our results are in agreement with those of Baraldi et al who also failed to find a correlation between steroid induced changes in PD20 and sputum eosinophils.22 The absence of such relationships may reflect the partially distinct pathophysiological backgrounds of these markers and might indicate the possible independent complementary clinical information during anti-inflammatory therapy.
We do not believe that our data were influenced by measurement errors since we used validated and reproducible methods.6 ,7 ,17 ,19 All subjects in the study were carefully selected as non-smokers with stable atopic asthma who had not used inhaled steroids for at least one month prior to the study. We chose a relatively high dose of inhaled steroid to ensure an optimal anti-inflammatory effect. To avoid carryover effects the histamine challenge for determination of PC20 and the sputum induction were separated by 2–4 days. Furthermore, exhaled NO levels on these two days appeared to be highly reproducible. Our inability to show a significant improvement in lung function following steroid treatment may be due to the normal baseline levels of FEV1in our study (77–111% of the predicted value).
How can the present findings be interpreted? Firstly, corticosteroids are likely to decrease the percentage of eosinophils in the sputum by reducing the release and subsequent effects of cytokines such as interleukin 5 (IL-5) and granulocyte-macrophage colony-stimulating factor (GM-CSF) on eosinophil infiltration and survival.23-25 Secondly, the steroid induced reduction in exhaled NO levels can be explained by the inhibition of inducible NO synthase (iNOS) expression directly and/or indirectly by reduction in the levels of stimulatory cytokines, for instance in epithelial cells.26 Finally, the improvement in the physiological marker PC20 is likely to be due to effects of steroids on the presence and activity of multiple (infiltrative and resident) cells.5 ,8 ,9 ,27 Hence, it may not be surprising that the steroid induced changes in the three markers were not significantly correlated with each other. It would appear that early improvement of eosinophils in sputum in response to steroid treatment is somewhat out of phase with the other two markers. However, we believe that this has few implications, given the consistency in the changes between the markers after four weeks of treatment.
What are the clinical implications of the present findings? Treatment according to the current guidelines is based on minimising symptoms and optimising lung function.1 However, frequently this fails to provide complete suppression of airway inflammation.5It has been postulated that persistent airway inflammation in asthma leads to airway remodelling and an irreversible loss of lung function.28 ,29 This may require the use of more direct markers for monitoring airway inflammation.10 ,30 Indeed, a recent study by Sont et al showed that the adjustment of long term inhaled steroid treatment, additionally guided by the level of airway hyperresponsiveness, leads to a significantly better clinical, as well as histological, outcome than treatment guided by symptoms and lung function alone.31 Based on the present data, it is now necessary to determine in long term prospective trials whether monitoring sputum eosinophils and/or exhaled NO levels can provide similar benefits in the management of asthma.
Acknowledgments
The authors thank all the volunteers who participated in this study and Glaxo Wellcome, The Netherlands, for supporting the study with a grant for material expenses.