Article Text

Abstract
Background Inhaled corticosteroid (ICS) use could decrease local immunity of the lung. Concerns have been raised regarding the risk of tuberculosis (TB) development among ICS users. The aim of this study was to elucidate the association between ICS use and development of TB among patients with various respiratory diseases in South Korea, an intermediate-TB-burden country.
Methods A nested case-control study based on the Korean national claims database was performed. The eligible cohort consisted of 853 439 new adult users of inhaled respiratory medications between 1 January 2007 and 31 December 2010. Patients diagnosed as having TB after initiation of inhaled medication were included as cases. For each case individual, up to five control individuals matched for age, sex, diagnosis of asthma or chronic obstructive pulmonary disease (COPD) and initiation date of inhaler use were selected.
Results From the cohort population, we matched 4139 individuals diagnosed as having TB with 20 583 controls. ICS use was associated with increased rate of TB diagnosis (adjusted OR (aOR), 1.20; 95% CI 1.08 to 1.34). The association was dose dependent (p for trend <0.001). A subgroup analysis revealed that ICS use increased the risk of TB development among non-users of oral corticosteroid (OCS) but not among OCS users.
Conclusions ICS use increases the risk of TB in an intermediate-TB-burden country. Clinicians should be aware of the possibility of TB development among patients who are long-term high-dose ICS users.
- Tuberculosis
Statistics from Altmetric.com
Key messages
What is the key question?
-
We tried to elucidate the association between inhaled corticosteroid (ICS) use and development of tuberculosis (TB) in South Korea, an intermediate-TB-burden country.
What is the bottom line?
-
ICS use could decrease the local immunity of the lung. Recently, an increased risk of TB development among ICS users was suggested in an analysis of a cohort based in Canada, where the prevalence of TB is low.
Why read on?
-
ICS use dose-dependently increases the risk of TB in South Korea, an intermediate-TB-burden country. Clinicians should be aware of the possibility of TB development among patients who are long-term high-dose ICS users.
Introduction
Among infectious diseases, tuberculosis (TB) is one of the leading causes of mortality and morbidity worldwide. In 2010, 8.8 million new cases, 1.1 million deaths among HIV-negative people and 0.35 million deaths among HIV-positive people with TB were reported.1
A considerable proportion of active TB results from reactivated latent infection, although this proportion varies geographically.2 ,3 Among patients with latent TB infection (LTBI), groups at high risk for development of active TB include: those with advanced HIV infection; those with lesions suggesting old, healed TB on chest radiographs; those with chronic renal failure; those who have undergone anti-tumour necrosis factor (TNF)α treatment; those with poorly controlled diabetes; those with silicosis; those who are underweight (>10% below normal); and those who have undergone gastrectomies.4
Inhaled corticosteroids (ICSs), one of the most frequently used forms of inhaled respiratory medication for chronic airway diseases, including chronic obstructive pulmonary disease (COPD) and asthma, could decrease local immunity of the lung.5 In fact, several studies and meta-analyses have found increased risks for pneumonia6–9 among patients with COPD who use ICSs. Meanwhile, concerns have been raised regarding the risk of TB development among ICS users.10–12 Recently, an increased risk of TB development among ICS users was suggested in an analysis of a cohort based in Canada.13 However, the majority of ICS users were unlikely to have had LTBI, because the incidence of TB is as low as 4.7 cases per 100 000 population per year in Canada.1 Considering that ICS users without LTBI could not have developed reactivated TB, the potential impact of ICS use might be underestimated in that study.14
In this context, we evaluated the association between ICS use and development of TB in patients with various respiratory diseases in South Korea, where the incidence of TB is 97 cases per 100 000 population per year, using the Health Insurance Review and Assessment Service database, which includes almost all South Koreans.1
Methods
Source of data
We used the database of the Health Insurance Review and Assessment Service (HIRA; Seoul, South Korea), a government-affiliated agency responsible for examining the accuracy of claims for National Health Insurance (NHI, which covers approximately 96.6% of the entire 48.6 million population of South Korean) and National Medical Aid (covering approximately 3.5% of the South Korean population). The NHI database includes the entire South Korean population as well as registered foreign-nationality residents as a compulsory insurance system, with exceptions for cases applicable to the National Medical Aid programme or foreign military personnel.15 The HIRA database contains information on demographics and all medical services rendered, along with the diagnostic code (as per International Statistical Classification of Diseases and Related Health Problems, 10th edition (ICD-10) code) and all prescription medications dispensed. Values in key fields such as drug name(s), quantity, date dispensed and duration are missing or out of range in <0.5% of records. These databases have been used in previous studies.16–19
Study design
A nested case-control study based on the HIRA database was conducted. The source population consisted of all individuals who were dispensed at least one of the following inhaled respiratory medications between 1 January 2007 and 31 December 2010: ICSs, (beclomethasone, budesonide, triamcinolone, ciclesonide, fluticasone, or flunisolide), short-acting inhaled β2 agonists (SABAs; salbutamol, fenoterol, procaterol, or terbutaline), long-acting inhaled β2 agonists (LABAs; salmeterol or formoterol), short-acting inhaled muscarinic antagonists (SAMAs; ipratropium), long-acting inhaled muscarinic antagonists (LAMAs; tiotropium), a combination of a SABA and SAMA (ipratropium/salbutamol), or a combination of a LABA and ICS (budesonide/formoterol, fluticasone/salmeterol).
An eligible cohort of new users of inhaled respiratory medication was identified from all individuals who had a prescription for an inhaled respiratory medication for 30 days or longer between 1 January 2007 and 31 December 2010. The date of the first use of the above inhaled respiratory medications was considered the initiation date. Individuals who had a prescription for inhaled respiratory medication for 30 days or longer or who had any of the ICD-10 codes covering TB (A15–A19, U88.0–U88.1) within the year prior to the initiation date were excluded. Additionally, individuals <20 years of age or of unknown age were excluded. The eligible individuals were monitored until the diagnosis of TB or until 31 December 2010.
The protocol of the present study was approved by the ethics review committee of the National Evidence-based Healthcare Collaborating Agency, Seoul, Republic of Korea.
Case definition
Within the eligible cohort, we identified cases with TB that occurred after the initiation date of the inhaled respiratory medications. TB was defined if ICD-10 diagnoses of TB (A15–A19, U88.0–U88.1) and two or more of following anti-TB drugs were prescribed in 90 days: simultaneously prescribed isoniazid and rifampicin (considered as one anti-TB drug), ethambutol, pyrazinamide, prothionamide, para-aminosalicylate and cycloserine. The index date was defined as the date of first assignment of an ICD-10 code for TB.
Control individuals
For each case individual, up to five control individuals, who were randomly matched for age (within 1 year), sex, diagnosis of asthma (J45–J46) or COPD (J41–J44) and initiation date (within 15 days), were selected without replication from among individuals without an ICD-10 diagnosis of TB. The index date for the controls was defined as the index date for their matched case.
Inhaled corticosteroid exposure
ICSs included orally inhaled beclomethasone, budesonide, ciclesonide and fluticasone, whether dispensed alone or in a combination inhaler with an inhaled β2 agonist. An ICS user was defined if ICS prescriptions for 30 days or longer were identified during the 1-year period before the index date. If the ICS prescriptions were for less than 30 days during the 1-year period before the index date, patients were regarded as non-users.
Equivalencies were estimated based on relative topical potency and what experts considered to be comparable doses according to the National Asthma Education and Prevention Programme Expert Panel report 3,20 the Canadian Asthma Consensus Statement,21 and the Global Strategy for Asthma Management and Prevention 2010 (updated).22 Accordingly, the equivalent doses for ICS were 100 µg beclomethasone, 50 µg beclomethasone HFA, 80 µg budesonide, 200 µg triamcinolone, 32 µg ciclesonide, 50 µg fluticasone and 200 µg flunisolide. All doses were converted to fluticasone equivalents. Cumulative dose was calculated for ICS use during the 1-year period before the index date.
Oral corticosteroid exposure
An OCS user was defined as an individual who took a cumulative dose of 1680 mg (60 mg daily for 4 weeks) of hydrocortisone equivalents or more during the 1-year period before the index date was identified. The OCS prescriptions were converted to hydrocortisone using the following equivalent doses: 20 mg hydrocortisone (cortisol), 25 mg cortisone, 5 mg prednisone, 5 mg prednisolone, 4 mg methylprednisolone, 4 mg triamcinolone, 0.75 mg betamethasone and 0.75 mg dexamethasone.23 Cumulative dose was calculated for OCS use during the 1-year period before the index date.
Covariates
We considered covariates for TB risk adjustment as follows: inhaled respiratory medications other than ICSs, OCS use, presence of TB sequelae, immunosuppressant use, comorbidities, Charlson Comorbidity Index (CCI) and number of healthcare usages. Inhaled respiratory medications other than ICS included LABAs, LAMAs, SABAs and SAMAs, which were used within 1 year prior to the index date. If a combination package of two different inhalers was used, they were counted separately. The presence of comorbidities, CCI score and number of healthcare usages were counted during the period between the initiation date of inhaler and the index date.
Statistical analysis
Baseline characteristics at initiation date (including age, sex, comorbidities, number of healthcare usages and inhaled respiratory medication use) for cases and control patients were summarised using descriptive statistics such as proportion, median and IQR. Continuous variables such as CCI score and number of healthcare usages were categorised into the appropriate categorical variables based on their distributions, because their distributions are skewed to the right.
The association between the use of inhaled respiratory medication and TB was investigated by conditional logistic regression, adjusting for inhaled respiratory medications other than ICSs, OCS use, presence of TB sequelae, immunosuppressant use, comorbidities (malignancy, diabetes, chronic renal failure, silicosis, malabsorption, HIV/AIDS, transplantation), CCI (0–1, 2–3, >4), number of healthcare usages (number of hospitalisations (0, 1, ≥2) and number of outpatient visits (<15, 15–30, 31–50, >51)). Variables for adjustment were selected based on likelihood ratio test to explore the effects of each variable on TB risk and clinical judgments. Likelihood ratio tests were used to examine the goodness of fit of the model, and no significant lack of fit was found. Adjusted odd ratios (aORs) are presented together with 95% CIs and a p value. Unadjusted and adjusted ORs after adjusting for covariates were estimated from conditional logistic regression. To explore the dose-response relationship, we divided the distribution of the cumulative ICS dose into five groups (0, ≤15 000, 15 001–45 000, 45 001–75 000 and >75 000 μg). Tests for trends were performed using the medians of each group as continuous variables in a conditional logit model.24
Protopathic bias25 can occur when early symptoms of undetected pulmonary TB could affect the use of ICSs. To explore the impact of protopathic bias, we performed a sensitivity analysis ignoring ICS and OCS use during the period within 3 or 6 months prior to index date (the day of TB diagnosis).
To assess effect modification of inhaler medication use on TB in OCS users, we considered the interaction term between ICS use and OCS use in adjusted model. A p value of less than 0.05 was considered statistically significant and all statistical analyses were performed using SAS V.9.2 (SAS Institute, Cary, North Carolina, USA).
Results
We identified 1 341 229 individuals with prescriptions for inhaled respiratory medications with a duration of 30 days or longer between 1 January 2007 and 31 December 2010. Among them, 203 230 individuals who had had previous prescriptions for inhaled respiratory medications for 30 days or longer during the year before the current initiation of inhaled respiratory medication as well as 941 individuals with ICD-10 diagnoses of TB that had been present during the 1-year period before the index date were excluded. Additionally, 283 619 individuals who were aged <20 years or of unknown age were excluded. Finally, a cohort of 853 439 new users of inhaled respiratory medication was identified (figure 1).

Patient selection flowchart. ICD-10, International Statistical Classification of Diseases and Related Health Problems, 10th edition.
During the study period, 4146 individuals in this cohort were newly diagnosed as having TB.
Patients with TB and controls
For the 4139 individuals with TB, we identified 20 583 controls matched (figure 1). A total of 67% of patients with TB and controls were men. The median ages of the patients with TB and those of controls were 67 years. COPD and asthma were the most common diseases among them. Approximately 9.2% of patients with TB and 10% of controls had diagnoses of malignancy. In addition, 8.5% of patients with TB and 11.3% of controls had diabetes (table 1).
Demographic and clinical characteristics of patients with tuberculosis and controls
Impact of ICSs on the risk of TB
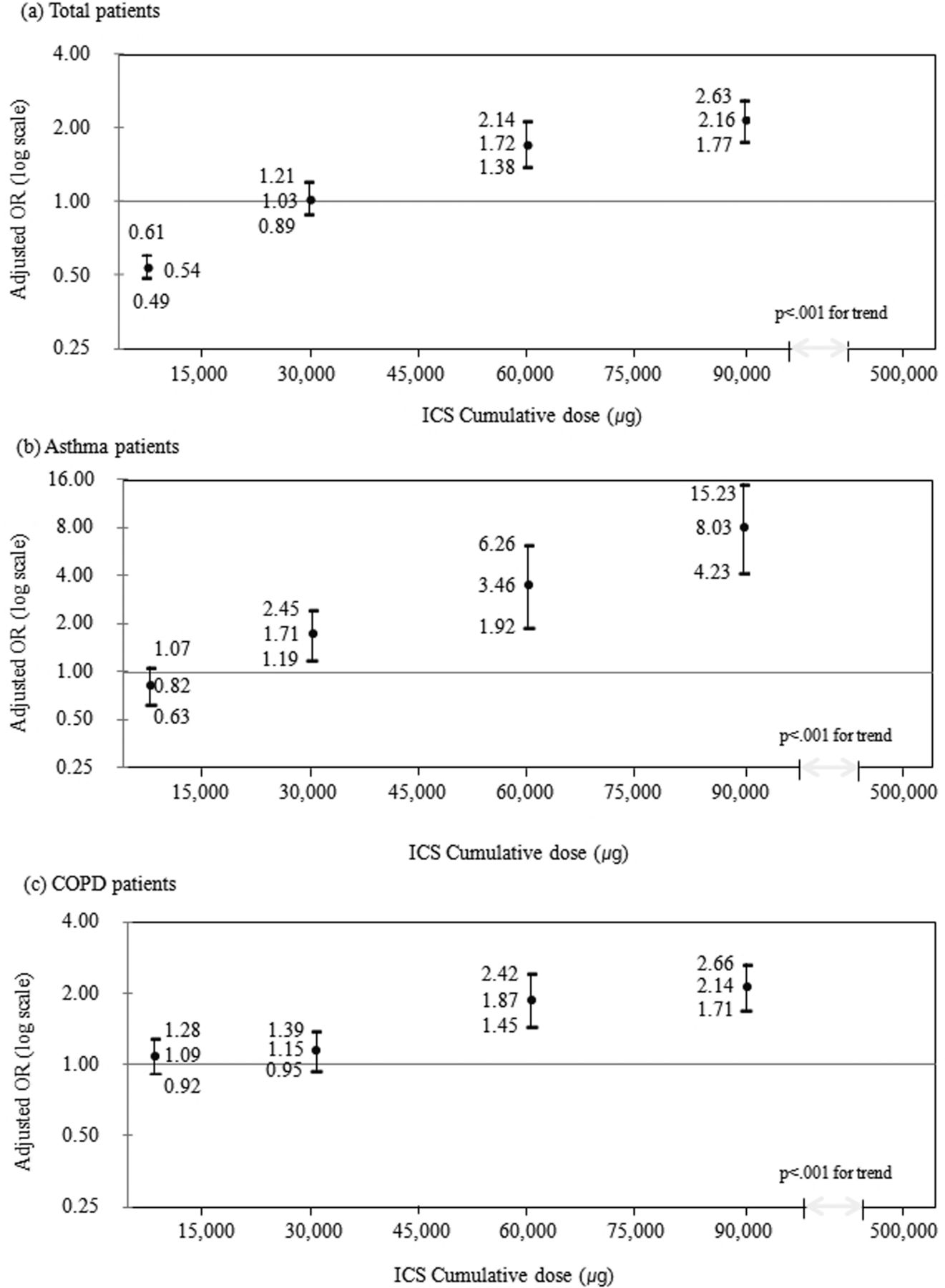
After adjusting for differences in the covariates, ICS use was associated with an increased rate of TB diagnosis (aOR 1.20; 95% CI 1.08 to 1.34). Additionally, the association between ICS use and an increased risk of TB was dose dependent (p for trend <0.001, figure 2). OCS use also increased the risk of TB development (aOR, 1.83; 95% CI 1.58 to 2.12). The association between ICS use and TB was maintained in 3-month and 6-month lag-time sensitivity analyses (table 2).
Risk of tuberculosis according to inhaler medication use

{kind=link}
{kind=link}
Dose-dependent relationship between cumulative doses of inhaled corticosteroid (ICS) and diagnosis of tuberculosis (TB). (A) All patients, (B) patients with asthma and (C) patients with chronic obstructive pulmonary disease (COPD).
Subgroup analysis according to oral corticosteroid use
OCS use was a statistically significant effect modifier of the association between ICS use and TB development (p for interaction=0.02). Among OCS users, ICS use did not increase the risk of TB development (aOR 1.35; 95% CI 0.86 to 2.12). However, among non-users of OCS, ICS use was associated with the diagnosis of TB (aOR 1.17; 95% CI 1.03 to 1.33). The association between ICS use and an increased risk of TB was dose dependent (p<0.001 for the trend) (table 3).
Subgroup analysis according to use of oral corticosteroid
Subgroup Analysis according to asthma or COPD
ICS use dose-dependently increased the risk of TB development among patients with asthma (aOR 2.30; 95% CI 1.55 to 3.41) as well as patients with COPD (aOR 1.84; 95% CI 1.56 to 2.17). In particular, patients with asthma with cumulative dose of ICS higher than 75 000 μg showed the highest risk of TB development (aOR 8.03; 95% CI 4.23 to 15.23) (table 4 and figure 2). OCS use also increased the risk of TB development in both groups of patients (table 4).
Subgroup analysis according to asthma or COPD
Discussion
In this nested case-control study based on the nationwide database of South Korea, we showed that ICS use increased the risk of TB development, in a nation in which the incidence of TB was 97 cases per 100 000 population in 2010. A higher risk of TB among ICS users was observed in patients with COPD and in patients with asthma as well.
Corticosteroids cause immune system suppression through peripheral blood monocytopoenia and inhibition of monocyte functions, including chemotaxis, bactericidal activity, and production of interleukin (IL)-1 and TNFα.26 Additionally, corticosteroids inhibit T cell activation, leading to reduced proliferative responses and cytokine production, and they also induce redistribution of T lymphocytes out of the circulation, leading to peripheral lymphocytopoenia.27 Based on their immunosuppression, use of corticosteroids could increase development of TB.4 An increased risk of TB was observed at doses as low as the daily ingestion of 7.5 mg prednisone.28 Given that prednisolone and inhaled fluticasone propionate are approximately equivalent on a 10:1 mg basis in terms of adrenal suppression,29 the possibility of TB reactivation among ICS users has been suggested.10–12 ,30 Subsequently, an increased risk of TB development among ICS users was reported in an analysis of a cohort of 427 648 individuals with airway diseases based in Canada.13 However, in that study, because the majority of ICS users were unlikely to have had LTBI, the impact of ICS use on the reactivation of TB among patients with LTBI may have been underestimated.14 In South Korea, the prevalence of LTBI, defined by positive interferon γ release assay among people older than 60 years without old, healed TB on chest radiography, was 67% in 2010.31 Analysis of a larger cohort consisting of 853 439 new users of inhaled respiratory medication in South Korea, an intermediate-TB-burden country, confirmed that ICS use could increase the risk of development of TB.
In particular, patients who used more than 45 000 μg of ICS had an OR for TB development higher than 2. Given that the OR of TB development among users of TNFα inhibitors is 2.0,4 testing and treatment for latent TB should be considered in patients who need long-term use of a high-dose ICS inhaler.
In our study, an association between ICS use and higher risk of TB development was observed in patients with COPD and in patients with asthma as well. In patients with asthma, the association was observed from lower cumulative dose of ICS than in patients with COPD (15 001–45 000 μg among patients with asthma vs 45 001–75 000 μg among patients with COPD). In particular, in patients with asthma with a cumulative dose of ICS higher than 75 000 μg, the odds for TB development were as high as 8.03. The observed higher susceptibility to TB development from ICS use in patients with asthma is not easily explained. Before jumping to any conclusions, we should wait until other studies confirm this observation.
Subgroup analysis based on OCS use revealed that ICS use in addition to OCS did not increase TB development. In fact, the Canadian study supports this observation.13 OCS use is a well-known risk factor for TB development4 ,28 and our study showed that OCS use of more than a cumulative dose of 1680 mg of hydrocortisone equivalents was associated with an increased risk of TB development among inhaler users in every analysis. Given that OCS use in itself is a strong risk factor for TB development, the results of this study and the Canadian study suggests that the additional contribution in OCS users in increasing the risk of TB could be negligible.
To correctly appreciate our results, the strengths and limitations of the study must be acknowledged. One of the main strengths of the current study was that it was based on a nationwide claims database, which minimised the likelihood of selection bias. Additionally, we avoided protopathic bias, which occurs when early symptoms of undetected TB affect the use of ICS, through 3-month and 6-month lag-time sensitivity analyses. However, our study also had limitations. First, heterogeneous patients with various respiratory diseases were enrolled, which might have obscured the actual effects of the drugs on the risk of TB. Nevertheless, consistent results from various subgroup analyses indicate that this limitation may be inconsequential. Second, the smoking status of inhaled respiratory medications users was not available. Selecting controls from users of other inhaled respiratory medications and matching and adjusting for important variables such as age, sex, asthma or COPD, CCI scores and healthcare usage could minimise the confounding effects of smoking on the results of this study.
In conclusion, the use of ICS increases the risk of TB in an intermediate-TB-burden country. Clinicians should be aware of the possibility of TB development among patients who are high-dose ICS users.
References
Footnotes
-
Contributors Literature research: J-JY, C-HL, MKH, EJJ. Figures: KK, NRL. Study design: J-JY, C-HL, MKH. Data collection: MKH, EJJ, KK. Data analysis: EJJ, KK. Data interpretation: J-JY, C-HL, MKH, EJJ, KK, NRL. Writing: J-JY, C-HL, MKH, EJJ, KK. Administrative, technical, or material support: MKH, NRL, KK, EJJ.
-
Funding This study was completed as part of the health technology assessment report (project no. NC2011-004) funded by National Evidence-based Healthcare Collaborating Agency (NECA) in South Korea.
-
Competing interests None.
-
Ethics approval The ethics review committee of the National Evidence-based Healthcare Collaborating Agency, Seoul, Republic of Korea.
-
Provenance and peer review Not commissioned; externally peer reviewed.