Article Text

Abstract
Background: The UK National Health Service is failing to meet the need for diagnosis and treatment of allergic disorders, which are common and increasing in prevalence. The House of Commons select committee report on allergy services highlighted the inequalities and urgent need for investment.
Aim: To survey the allergy workload provided by clinical immunologists to inform service planning and resource allocation.
Methods: The allergy services performed by clinical immunologists during a 12 month period from 1 April 2003 to 31 March 2004 were surveyed by means of a questionnaire via supraregional audit groups.
Results: The immunology centres surveyed serve 32 million people and offer almost the complete repertoire of a specialised allergy service. There were large variations in clinic capacity, new referrals, appointment duration, and service configuration. Services were largely consultant delivered, but availability of joint clinics with paediatricians and anaesthetists was locally variable. Novel service delivery models utilising nurses and clinical assistants have been developed and merit further investigation.
Conclusion: Consultant immunologists and trainees currently make a major contribution to the development and provision of specialised allergy services. Consultant immunologists will probably remain key providers of tertiary level allergy care in the UK in the long term (in line with other countries) and will be pivotal in supporting and developing the provision of equitable national access to specialist allergy services in a timely manner. Rapid progress in developing the new specialty of allergy and securing better access to services for patients in the short term will be best served by strengthening the collaborative relationship between allergists and clinical immunologists.
- immunology
- clinical allergy services
- audit
- workload
Statistics from Altmetric.com
Clinical immunologists in the UK undertake a range of clinical and laboratory duties, but their core activities are in the clinical management of patients with primary immunodeficiency and allergy.1 There is a misconception, recently repeated within the report of the health select committee, that immunology is principally a laboratory based discipline, and that no specialised allergy service exists north of Manchester or west of Bournemouth. Clinical immunologists provide clinical services for patients with various other immunological disorders (infections, vasculitis, human immunodeficiency virus infection, transplantation, haematological malignancy) and, like allergists, manage both adults and children with a variety of disorders affecting many organ systems.2,3
“Allergy currently affects one third of the general population and its prevalence is increasing”
The clinical immunology curriculum and syllabus includes a thorough grounding in the science and clinical management of all aspects of immunology, specifically including the immunology of allergy. Most immunologists hold joint membership of the Royal College of Physicians and the Royal College of Pathologists by examination. In addition, most immunologists working today completed pre-Calman training in immunology and allergy, which included an even larger allergy component, and which pre-dates the introduction of a separate specialty of dedicated specialist allergists.
Clinical immunologists are the largest single specialty providing tertiary level allergy services throughout the UK at present, but there is a lack of detailed data regarding the level of service provided.
Allergy currently affects one third of the general population and its prevalence is increasing.4–6 National Health Services are experiencing the pressure of increasing workload and insufficient resources. Recent surveys of allergy workload within the UK have not specifically identified the contribution of immunology to specialist service provision because of a lack of data.4,6 We have surveyed this workload to inform service planning and resource allocation, and based our assessment on the standards set out in the Department of Health’s definition of a specialist allergy service (specialised services definition number 17).7
METHODS
Data were collected (via Excel spreadsheets) for the period 1 April 2003 to 31 March 2004 from regional immunology centres in the three UK supraregional immunology audit groups: the North of England Clinical Immunology Audit Group, the South and West of England and Wales Clinical Immunology Audit Group, and the London and the South East Group Clinical Immunology Audit Group. A copy was sent to the British Society for Allergy and Clinical Immunology for distribution to allergy centres.
Centres participating in the South and West of England and Wales Clinical Immunology Audit Group are Cardiff, Bristol, Plymouth, Oxford, Birmingham (City, University, and Heartlands Hospitals), Cambridge, and Southampton. Centres participating in the North of England Clinical Immunology Audit Group are Belfast, Newcastle, Middlesbrough, Leeds, Sheffield, Path Links, Hull, Manchester Central, Salford, Liverpool, Preston, North Birmingham, Nottingham, and Leicester.
The questionnaire related to:
-
Service repertoire provided in clinical allergy.
-
Staffing.
-
Workload and waiting times.
-
Joint clinics with other specialists.
-
Specialist activities including: desensitisation, food challenges, nurse led Epipen clinics.
-
Laboratory activity for allergen specific IgE assays.
The questions concerning services provided in clinical allergy were based on specialised services definition number 17 for allergy.7 Questions on laboratory activity related to the number of allergy tests performed in the laboratories and the amount of time devoted each week to laboratory allergy.
Where exact workload figures were not yet available for the survey period, we requested estimated figures based on the previous year’s data. Overall, 65% of centres were able to provide in year data; 35% estimated activity based on the previous year’s figures.
RESULTS
Completed responses were received from 17 centres where the allergy service is led by clinical immunologists (Aberdeen, Belfast, Bristol, Birmingham City and Birmingham Heartlands Hospitals, Cardiff, Guildford, Hull, Leeds, Manchester Central, Newcastle, Oxford, Path Links, Plymouth, Preston, St Helier, and Sheffield) and one centre where the service is led by allergists (Southampton). The responses from Southampton are shown for information only but are not included in the analysis. The 17 regional services provided by consultant clinical immunologists that responded to the survey serve a total UK population of 32 million.
Services provided in clinical allergy within the specialised services definitions number 17
Table 1 summarises the allergy services provided by consultant immunologists in the 17 regional centres. None of the centres offers an open access skin prick test service to general practitioner referrals. All perform skin prick tests as part of the routine assessment of patients referred for allergy. All 17 centres offered all specialised services with the following exceptions:
Specialised allergy services provided by clinical immunology centres
-
Cardiff, Oxford, and Preston did not offer challenge testing because of a lack of resources.
-
Aberdeen did not offer desensitisation immunotherapy.
-
Cardiff and Sheffield adult immunology centres do not coordinate services via community paediatricians for the management of children because comprehensive allergy services are provided by paediatricians in Cardiff and a paediatric immunologist in Sheffield.
-
Paediatric allergy services are run separately from clinical immunology services in Aberdeen, Newcastle, and Sheffield.
-
The Birmingham City Hospital, Cardiff, Hull, Manchester, and Preston centres do not have dedicated inpatient facilities easily available for active admission of patients. However, all had access to inpatient beds for emergency admissions.
Staffing and workload in clinical allergy
Table 2 summarises the relevant data on staffing and a summary of the allergy workload data. Figure 1 shows the allergy workload by diagnostic category. The case mix is similar throughout the UK; urticaria/angio-oedema, serious anaphylaxis, and food allergy/intolerance comprise 65% of referrals. Figure 2 shows the breakdown of service provision by each grade of staff. The services are predominantly consultant delivered. There is a large variation in the number of clinics in each centre. Notional appointment durations range from 15 to 45 minutes, but the average is 30 minutes or less in 13 of 17 centres, which is less than college guidelines of 40–45 minutes for each new patient.2 Follow up appointments range from 10 to 20 minutes. Services are difficult to compare: the “one stop” patient may spend longer than 30 minutes seeing other clinic staff for counselling, explanation of treatment plans, Epipen training, and skin prick testing in a notional 30 minute appointment. Similarly, patients seen by a nurse practitioner, trainee doctor, or general practitioner with a special interest will be discussed with the consultant and so will have a length of stay in excess of the notional time. There is great variation in follow up policies, with some clinics delivering a “one stop” visit wherever appropriate. Just as it is impossible to compare the notional clinic appointment times on this basis, it is not possible to make inferences about the quality of the experience for the patient or the efficiency of the process. Clearly, there are a variety of service models in existence for evaluation to inform the governmental strategy to deliver improved care for patients with allergy. In particular, the use of nurse practitioner staff and general practitioners with a special interest merits exploration as a method of enhanced service delivery.
The staffing structure and workload of allergy services based in regional immunology units

Analysis of allergy caseload by diagnosis in allergy services based on regional immunology units. The figure shows the breakdown of the total allergy workload by diagnostic category in 12 centres. There was a similar case mix across the centres surveyed. Five centres were unable to provide a detailed breakdown and their data have been excluded.
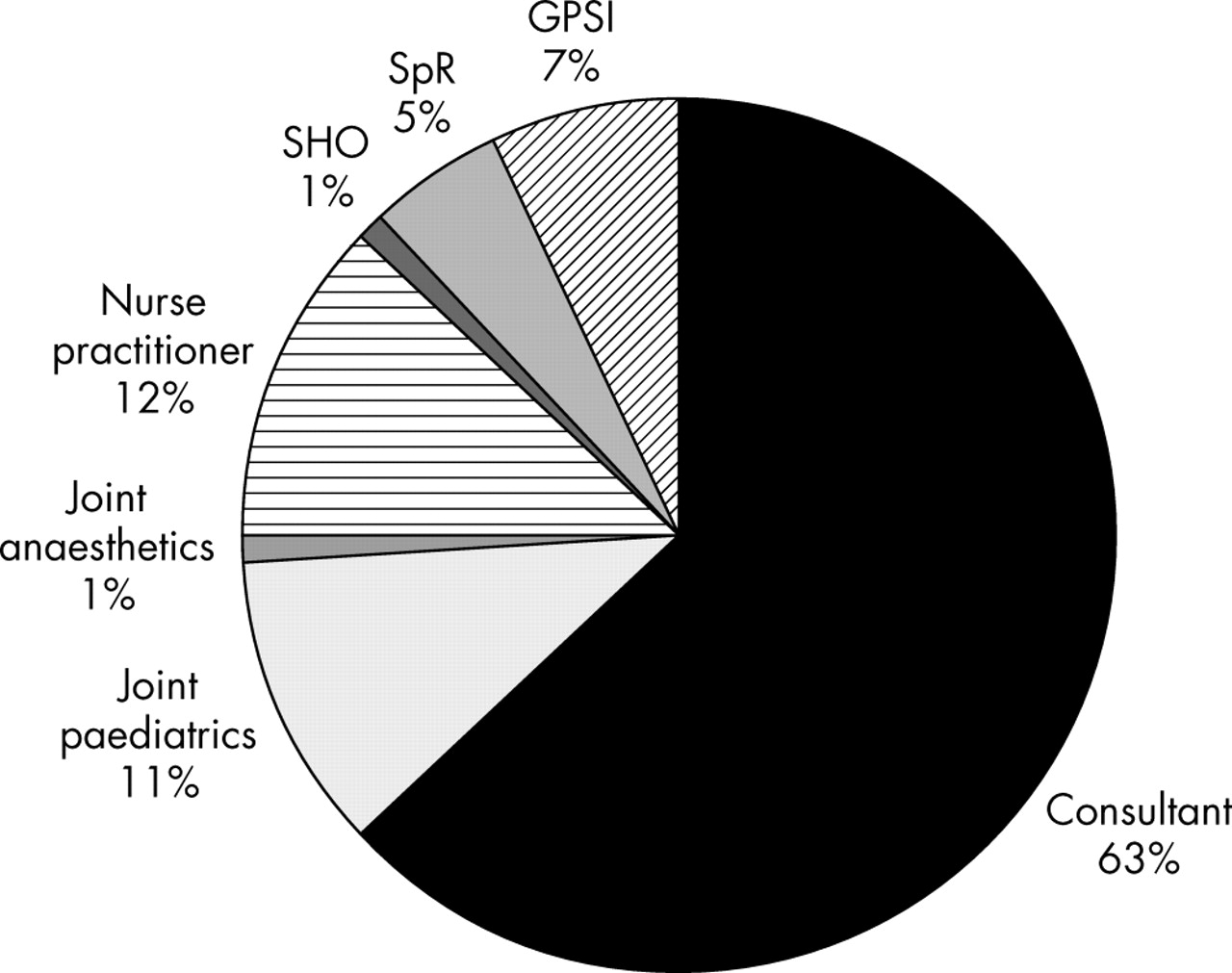
Percentage of new patients seen by different staff (total for all centres). The figure shows the distribution of new allergy consultations by staff grade in 15 centres (data not available from two centres). Allergy provision by immunologists in the UK is predominantly a consultant driven service. Twenty five per cent of consultations were with other staff who were directly supervised by consultants. GPSI, general practitioner with a special interest; SHO, senior house officer; SpR, specialist registrar.
Waiting times in England varied between two and 20 weeks for a routine new appointment, and from zero to four weeks for urgent appointments. Some centres experienced severe workload pressure, with waiting times of 260 and 26 weeks for Belfast, 143 and 60 weeks for Cardiff, and > 100 and four weeks for Aberdeen for a routine new appointment and urgent appointment, respectively.
Staffing levels and mix vary greatly between centres, relating to differences in workload and the variable amount of consultant time spent on allergy activity (from 0.5 to 15 programmed activities (four hour blocks of time)/week). Services are predominantly consultant delivered. Patients seen by nurse practitioners or junior medical staff are discussed in detail with the consultant. One centre makes extensive and effective use of a general practitioner with a special interest. There is a lack of dedicated support from dieticians, and this is a matter of concern, because it is a key service component for the effective delivery of specialised allergy care for food allergies.7 The variation in workload in allergy, non-allergy clinical work, teaching, research, and other duties is consistent with the great variation in job plans of consultants in immunology across the UK.
Joint clinics with other specialists
Joint clinics for patients with suspected anaesthetic allergy were carried out with anaesthetists in six of the 17 centres, and comprised 2.8% of the caseload in these six centres. Children were seen in joint clinics with paediatricians in eight of the 17 responding centres, and 15.6% of the patients at these eight centres were seen in such clinics.
Arrangements for joint clinics with other specialists varied greatly, apparently reflecting the individual interests of different consultants, local service requirements, and the workload pressures on single handed practitioners. This method of enhanced service delivery requires evaluation for cost effectiveness and efficacy.
Desensitisation, food challenges, nurse led activity, etc.
Table 3 shows the desensitisation, Epipen clinic, nurse led clinic, and allergen challenge activity. Desensitisation was carried out in all but one centre (Aberdeen). Fifteen of the 17 performed food challenges, mostly as outpatient activity. In all centres, Epipen training was provided but such activity occurred, often unrecorded, during initial and follow up clinic appointments rather than in dedicated Epipen clinics.
Table of desensitisations, food challenges, and nurse led activity
Laboratory activity in allergy
Table 4 summarises the data relating to allergy laboratory tests, turnaround times, and clinical correspondence.
Laboratory activity relating to allergy and communications practices
The number of allergen specific IgE and total serum IgE assays performed varies greatly. Sheffield and Cardiff test large numbers by virtue of a supraregional workload as “protein reference units”. In general, the turnaround time for laboratory tests and dispatch of letters relating to clinical consultations with patients are excellent. Clinic letters are routinely copied to the patient in six of the 17 centres; and dictated in the presence of the patient in an additional centre, in line with national Department of Health aspirations for improved communications.
DISCUSSION
This is the first large scale survey of clinical allergy activity provided by clinical immunologists in the UK, and provides important new data for the planning of a national network of allergy services. It reveals that clinical immunologists are currently the major providers of regional specialised clinical allergy services covering most of the UK and meeting the specialist service definitions for the 32 million people surveyed. Clinical immunologists have provided leadership in developing new service models for allergy provision and have led in the establishment and development of services throughout the UK. Other organ based specialists such as respiratory physicians, ear nose and throat surgeons, and dermatologists also see some patients with organ based allergic disease within the same population, but there is little published data and few provide the full repertoire of specialised services.5 Immunology centres are the only providers of generalised tertiary level specialist allergy services for most of the UK. Fourteen of the 17 participating centres offered all the services listed in the specialised services for allergy definition number 17.7
Consultants and trainees in clinical immunology currently make a major contribution to the development and provision of specialised allergy services at secondary and tertiary level, and have provided leadership and championed the provision of regional specialised allergy services. Even if a substantial number of new consultants in the separate speciality of allergy are trained in the next 10 years, consultant immunologists will probably remain key providers of specialist clinical care in the long term (in line with the situation in other countries), and will be pivotal in supporting and developing the provision of equitable access to specialist allergy services on a national basis in a timely manner. The potential benefits and roles of general practitioners with a special interest and of nurse practitioners require further assessment, but there are already several effective models of service delivery utilising these resources within the immunology community. Rapid progress in developing the specialty of allergy and securing better access to services for patients in the short term will depend on strengthening the collaborative relationship between allergists and clinical immunologists to maximise access to high quality specialised allergy services throughout the UK, to improve education and support for primary care, and to end the current geographical inequality of access to tertiary level services. Collaboration might involve facilitating or hosting the training and development of allergy specialist registrars alongside immunology trainees, the development of colocalised services led by allergists and immunologists sharing the same facilities, and the development of service models for maximum cost effectiveness.
“Clinical immunologists have provided leadership in developing new service models for allergy provision and have led in the establishment and development of services throughout the UK”
Allergists are currently available in only a few centres in the UK, predominantly in the South East of England. In most regions of the UK, clinical immunologists provide the only hospital based specialist allergy service for patients with widespread, complex, severe, or multisystem allergies. Thus, throughout the UK, postgraduate training programmes in clinical immunology always have, and continue to, incorporate a substantial amount of allergy training. Allergy forms part of the curriculum and syllabus of clinical immunologists as set out by the joint committee on higher medical training; allergy is recognised as part of the services offered by clinical immunologists,3 and most immunologists maintain continuing professional development in allergy.
The National Health Service is struggling to cope with the explosion in allergic diseases over the past decade. As a specialty, the clinical immunology consultant community fully endorses the recommendations of the Royal College of pathologists’ publication Allergy, the unmet need and the aspirations of the few existing consultant allergists to establish an expert cadre of consultant allergists whose clinical focus is on allergic disease alone. Any plans to meet this great need are likely to be successful if built upon existing service provision for allergy and the current referral pathways for patients with allergy (fig 3). We believe that the greatest progress can be made most quickly by recognising and building on this foundation, while simultaneously expanding the specialty of allergy and strengthening the relation between it and related specialties, such as clinical immunology, to sustain targeted research, provide effective service provision, and identify and promote good clinical practice. The few full time allergy consultants and specialist registrars in training in the UK at present mean that sufficient consultant allergists are not likely to be available to service an adult expert allergist network for at least 20 years, even at the maximum training capacity, unless immunology centres with sufficient expertise are involved. The situation for paediatric allergy specialists is even worse. In view of this, it makes good sense to co-opt the existing nationwide infrastructure of clinical immunology services in any future service plans to improve the provision of national allergy services.

{kind=link}
{kind=link}
{kind=link}
Map of allergy services. In the National Health Service, services for patients with allergy tend to be provided by clinical specialists in the system involved (such as the chest for asthma). Increasingly, there is subspecialisation within these teams such that one specialist sees all patients with allergy. Over the past 20 years, clinical immunology has grown as a specialty and services are available in major medical centres across the UK. Specialists in clinical immunology are trained both to provide professional direction to diagnostic immunology services and manage patients with illness caused by abnormality of the immune response, including allergy. Most clinical immunology services provide allergy services, which tend to see patients in whom more than one system is involved (such as those with anaphylaxis). The number of patients seen by these services has grown rapidly in recent years. To date, the specialty of allergy alone has been provided in a few teaching hospitals only, usually in an academic setting. Some of these services are world leaders in research. All these clinical teams delivering allergy services set standards of best clinical practice, provide a resource for training, and offer tertiary referral of difficult cases. ENT, ear, nose, and throat.
Take home messages
-
Consultant immunologists and trainees currently make a major contribution to the development and provision of specialised allergy services
-
Consultant immunologists will probably remain key providers of tertiary level allergy care in the UK in the long term, and will be pivotal in supporting and developing the provision of equitable national access to specialist allergy services in a timely manner
-
Rapid progress in developing the new specialty of allergy and securing better access to services for patients in the short term will be best served by strengthening the collaborative relationship between allergists and clinical immunologists
Acknowledgments
We thank Professor D Warrell for permission to include data from the Oxford venom desensitisation clinic.
Footnotes
-
This study was undertaken on behalf of the South and West of England and Wales, and the North of England and Northern Ireland Clinical Immunology Audit Groups.