Article Text

Abstract
Objective This study explores the provision of spiritual care by healthcare professionals working at the end of life.
Design Qualitative–ethnographic inquiry.
Setting Phase 1: five Canadian sites; phase 2: a residential hospice in Alberta, Canada.
Participants Phase 1: six palliative care leaders; phase 2: 24 frontline palliative care clinicians.
Results Data were collected over a 12-month period with analysis of findings occurring concurrently. Using semistructured interviews and participant observation, 11 themes, organised under five overarching categories, emerged from the data. Five bedside skills were identified as essential to spiritual care: hearing, sight, speech, touch and presence. The integration of these bedside skills with the intrinsic qualities of healthcare professionals, including their values and spiritual beliefs, appeared to be essential to their application in spiritual care. Spiritual care primarily involved the tacit qualities of healthcare professionals and their effect on patient's spiritual well-being, rather than their explicit technical skill set or expert knowledge base.
Conclusion Participants identified spiritual care as both a specialised care domain and as a philosophy of care that informs and is embedded within physical and psychosocial care. Hearing, sight, speech, touch and presence were identified as the means by which healthcare professionals impacted patients' spiritual well-being regardless of clinician's awareness or intent. An empirical framework is presented providing clinicians with a pragmatic way of incorporating spiritual care into clinical practice.
Statistics from Altmetric.com
Introduction
Addressing the spiritual needs of patients is a core component of comprehensive cancer and palliative care.1,–,3 The National Comprehensive Cancer Network distress management and palliative care guidelines recommend routine screening and assessment of patients' spiritual issues.4 ,5 Spiritual care addresses issues associated with individual's beliefs, values, behaviour and experiences related to ultimate meaning.6,–,9 Most patients, especially those facing the end of life, want their spiritual needs addressed by their healthcare professionals.10,–,13 The spiritual domain has been reported to be of equal importance and, in some instances, more important than other health domains for patients facing a life-threatening illness.4,–,18 Failing to address patient's spiritual needs is associated with higher patient distress, higher health costs and adverse clinical outcomes.9,–,21 These emerging concerns, and prior recommendations of the National Consensus Project Guidelines and the National Quality Forum Preferred Practices and Conference proceedings, resulted in a national consensus project on improving the quality of spiritual care at the end of life to recommend routine screening for spiritual distress.22 While addressing patients' spiritual needs has been endorsed by professional bodies and healthcare organisations, there is surprisingly little clinical guidance on what constitutes spiritual care and how clinicians might best meet these important needs.1,–,5 ,23,–,26 This study investigates the core elements of spiritual care from the perspective of palliative care leaders and frontline professionals in order to provide clinical guidance on how to integrate spiritual care into routine bedside clinical care.
Methods
Participants
This study was a part of a larger ethnographic inquiry, exploring the spirituality of Canadian palliative care professionals. The recruitment characteristics of this multicentre qualitative study have been described in detail previously.6 Briefly, the first phase involved a purposive sample of six leaders (19.8 average years of service in palliative care) in palliative and hospice care at five centres across Canada. Each key leader consented to waive his or her anonymity, allowing their expert opinions to be acknowledged. This option was not available to frontline staff who participated in the second phase of the study, as individuals who wished to remain anonymous could be more easily identified through a process of elimination (table 1). In this second phase of the study, a convenience sample of 24 frontline palliative and hospice care professionals (7.2 average years of clinical service in palliative care) were recruited from a hospice in southern Alberta, Canada. This study was approved by the Conjoint Health Research Ethics Board of the University of Calgary, the Ottawa Hospital Research Ethics Board and the Fraser Health Research Ethics Board.
Participant demographic data
Method
An ethnographic approach was used in order to capture explicit and implicit meanings embedded within the culture of palliative care. Semistructured interviews and participant observation were used to gather data. A poststructuralist approach to ethnography was employed in this study.27 In contrast to classical ethnography which is rooted in realism, ethnography from a poststructural perspective understands truth as contextual, dynamic and embedded within the subjectivities of language.28 ,29 Poststructural ethnography acknowledges the researcher's role in the ethnographic report and controls this bias through the presentation of verbatim data which are constantly verified through an ongoing process of member checking. Interviews, ranging in duration from 1 to 2 h, were designed to provide a deeper understanding of data gained through observation. An interview guide was constructed, and the researcher used an open method of interviewing whereby the participants shared narratives pertaining to their perspectives on spirituality and providing spiritual care (Box 1). During the first phase, each leader was interviewed and observed in their clinical work for about a week. Interviews were audio recorded and transcribed. Field notes, containing informal discussions and participant observation, were captured in two ways: through the researcher audio recording his or her observations and through written field notes in the researcher's field journal. The second phase required the researcher to be immersed in the workings of a local hospice for 4 months where interviews and participant observation were also conducted.
Semistructured interview guiding questions
Interview guiding questions
What does a typical day at work look like for you?
What drew you to palliative care?
Do you have a sense of fulfilment working in palliative care?
What is spirituality?
Have you had what you would consider a ‘spiritual experience’ in your work or life?
Describe, if any, how your own spirituality connects with patients?
Have your patients influenced your own spirituality; if so, how?
Data analyses
In ethnographic research, data collection and analysis occur concurrently through a ‘back and forth’ process, consisting of an interplay between the emic (interview data from the perspective of an insider) and etic (participant observation data from the perspective of an outsider) perspectives.30 Poststructural ethnographers often coalesce emic and etic data rather than treating them as two distinct data sets.27 ,31 In this study, this iterative process involved the researcher continually validating participant observation data with participants themselves in order to produce ‘a ‘third dimension’ that rounds out the ethnographic picture’ (32, p.63). Comparing and validating interviews, informal discussions and participant observation allowed for member checking to occur in an ongoing reflexive manner, enhancing the credibility and validity of the data, while also informing subsequent data collection in the process. At the end of each phase of the study, two formal levels of analysis occurred.33 First, written field notes, transcribed audio-recorded field notes and transcribed interviews were read independently by the researcher (SS) and the auditor (SR) line-by-line with initial codes, words or phrases that captured the meaning of a section of text being recorded in the margins. Transcripts were then read a second time, developing a coding taxonomy, which developed into themes and categories that were continually refined and expanded as data were collected. The researcher and auditor met on a monthly basis to share individual analysis and themes, serving as the second level of analysis. A consensus method of coding agreement continued until all themes and categories were saturated, with a final level of member checking being employed when further clarity of the raw data was needed.
Results
Eleven themes, organised under five overarching categories, emerged from the interviews and participant observation data. The five categories described bedside skills essential to spiritual care: hearing, sight, speech, touch and presence (table 2). The integration of these skills with the intrinsic qualities of healthcare professionals, including their values and spiritual beliefs, appeared to be essential to their application in spiritual care.
The categories, themes and subthemes derived from the study data
Hearing: listening intuitively
Participants identified listening as an essential skill in effective spiritual care. Intuitive listening was described as an enhanced form of hearing, focusing on the subtext of a patient's life story as it related to his or her illness. Intuitive listening paid particular attention to the tone of the conversation, the silence between sentences and the implicit messages, allowing participants to elicit a deeper understanding of their patient's needs (box 2).
Categories and themes: hearing: listening intuitively
Category – hearing: listening intuitively
I'm going to go in and just listen. That already is a gift that I have given that person. (David Kuhl)
So much of it is intuitive, I’ve learned to trust that's how God's spirit talks to me, is through my intuition. There's that inner knowing…It's about knowing that God is there in the midst of that [conversation]. (Chaplain Ellen)
Theme: instrumental listening
I very much feel like a vessel, and just to keep myself open to being that vessel. That is really important… being a vessel gives the power to the source that it needs to be, and that's what I continue to hold before me. (Chaplain Ellen)
The relationship I have was definitely not nothing, it was definitely something that was valuable and brought some comfort but that also something more was needed many times. (Michael Kearney)
I'm going to go in and just listen. That already is a gift that I have given that person. (David Kuhl)
Not to do with me, it's not about ego… But one day the message was, ‘I’m sending you the people you need to see. Don't think there is anything special about you'…It's about being an instrument. I am but a channel, I am but an instrument. (Mary Vachon)
Theme: listening with humility
When I’m with a patient, the part of me that wants to be present is what I give without expecting gratitude. (David Kuhl)
… I never want my name on a [thank you] card… I do everything to serve. Everything I do here I feel is service to others. (Nurse Luella)
Instrumental listening
The capacity to listen intuitively also involved an emptying of self in order to function as a conduit of a Higher Power, Life Force or God. Participants in describing this skill often used the image of an instrument or vessel. While this connection often tapped into their unique gifts as individuals, the source of healing was understood as ultimately transcending the self. The prayer of St Francis was a powerful exemplar of this notion, with its supplication to be an instrument of peace, being referred to by a number of participants and displayed in two participants' offices.
Listening with humility
Intuitive listening required and cultivated humility on the part of participants, as they located the agency of spiritual care outside of themselves. Participants desired to be a conduit, but not the source of healing, reflecting a belief that this aspect of spiritual care could only be maintained in a position of proxy.
Sight: seeing soulfully
The notion of seeing soulfully differed from mere visual perception in intent and focus, as it involved participants looking beyond the surface to the person's essence and sacredness. Seeing soulfully also involved paying attention to the aesthetics within a patient's room – the pictures adorning the walls or greeting cards on their night table – objects providing further insights into their patients' inner world (box 3).
Categories and themes: sight: seeing soulfully
Category – sight: seeing soulfully
I try and read the person. I remember a patient who, from the treatments, she had not a square centimeter of skin left on her body. She was totally, totally disfigured. And she was one of the most beautiful people…. I could look right into her and also feel that I was totally comfortable with that disfigured body. (Jeremy Wex)
It (closing her eyes in therapy) is a part of my centring that I’m just being grounded, being centred now it was obviously beyond looking and seeing what's going on with that person…so I enter the space. (Mary Vachon)
We need to look at people, look at the person behind the face of disease and illness. (John Seely)
Theme: seeing the whole person: reflecting the person at the centre of care
I feel really strongly about this, the fact of having respect for one another, no matter what walk of life they come from and what's happening in their life. (Assistant Ashley)
At this place we are about loving people where they are at. (Nurse Louise)
That's something the person has to find within them self … what became more interesting to me was how to enable the person to tap into their own resources, however one understands that. (Michael Kearney)
What I’m doing is I’m taking the lead from the person I’m working with and reflecting their spirituality back. That's the best I can do. (Jeremy Wex)
You know if we don't understand the people, we don't know where they're coming from. (Volunteer Mary)
One of the characteristics of the people we care for is that their superficialities have been swept away. (Balfour Mount)
Theme: seeing the unseen: the divine within
My goal was to be in contact with God within him (patient). (MD Mark)
There is something else you can connect to… There's a feeling, that gentle feeling to a person at that particular moment, it just happens. (Assistant Ashley)
What matters is a sense of connection in the core of your being with something bigger than ourselves. (David Kuhl)
I think that really that there was something else possibly another, that was caring for (them). (Assistant Ashley)
Seeing the whole person: reflecting the person at the centre of care
Seeing the whole person allowed participants to better deliver care from a patient centred perspective. Field observation served as a valuable source of data in this regard, as members of the interdisciplinary palliative care team sought to understand and reflect back to the patient threads of meaning interwoven throughout the life and their own internal healing resources during routine care delivery. In applying this holistic lens to their clinical practice, participants emphasised unconditional acceptance of the patient, regardless of patients' awareness of their issues or their capacity to change.
Seeing the unseen: the divine within
As described by participants, ‘seeing the unseen’ was an attempt to discern and align with the divine within the patient, or as some participants described, the ‘divine spark’. In contrast to the category of hearing, which focused on transcendent aspects of spirituality, sight focused on immanent features of spirituality, embedded within the patient and the clinical encounter. Participants felt that their belief in a sacred element within the patient enhanced their respect, compassion and perceived dignity toward them.
Speech: taming the tongue
Reliance on verbal communication was often reported to inhibit effective spiritual care. When words were necessary in spiritual care, participants stressed the importance of being brief and choosing them wisely. Participants preferred instead to engage spiritual issues in a more experiential and subtle manner, assessing a dying person's sense of peace for example, first through non-verbal cues and intuition, rather than direct verbal engagement (box 4).
Categories and themes: speech: taming the tongue
Category – speech: taming the tongue
I began to realize that we can reach people through our attitude and nature and that spiritual development enables us to extend spiritual support without words.… I also started to integrate spirituality or spiritual awareness into my work with people suffering from cancer, not by preaching but through the virtues of love and respect. (Mary Vachon)
I say as little as possible. I try and get away with saying nothing. (Jeremy Wex)
We communed in silence. (MD Mark)
That is an expression of our spirituality because we are connecting on the deepest level. We may not use words, we may not use particular words, there's that human connecting. (Chaplain Ellen)
I believe it doesn't always have to be words. I mean yes, we need those, but there's just that sense that comes from within. (Assistant Ashley)
Theme: communicating in the language of the patient
I have a very flexible approach… my role will change with people. (Mary Vachon)
Using language that offers an opportunity for them to express what's really going on for them is important. (Nurse Luella)
Yes we bring our skills and yes we bring our training and our experience, but we also bring an open and ready spirit to meet people where they are. (Chaplain Ellen)
Theme: the danger of words
I have this conviction that words get in the way sometimes. (Jeremy Wex)
The god that can be defined is not god. (David Kuhl)
I remember saying, ‘You’re going to be fine, don't worry, they're looking after you well'… he died about five days later. (John Seely)
Communicating in the language of the patient
Communicating spiritual care in a language most meaningful to the patient involved a desire to understand each patient's spiritual background and to build from that perspective, rather than requiring patients to ascribe to the spirituality of participants. While participants brought their own spiritual beliefs to their relationships with the dying, they sought to discover how their own beliefs, experiences and values might be understood from the patient's vantage point, focusing on broad commonalities rather than differences.
The danger of words
A number of participants felt that verbal communication had equal potential to harm in the provision of spiritual care, especially when comprised of superficial clichés and hollow scripts of comfort. Participants indicated that their words had the potential to stifle the flow of patient driven and therapeutic conversations.
Touch: physical means of spiritual care
Clinicians recognised touch as an essential bedside skill in the provision of spiritual care. This included empathetic touch: holding a patient's hand or a gentle hand of reassurance on a patient's shoulder, for example. Physical care often established a natural foundation of intimacy and trust for conversations that were more spiritual in nature to transpire (box 5).
Categories and themes: touch: physical means of spiritual care
Category – touch: physical means of spiritual care
So (through the provision of physical care) your sense of safety with this doctor is increasing, so that if there is something you wanted to explore, you're going to say to him, ‘you know, there’s something I’ve been wanting to talk to somebody about for a long, long time and I think I can trust you now'. (David Kuhl)
The best part of my day after morning med rounds is getting to actually participate in hands-on care… Little things mean everything… I love doing even the nastiest of jobs – anything that has to do with touching and cleaning and making beautiful. (Nurse Luella)
Theme: the therapeutic effect of touch
The nurses touch patients on this unit, they communicate respect. (Jeremy Wex)
I think a lot of that came up because we had to do the hands-on care. I’d often establish really good relationships with the clients, with the family by doing that. (Volunteer Mary)
Sometimes it is in a prayer, but sometimes it is in a held hand. (Nurse Lily)
Theme: embodied spiritual care
People have that sense that you'll go out of your way to do something, and I don't think of it as going out of my way… That's service, anything that I can do to make them comfortable. I’ll run down three blocks and get them an ice cream cone if that was going to make them feel comfortable. (Nurse Luella)
I remember this one resident who was deplored that she was incontinent and needing me to clean her up. I said to her, ‘I’m the pooping queen!' and from that point on we were on a completely different level. (Assistant Dianne)
The therapeutic effect of touch
Although spiritual care was primarily associated with non-tactile bedside skills, the manner in which physical care was provided was felt to have an effect that extended well beyond the patient's body, modifying the patient's spiritual well-being. Participant observation served as a valuable source of data in this respect as the researcher observed practices that were considered routine to participants (eg, a physician holding a patient's hand when breaking bad news, a nurse's tenderness in wound care), yet were often informed by participants' beliefs and values. The researcher learnt that a ‘spa day’, for example, occurred in the newly renovated hospice bathing room when patients were in need of a little extra tender-loving-care.
Embodied spiritual care
Investing physical tasks with virtues of acceptance, love, respect, dignity and compassion extended their therapeutic effect to the spiritual domain. In this study, spiritual care expressed through physical acts was evident in: a nurse removing a mirror from a patient's room, because it served as a constant reminder of the toll of cachexia; a nursing assistant massaging an achy back; and a physician laying a gentle hand of comfort on the shoulder of a dying man. Although embodied spiritual care was frequently associated with disease management, it also involved physical acts intended to enhance a patient's dignity and sense of self (personhood).
Presence: the essence of spiritual care
The fifth bedside skill, presence, was the foundation upon which the other four categories were grounded. Presence was seen as the outward radiance of an individual's essence or soul. Presence was not based on technical competence, spiritual awareness or self-assessed spirituality, but the expression of clinicians' character, beliefs, behaviour and giftedness within their clinical practice. Participants believed that presence was an innate aspect of humanity, experienced relationally in terms of ‘being with’ rather than ‘doing for’. The effect of presence was not restricted to individuals who ascribed to its existence or to a personal spirituality; rather, participants believed a clinician's presence affected patients whether clinicians were aware of it or not. In short, presence was what clinicians brought and left in a patient's room (box 6).
Categories and themes: presence: the essence of spiritual care
Category – presence: the essence of spiritual care
Your presence is the best gift you can give anybody. (David Kuhl)
Not necessarily somebody who was saying anything or teaching anything with their words, just the quality of presence. (Michael Kearney)
To be able to provide support and care to people as they conclude their earthly life and prepare for whatever they believe is ahead and provide a gentle presence in the midst of that helps contribute to making this a meaningful time. (Chaplain Ellen)
Theme: being vulnerable
My guess is that being vulnerable and being open is an important part of being in touch with one's spirituality, and that is not necessarily a comfortable place to be. (John Seely)
You are basically handing over that power, that need for control, requiring humility, open spirit, open heart, all of those things. (Chaplain Ellen)
Subtheme: professional vulnerability: relinquishing the expert model
It is particularly uncomfortable as a physician when you are not able to provide the answers. I am constantly fighting that myself. (John Seely)
There is a risk of giving answers to the question, and what I do know about my job is that there are no answers. (Jeremy Wex)
It would be hard to work in palliative care and not be aware of one's vulnerability. (Balfour Mount)
Subtheme: personal vulnerability: the precursor of presence
The healing part is what I bring as a person… Any question you ask another person, you have to first ask yourself. (David Kuhl)
It requires a part of our personhood whether it's reflecting on our own spirituality, or in talking to a patient, sharing parts of ourselves or laying down our role as professionals… It speaks of a requirement of ourselves as being, as sharing ourselves, as risking ourselves. (Mary Vachon)
The other thing I link to these reflections is some kind of practice towards self-knowledge, a reflective practice towards self-knowledge. (Balfour Mount)
Subtheme: the effect of vulnerability in spiritual care
If one is open to that kind of experience you can get to an incredibly meaningful space with another person. (John Seely)
Theme: being present: spiritual reciprocity in the clinical encounter
It's hard to describe, but that feeling is within a person, within the resident and within the carer. (Assistant Ashley)
It's that sense of simply witnessing, simply continuing to show up in life. (Mary Vachon)
Just being. Just being with them. (Nurse Sharon)
Theme: the essence of being: defining presence
I think my spirituality connects when I am non-judgmental, show love, show compassion… Those times I was able to express or feel love and compassion for everyone else and in those times you feel your heart is expanding, your self is expanding, and I could recognize that was happening. (John Seely)
Stop the iatrogenic suffering, meaning both the suffering that you experience and the suffering you project onto the patient. How you speak and how you conduct yourself, can contribute to suffering… Being non-judgmental is a huge part of it…. When I’m not self-conscious is when I totally feel most connected. (David Kuhl)
If we have to choose we will err on the side of compassion. (Chaplain Ellen)
Being vulnerable
An essential ingredient within participants' conceptualisation of presence was vulnerability. Vulnerability allowed participants to recognise their shared humanity with patients, requiring them to temporarily put their white coats, titles, professional and personal credentials aside in order to interact with each patient as a fellow human being. In participant's recalling instances of excellence in the provision of spiritual care, they identified a willingness to acknowledge and occasionally disclose personal vulnerability as an essential factor. Participants indicated that although their sense of vulnerability did not diminish over time, their capacity to cope increased through clinical exposure. Three subthemes emerged: professional vulnerability, personal vulnerability and the effect of vulnerability on spiritual care.
Professional vulnerability: relinquishing the expert model
Entering the place of shared humanity – where the tough questions of life and death were raised and rarely answered – was described by the majority of participants as a deeply uncomfortable experience. While participants acknowledged initial discomfort in relinquishing their roles as experts, ironically, this was identified as underpinning effective spiritual care at the bedside and the spiritual growth of clinicians.
Personal vulnerability: the precursor of presence
Whereas professional vulnerability involved encountering their shared humanity with patients, personal vulnerability involved a deeper process, whereby participants attempted to integrate the life lessons of their patients into their personal lives. Caring for dying people caused participants to reflect on their own mortality and the mortality of those closest to them6. Participants identified personal vulnerability as an antecedent to effective use of presence in spiritual care.
The effect of vulnerability on spiritual care
Participants felt that personal vulnerability, including death-related fears and life questions, informed and enhanced their care for patients. The perceived therapeutic effect of professional and personal vulnerability within the clinician–patient relationship was described by clinicians as a sacred relational space or place of healing, where patients' spiritual resources and distress could be effectively engaged.
Being present: spiritual reciprocity in the clinical encounter
Awareness of their own presence allowed participants to attune to the patient's presence, allowing participants to feel that they were more attentive to their patients' needs in the clinical encounter. This extrasensory perception was born out of an intentional, yet non-prescriptive desire for participants to deeply connect to their patient's essence in each moment, without a need to provide answers, direct the conversation or have a specific predefined end point.
The essence of being: defining presence
The majority of participants found presence at the bedside difficult to describe. When participants were asked to articulate what they considered to be the key components of presence, this inevitably led to discussions of healthcare professionals' virtues and vices – the intrinsic qualities that the care giver brings to the clinical encounter. Participants identified virtues of hope, compassion and acceptance in their descriptions of presence and at the same time included darker attributes of despair, apathy and disregard. They felt both virtues and these darker attributes had an equal, albeit opposite effect, on the patient's spiritual well-being.
Discussion
This study is consistent with the findings of earlier studies exploring the spiritual needs of patients. These publications describe qualities related to clinicians' presence as essential in quality spiritual care.34,–,44 The current study builds on this knowledge through its focus on participants' perspective and practice of spiritual care; its cross-sectional and interdisciplinary sample of national leaders and frontline clinicians; and its design which attempts to suspend assumptions regarding spiritual care, allowing participant perspectives to inform the data.
Addressing spiritual needs has been identified as an important aspect of comprehensive cancer care, especially at the end of life.1,–,5 ,9 ,23,–,26 Clinicians are given little clinical guidance however on specifically how to effectively provide spiritual care at the bedside.2 ,3 In essence, experienced leaders and clinicians working at the end of life felt the role they played in the provision of spiritual care had less to do with professional training or prescriptive technique and more to do with their distilled spiritual beliefs permeating their presence and senses in the clinical encounter.10 ,17 ,18 ,34,–,42 The literature also indicates that presence plays a significant role in shaping patient outcomes and complaints in general.18 ,33 ,45,–,49 While the relevance of presence to effective communication, spiritual care and psychosocial care is self-evident, this study affirms the central role of clinician presence in interactions with patients across all care domains in end of life care.3,–,37 ,45 ,50
This study suggests that clinicians are involved in spiritual care less by their willingness and aptitude and more by the intrinsic qualities and spiritual beliefs they bring to the clinical encounter. The precise contents of clinicians' and patients' spirituality were identified by participants as secondary to their effects in the clinical encounter, whether their beliefs were rooted in humanism, religion or spirituality.51 ,52 This study suggests that clinicians may be better equipped at the bedside if they develop a reflective practice, exploring the impact of their intrinsic qualities and spiritual beliefs in clinical care: as the medium, in relation to spiritual care, is the message.53
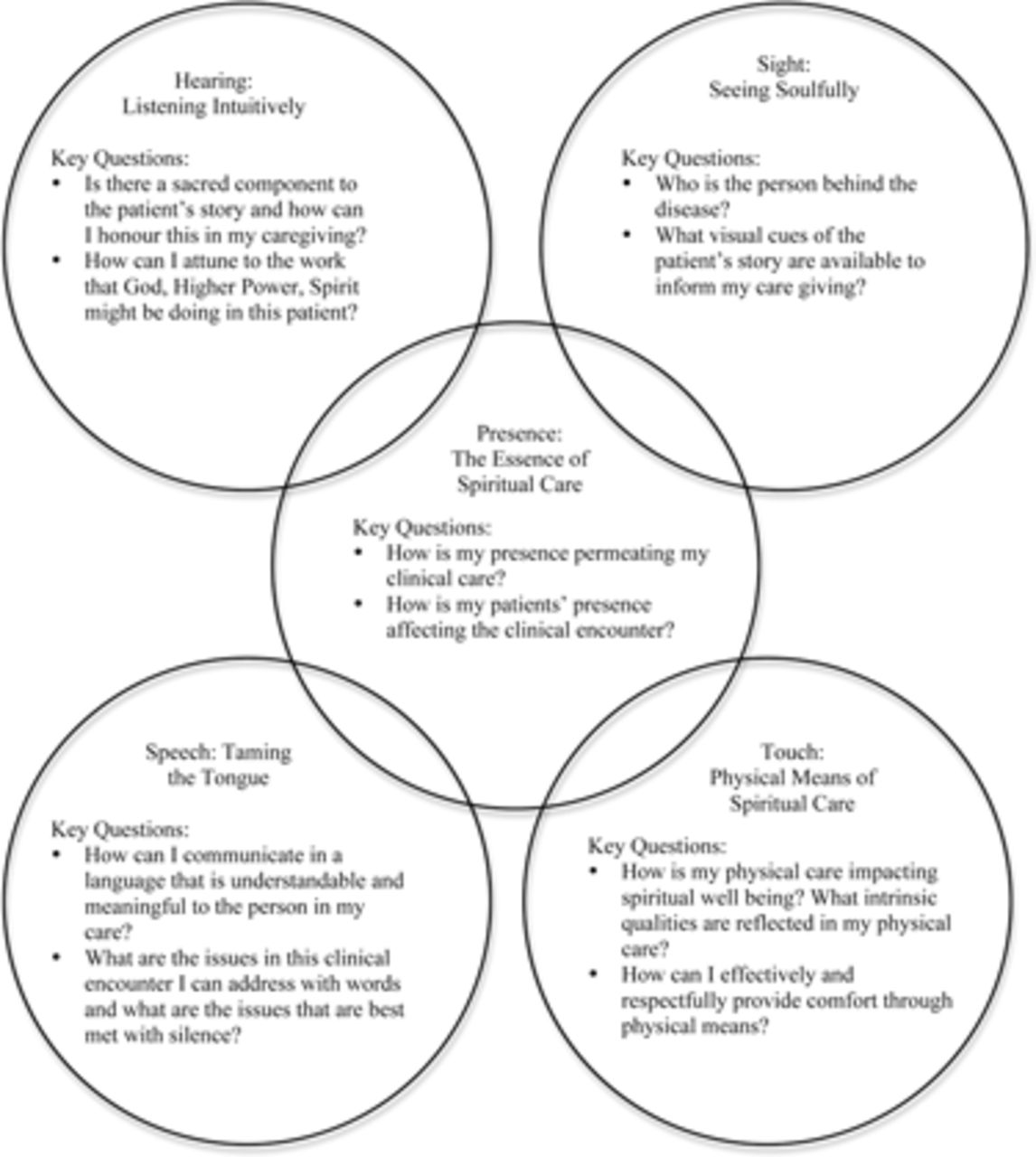
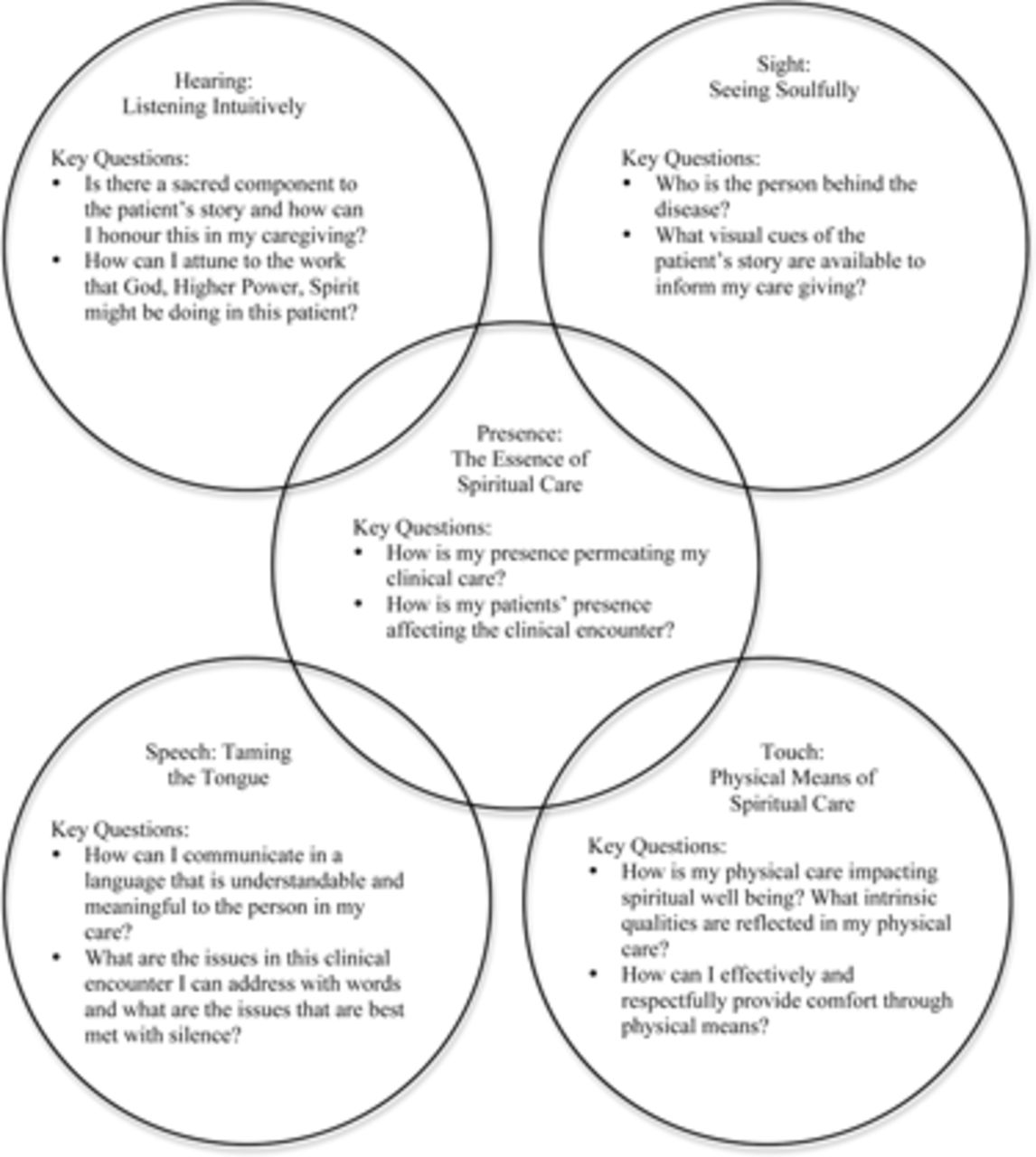
Although each clinician's personal spiritual beliefs will likely be as diverse as that of their patients, participants felt their beliefs informed clinical practice through five bedside skills. The five senses of spiritual care model (Figure 1) and associated key questions (box 7) are based on the five categories: hearing, seeing, speech, touch and presence, and their respective themes and subthemes that emerged from the qualitative analysis (table 2). While this framework may initially seem simplistic, its application in clinical practice is more challenging, as tacit skills are known to be difficult to incorporate within the demands of clinical practice.10 ,17 ,18 ,34 ,38,–,42 ,54 ,55
{kind=link}
The five senses of spiritual care.
The five senses of spiritual care
Hearing: listening intuitively
Key questions
Is there a sacred component to the patient's story and how can I honour this in my care giving?
How can I attune to the work that God, Higher Power, Spirit might be doing in this patient?
Sight: seeing soulfully
Key questions
Who is the person behind the disease?
What visual cues of the patient's story are available to inform my care giving?
Presence: the essence of spiritual care
Key questions
How is my presence permeating my clinical care?
How is my patients' presence affecting the clinical encounter?
Speech: taming the tongue
Key questions:
How can I communicate in a language that is understandable and meaningful to the person in my care?
What are the issues in this clinical encounter I can address with words and what are the issues that are best met with silence?
Touch: physical means of spiritual care
Key questions:
How is my physical care impacting spiritual well-being? What intrinsic qualities are reflected in my physical care?
How can I effectively and respectfully provide comfort through physical means?
This study has several limitations. It assessed perspectives on spiritual care using an interdisciplinary sample of palliative care professionals which may not be the same as advanced bedside skills employed by experienced spiritual care professionals. Study participants worked exclusively at the end of life; therefore, their perspectives do not necessarily reflect those of healthcare professionals working in other clinical settings. Finally, this cross-sectional study aimed to provide a Canadian perspective and may not be generalisable to other countries or cultures. Further research is required to determine the validity and utility of this conceptual model – and whether or not it helps enable healthcare providers to provide more effective spiritual care.
While spirituality is a burgeoning field in healthcare, with a growing evidence base, clinicians have been given little guidance on how to incorporate this vital domain of care into their clinical practice. This qualitative study identified five bedside skills that are core to the provision of spiritual care: listening, sight, touch, speech and, above all else, presence.
Acknowledgments
The authors would like to gratefully acknowledge the participants in this study, including the key leaders: Dr Balfour Mount, Dr Michael Kearney, Dr David Kuhl, Dr John Seely, Dr Mary Vachon and Jeremy Wex. This work was supported through a Canadian Institutes of Health Research-Wyeth Pharmaceuticals postdoctoral fellowship at the University of Manitoba.
References
Footnotes
-
Competing interests None.
-
Ethics approval Approval provided by the Conjoint Health Research Ethics Board of the University of Calgary, the Ottawa Hospital Research Ethics Board and the Fraser Health Research Ethics Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement These data are a subset of a larger ethnographic study investigating the spirituality of palliative care professionals in Canada which was the topic of Dr Shane Sinclair's PhD Thesis. The thesis is available through the University of Calgary.