Article Text

Abstract
Objectives The objective was to describe the prevalence of sexually transmitted infections (STI) and blood-borne viruses (BBV), and prophylactic treatment offered to female postpubertal patients attending a Norwegian Sexual Assault Centre (SAC). We wanted to evaluate whether STIs diagnosed at the initial visit could have been assault-transmitted, and to explore whether background and assault characteristics were associated with diagnosed STI/BBV.
Methods We included postpubertal females ≥12 years of age attending the SAC within 1 week of the assault. Data were collected from records. We conducted a retrospective, descriptive study, and used logistic regression analysis.
Results Among 412 patients with a median age of 21 years, 35 patients had an STI (8.5%), two of which probably were assault-transmitted. Chlamydia trachomatis was the dominating agent, detected in 25 patients (6.4%). At serology screening, 3.7% tested positive for hepatitis C and/or hepatitis B core antibody. Patient age 16–19 years was associated with STI, while BBV positives were older. Non-Western assailant was associated with STI, while substance abuse was associated with STI and BBV. In order to prevent potential transmission of STI not identified at the initial visit, 91% accepted prophylaxis against bacterial STI, while antiviral prophylaxis was offered to less than one-fifth of the patients.
Conclusions The C trachomatis prevalence among the sexual assault patients was lower than in a comparable clinical population. The STI was suspected to be assault-transmitted in only two cases.
- SEXUAL ASSAULT
- SEXUAL HEALTH
- HEPATITIS B
- HEPATITIS C
- WOMEN
Statistics from Altmetric.com
Sexually transmitted infections (STI) and blood-borne viruses (BBV) may be transmitted during sexual assault. Consequently, many victims of sexual assault contact healthcare because they fear acquiring infections. Several countries have established multidisciplinary specialised healthcare units for victims of sexual assault, called sexual assault centres (SAC), which offer examination and prophylaxis for STIs/BBVs in addition to forensic examination and psychosocial care.1–3 Existing guidelines diverge on whether and when to test for infection, as well as on the recommendations for postexposure prophylactic treatment of STIs and BBVs after sexual assault,4–8 since among other factors the local prevalence and antibiotic resistance pattern varies.
Among victims of sexual assault, prevalence rates between 0% and 33% have been reported for STIs,1 ,9–18 and between 0% and 14% for BBV markers.1 ,9 ,10 ,12 ,14 ,16 ,19 Studies of sexual assault victims differ regarding which conditions to include, mode of detection, and whether they report the prevalence of STIs/BBV markers from examination at the initial SAC visit,9 ,10 ,14 ,15 ,19 from follow-up consultations at the same clinic,1 ,13 ,18 or from referrals to specialised sexually transmitted diseases (STD) clinics.11 ,12 ,16
Furthermore, most of these studies do not discriminate between pre-existing and assault-transmitted STI. Exceptions to this are studies that either report the numbers of infected patients with no prior coital experience or follow-up studies where prophylactic treatment is withheld at initial visit.9 ,13 ,18 The latter may be regarded as controversial, given the low follow-up rate among SAC patients.1 ,15 ,17 ,20
So far, there are few studies reporting STI and BBV prevalence from SACs in the Nordic countries, where the prevalence of certain infections, such as Neisseria gonorrhoeae, Trichomonas vaginalis and HIV is low. On the other hand, the Scandinavian countries report equally high levels as other Western countries of Chlamydia trachomatis and the more recently diagnosable sexually transmissible agent Mycoplasma genitalium.21 ,22
The objective of this study was to describe the prevalence of STIs and BBVs among female postpubertal patients who attended the Trondheim SAC within 1 week of the assault, and to describe the prophylactic treatment offered. We wanted to evaluate whether any of the STIs diagnosed at the initial visit could have been assault-transmitted, and to explore whether background and assault characteristics were associated with diagnosed STI/BBV.
Methods
Study design, settings and participants
This retrospective, descriptive study comprises female patients ≥12 years old examined at the SAC at St Olavs Hospital, Norway, between 1 July 2003 and 31 December 2010. A more detailed description of the centre is given elsewhere.23 ,24 The Regional Committee for Medical and Health Research Ethics approved the study.
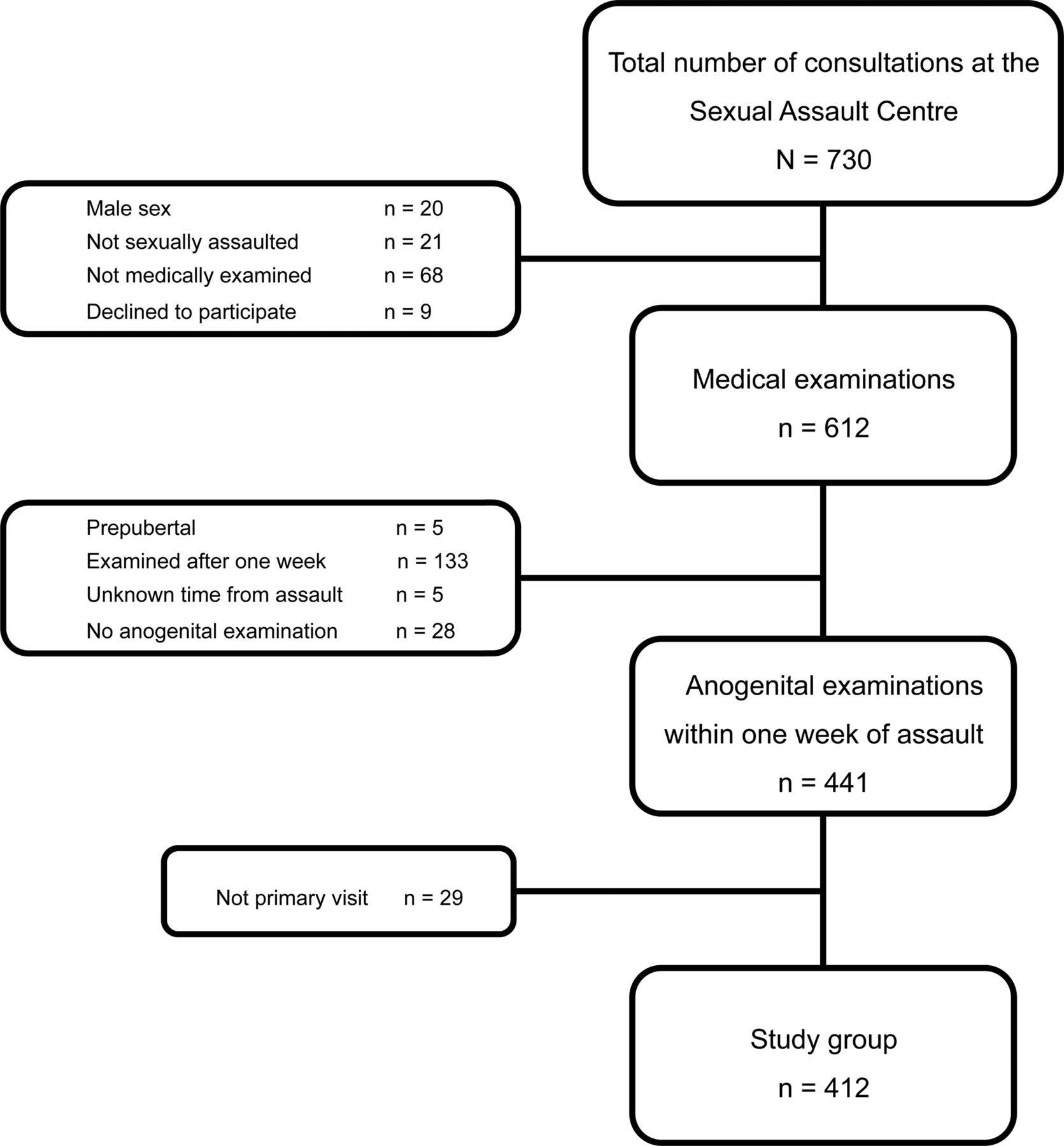
Altogether, 730 individual hospital consultations regarding recent sexual assault were identified from the study period. Males, those with no suspected sexual assault, and those not medically examined, were excluded (figure 1). All patients eligible for inclusion received a letter of information about the study with instructions on how to withdraw their information; those who did were excluded. We also excluded those recorded as prepubertal, those who appeared at the SAC more than 7 days after the assault, those with missing information regarding interval since assault, as well as those who did not undergo anogenital examination. Only the first visit for each patient was included, resulting in a study group of 412 patients.
{kind=link}
Flow diagram showing the inclusion and exclusion of subjects in the study of the 412 sexually assaulted female patients ≥12 years of age finally included.
Data collection and variables
Information from the patients’ medical records, including microbiological and serological test results, was registered through a web-based data collection system developed and administered by the Unit of Applied Clinical Research at the Norwegian University of Science and Technology.
Sociodemographic patient characteristics, such as age, occupation, country of origin (as previously defined),23 vulnerability factors (previous sexual assault, history of former/current alcohol/substance abuse (henceforth called substance abuse), and former/current mental health problems, as previously defined),23 prior coital experience, time since last consensual coitus, prior pregnancy and use of contraceptives, were recorded. Assault and assailant characteristics, including the time of assault, were recorded.
We noted the time of the clinical examination at the initial SAC visit and descriptions of anogenital injuries (excluding redness and/or swelling), as well as whether a full speculum examination or only inspection of the anogenital area was performed. The presence of spermatozoa on microscopy was recorded. The event was recorded as police-reported if the patient said so or if the police requested a medical report.
We recorded whether any prophylactic treatment was given at the initial visit according to Norwegian guidelines: for example, a one-dose regimen of oral azithromycin, hepatitis B vaccination and/or HIV postexposure prophylaxis (PEP).
Sampling and laboratory analysis, assault-transmission
Secretions from the urogenital (cervix and/or vagina), anorectal, and/or pharyngeal area were collected for microbiological examination (for N gonorrhoeae, C trachomatis, and from 2008, M genitalium) using swabs. From 2005, a first void urine (FVU) sample was alternatively offered for examination of C trachomatis (and, from 2008, M genitalium). If clinically indicated, specimens for additional microbiological agents, for example, T vaginalis or herpes simplex virus (HSV), were collected. At least one microbiological test was performed in 396 patients (table 1). Anogenital warts were clinically diagnosed.
Microbiological initial visit test results from 412 female victims attending the Trondheim Sexual Assault Centre within 1 week of assault
The Department of Medical Microbiology, St Olavs Hospital, examined all swabs and urine samples. C trachomatis, M genitalium and HSV were diagnosed by nucleic acid amplification test (NAAT) (Amplicor, Roche Molecular Systems for the former, and in-house real-time PCR assays for the latter two). All positive tests were reproducible by retesting. Standard culture techniques were used for the detection of N gonorrhoeae and T vaginalis.
A blood sample from all consenting patients was screened for serological markers of BBVs: HIV (HIVAg/Ab Combo test), hepatitis B (hepatitis B surface antigen (HBsAg), hepatitis B core antibody (HBcAb), and occasionally hepatitis B surface antibody (HBsAb)), hepatitis C antibody (HCVAb) (all hitherto Architect, Abbott), syphilis (Treponema pallidum antibody) (Bio-Rad, Murex, and Abbott), and occasionally HSV antibody. If not previously verified, positive screening tests were confirmed by alternative tests (HBsAg by neutralisation or PCR (Roche), and HCV by Chiron recombinant immunoblot assay (RIBA) HCV 3.0 (Novartis)). Altogether, 381 individual blood samples were collected for serological screening for markers of BBVs at the initial visit (table 1).
The STI was considered assault-transmitted when the patient testing positive had no prior coital experience and, for HSV, a positive swab NAAT was followed by HSV seroconversion.
Statistical analyses
Descriptive characteristics were described by frequencies and proportions for categorical variables, and by median and ranges for continuous variables. Associations between diagnosed STI/BBV and independent categorical variables were explored by binary logistic regression analyses. To adjust for patient age, we used multivariable logistic regression analysis without stepwise selection; for the BBV associations, we also adjusted for substance abuse. Statistical significance was assumed when p<0.05. Missing data were calculated, but mostly excluded. All statistical analyses were performed in SPSS V.19.0.
Results
Table 1 presents the number of patients testing positive in proportion to the number of patients tested for each of five microbes at the initial visit. C trachomatis was detected in 25 patients (6.4% of the 393 patients tested), one of whom had no prior coital experience. Two patients tested positive for M genitalium (1.9% of the 106 patients tested). One of two patients with genital lesions tested positive for HSV: this infection was probably assault-transmitted. Eight patients (1.9%) had visible anogenital warts. At least one STI was diagnosed in 35 patients (8.5%). Only one patient had more than one STI, testing positive for C trachomatis and demonstrating genital warts.
Stratifying patients by age groups, we found a C trachomatis prevalence of 11% (15/139) among 15–19-year-olds, and 5% (6/129) among 20–24-year-olds. There was no difference in the year-by-year prevalence of C trachomatis.
Table 1 also describes the number of patients testing positive for BBV markers at the initial visit. Seven patients had serological markers compatible with prior hepatitis B infection, while nine were HCVAb positive. A total of 14 patients (3.7%) tested positive for at least one BBV. Two patients tested positive for HBcAb and HCVAb, and one for HCVAb and M genitalium.
Patient characteristics are outlined in table 2. Patients’ median age was 20.8 years (range 12.8–61.2). One or more vulnerability factor was present in 232 patients (56%): substance abuse was reported by 42 patients (10%), 174 (47%) had mental health problems, and a further 147 (41%) had suffered a previous sexual assault. A total of 222 patients (54%) did not use any contraception, while eight (1.9%) habitually used condoms. Some assault and assailant characteristics are shown in the supplementary e-table.
STIs* disclosed at initial visit: characteristics and clinical variables of 412 female victims attending the Sexual Assault Centre within 1 week of the assault by presence of STI, crude and age adjusted OR with corresponding 95% CI presented
Table 2 also presents crude and age-adjusted OR with corresponding 95% CI for the association of victim characteristics and STI. Those diagnosed with an STI were more often in the 16–19-year-old age group. After adjusting for age, those diagnosed with an STI more often reported substance abuse and assailant(s) of non-Western origin. No other assault characteristic was associated with the diagnosis of STI (see supplementary e-table).
Table 3 describes crude and adjusted OR for the association of victim characteristics and BBV markers. Compared with those testing negative for at least one of the serological markers, those testing positive were older, more often unemployed, and more often reported substance abuse. Those patients testing positive who did not report substance abuse, one of them of non-Western origin, were all positive for HBcAb only. Reported mental health problems or previous sexual assault had, after adjustment for age and substance abuse, no association with BBVs (data not shown).
Blood borne viruses (BBV)* disclosed at initial visit: characteristics of 381 female victims attending the Trondheim Sexual Assault Centre within 1 week of the assault by presence of BBV, crude and adjusted OR presented
After the examination, 374 patients (91%) accepted an oral one-dose regimen of azithromycin, 80 patients (19%) initiated hepatitis B vaccination, while 11 patients (2.9%) consented to HIV-PEP. Significantly more patients got hepatitis B vaccination as well as HIV-PEP when the assailant was reported to be non-Western, and if presenting in the period 2008–2010 (data not shown).
Discussion
Among the 412 female adult and adolescent patients attending the SAC, an STI was found in 35 patients (8.5%), two of which were probably assault-transmitted. C trachomatis was detected in 25 patients (6.4%) and at serology screening, 3.7% tested positive for HCVAb and/or HBcAb. Prophylaxis against bacterial STI was accepted by 91% of patients, while anti-viral prophylaxis was offered to less than a fifth. Patient age 16–19 years was associated with STI, while BBV positives were older. After adjusting for age, a non-Western assailant was associated with STI, while substance abuse was associated with STI and BBV.
We found a lower C trachomatis prevalence than reported in other studies of postpubertal sexual assault victims.9 ,11 ,13 ,15 ,16 ,18 ,20 Given the diversity of these studies, comparable studies should at least be extracted from the same time period as the present,9–11 ,15 ,17 ,20 ensuring that C trachomatis is diagnosed by NAAT. Other factors known to influence prevalence, such as geographical region, ethnicity, age range and sex of the victims, as well as whether or not to include non-penetrative assaults, vary across the studies. The lowest C trachomatis prevalence (5%) was reported in a US study of postpubertal raped females <19 years of age.10 In two European studies, one from a Belgian emergency unit staffed by gynaecologists, and the other from a London STD referral clinic, the median age was higher than in the present study15 ,20; still, prevalence of C trachomatis was as high as 8–9%. This could possibly reflect the mixed ethnic background of the patients, since both studies reported a high proportion of non-Caucasians. The only non-Western SAC study reporting C trachomatis prevalence is South Korean, where as many as 29% of patients tested positive. Although the victims’ mean age was comparable with the present study, the authors included only those reporting a history of penile penetration, thereby restricting the inclusion to certain types of assault.
Contrasting with the UK studies,11 ,16 ,17 ,20 but in accordance with the Belgian and US studies,10 ,15 we report C trachomatis prevalence from the initial SAC consultation. When the interval from assault to examination is brief, we assume that most infections diagnosed are pre-existing. An exception is STI diagnosed in patients with no prior coital experience. We found that one patient among the 31 with no prior coital experience was infected with C trachomatis, whereas the South Korean study found that 20% of the virgins were infected.9 Only two US studies conducted in the early 1990s have managed to estimate the C trachomatis transmission rate as a result of sexual assault, at 2–16%.13 ,18 Ideal studies of STI transmission after sexual assault should include initial and follow-up testing, withhold prophylactic antibiotic treatment, and collect information on consensual sexual activity in the period before and between testing. Additionally, recent preassault test results should be available and compared with the postassault results. Such a study design is challenging. We prioritised to prevent potential transmission of STI, and given the high acceptability of azithromycin and the low follow-up rate, all our patients were offered prophylaxis against bacterial STI. More than 90% received azithromycin, hence, rendering routine retesting for C trachomatis superfluous.
When the assailant was reported as non-Western, the victim more often had an STI. None of the other assault and assailant characteristics was associated with STI, again indicating that most of the STIs were pre-existing. We could not, however, exclude that some of the patients with prior coital experience contracted the infection during the assault, as NAAT is sensitive and will detect low levels when infected semen is caught in the swab. Assault characteristics may still guide the clinician regarding when to initiate antiviral prophylactic treatment.
We compared the C trachomatis prevalence found in the present study with the prevalence in the community, as well as in the clinical population. Two Norwegian studies among female volunteers <25 years of age have estimated the prevalence of C trachomatis at 2%.25 ,26 By contrast, according to a clinically based study from the catchment area of our SAC, the prevalence of C trachomatis was overall higher than that among the assault patients, as high as 16% among the youngest women (15–19 years) and 12% among those 20–24 years old.27 Furthermore, a UK study reported that the prevalence of STI among the sexually assaulted was no higher than in the routine clinical population.11 This knowledge contrasts with the assumption that sexual assault victims generally have higher risk of STI.
None of our patients tested positive for HIV at the initial visit. Except for a recent South African study which reported a prevalence of HIV positivity as high as 14% among more than 1400 patients attending a local SAC,19 HIV prevalence among SAC patients in Kenya, South Korea, US and Europe has been less than 2.5%.1 ,9 ,10 ,13–16 In the present study, we only detected markers of hepatitis B and C suggestive of prior infection. Other SAC studies reporting markers of hepatitis B and C have found similarly low rates, although not all include details about the markers tested for.1 ,10 ,14–17 Generalising our results to other SACs is therefore difficult.
It is not known whether exposure to hepatitis B and C infections are more common among our patients reporting sexual assault than in the general Norwegian population. In two studies among women pregnant during the 1990s, a prevalence of HCVAb of only 0.2–0.7% was found,28 ,29 while the prevalence of HBcAb in the general Norwegian population has not been published.
We found that substance abuse was reported by as many as 11 of our 14 BBV-positive patients at the initial visit. Although our study did not include details on type of drug abused, a recent study has found particularly high prevalence of hepatitis C and B infection among injectional and non-injectional drug users in Stockholm.30 It therefore seems likely that this specific risk group is responsible for the high prevalence of BBVs among our SAC patients. This is also in accordance with the Norwegian Institute of Public Health, which states that ethnic Norwegians usually contract hepatitis B by injecting drugs. Hepatitis B vaccination should, therefore, be liberally offered to SAC patients, and we found that this was offered more frequently in the latter half of the study period, according to a change in the guidelines in 2007.
One of the strengths of this study is the close access to medical records, allowing us to combine detailed clinical information with laboratory findings. The design enables us to characterise differences between STI/BBV positive and negative cases for several patient and assault characteristics usually not available in STI/BBV prevalence studies.
As the present study represents unselected female patients attending a SAC, it reflects the true prevalence of STI/BBV findings among them. However, many victims of sexual assault do not seek medical care,6 and our results are therefore not necessarily applicable to all Norwegian victims of sexual assault. Moreover, extrapolating our findings to other countries should be done with caution.23
Our study is hampered by the limitations of small sample size. Even if approximately 400 patients are included, some of the comparisons between STI/BBV positive and negative cases may have been subjected to type II statistical errors, especially when some of the outcome groups are small. For some variables, missing information is substantial. However, when we include those with missing data into the analyses, the results remain unchanged although some effects may be overestimated or underestimated.
Since this is a retrospective study using medical records as the sole source of information, data on some patient characteristics may be incomplete. Sensitivity for C trachomatis is generally high in urogenital swabs and FVU, although M genitalium detection could vary.22 Even if specificity is high regardless of sampled material, some of our patients might have undetected M genitalium infection. Further, limiting our N gonorrhoeae detection to culture could result in this infection being underdiagnosed as well. Further limitations are described elsewhere.23 ,24
This is the first study to explore prevalence of STI/BBV from Norwegian postpubertal females after sexual assault. The C trachomatis prevalence found here is higher than in the community but lower than in the comparable clinical population. In only two cases the STI was suspected to be assault-transmitted. Assault characteristics may guide the clinician when to initiate antiviral prophylactic treatment. The possibility of testing suspected assailants should be explored.
Key messages
-
Chlamydia trachomatis prevalence among the sexual assault victims was notable, but lower than in the comparable clinical population.
-
Differentiating sexually transmitted infections (STI) transmitted during assault from pre-existing STI is difficult, and in only two cases the STI was suspected to be assault-transmitted.
-
STI prevalence was highest among 16–19-year-old patients, while blood-borne virus (BBV) positives were older; substance abuse was associated with STI and BBV.
-
Assault characteristics may guide the clinician's decision about when to initiate antiviral prophylactic treatment, but were usually not associated with diagnosed STI.
Acknowledgments
Berit Marianne Bjelkåsen at the Unit of Applied Clinical Research at the Norwegian University of Science and Technology has kindly provided the web-based registration form and converted it to an SPSS-file. Thanks to the students Katharina Frydendal Pedersen, Karen Løhre and Anna Hjorth-Hansen who participated in the registration of the data.
References
Supplementary materials
Abstract in Norwegian
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online eTable
Footnotes
Handling editor Jackie A Cassell
-
Contributors CTH is the main author. She made substantial contributions to study design, data collection and registration of the data from hospital files, data analyses, interpretation of data, and to the drafting and revision of the manuscript. BS was the initiator of the study and SAN contributed to laboratory data collection. All coauthors contributed to study design, interpretation of the data and to the drafting and revision of the manuscript.
-
Funding The Norwegian ExtraFoundation for Health and Rehabilitation through the NGO Norwegian Women's Public Health Association, and The Liaison Committee between the Central Norway Regional Health Authority (Helse Midt-Norge) and the Norwegian University of Science and Technology.
-
Competing interests CTH received funding from the The Norwegian ExtraFoundation for Health and Rehabilitation through the NGO Norwegian Women's Public Health Association (grant number 2008/2/0241), as well as from The Liaison Committee between the Central Norway Regional Health Authority (Helse Midt-Norge), and the Norwegian University of Science and Technology (grant number 2010/14281).
-
Ethics approval Regional Committee for Medical and Health Research Ethics, Central Norway.
-
Provenance and peer review Not commissioned; externally peer reviewed.