Article Text

Abstract
Objectives: One of the two new human papillomavirus (HPV) vaccines protects against HPV types 6 and 11, which cause over 95% of genital warts, in addition to protecting against HPV types 16 and 18. In anticipation of HPV vaccine implementation, the impact of genital warts on health-related quality of life (HRQoL) was measured to assess the potential benefits of the quadrivalent over the bivalent vaccine.
Methods: Genitourinary medicine clinic patients aged 18 years and older with a current diagnosis of genital warts were eligible; 81 consented and were interviewed by a member of the research team. A generic HRQoL questionnaire, the EQ-5D (comprising EQ-5D index and EQ visual analogue scale (VAS) scores) and a disease-specific HRQoL instrument, the CECA10, were administered. Previously established UK population norms were used as a control group for EQ-5D comparisons.
Results: Cases (with genital warts) had lower EQ VAS and EQ-5D index scores than controls. After adjusting for age a mean difference between cases and controls 30 years of age and under (n = 70) of 13.9 points (95% CI 9.9 to 17.6, p<0.001) for the EQ VAS and 0.039 points (95% CI 0.005 to 0.068, p = 0.02) on the EQ-5D index (also adjusted for sex) was observed. The difference between cases and controls for the EQ VAS was especially notable in young women.
Conclusions: Genital warts are associated with a significant detriment to HRQoL. The potential added benefit of preventing most cases of genital warts by HPV vaccination should be considered in decisions about which HPV vaccine to implement in the United Kingdom.
Statistics from Altmetric.com
In October 2007 the Department of Health, UK, announced the introduction of a national human papillomavirus (HPV) immunisation programme, to commence with the vaccination of 12–13-year-old girls from September 2008.1 Two HPV vaccines are now potentially available in the United Kingdom, although no guidance has been offered at the time of writing about which of the two vaccines should be administered. Both vaccines protect against HPV types 16 and 18, which cause over 70% of cervical cancer cases worldwide.2 One of the vaccines also protects against HPV types 6 and 11, which cause more than 95% of genital warts.3 The study presented here was carried out to inform the decision about which vaccine to use.
Genital warts are the most commonly diagnosed viral sexually transmitted infection (STI) in the United Kingdom. In 2006 over 80 000 first episode diagnoses were made in 2006 in genitourinary medicine (GUM) clinics alone.4 The estimated peak incidence among 20–24-year-old men is 794/100 000 and 767/100 000 in 16–19-year-old women.5 The disease course may be protracted even with treatment. It has been estimated that at least 25% of cases recur within 3 months and episodes can vary from weeks to occasionally years in duration.6 Despite the heavy burden of disease, little research has been carried out to assess the impact of genital warts on health-related quality of life (HRQoL).7 A small number of studies has assessed the way in which people with genital warts are affected8–12 but few of these included a comparison group or were designed for use in economic analyses. One study asked female volunteers to rate the value of different health states related to HPV infection, but this did not collect data from individuals who actually had genital warts.13 One Canadian study has used the EQ-5D in 31 women with genital warts, as part of research into the cost-effectiveness of HPV vaccination.14 We are unaware of any such study having been carried out in the United Kingdom or Europe.
The potential for prevention through vaccination is considerable given that over 95% of genital warts can be attributed to HPV types 6 and 11.3 15 This study was conducted to provide data on the impact of genital warts on HRQoL, which could then be used in analyses of the cost-effectiveness of HPV vaccination. Generic measures of HRQoL can be used to compare outcomes across different health states and we therefore used one such instrument (the EQ-5D)16 to compare quality of life in patients with genital warts with that in the general population.
METHODS
Cases consisted of men and women attending the York GUM clinic during a 3-month period. Adults aged 18 years and over with a current diagnosis of genital warts were eligible. This included those attending for a first or follow-up visit. All GUM clinics in the United Kingdom collect data on the number of episodes of STI on a quarterly basis and each diagnosis is assigned a KC60 code.17 The codes for genital warts are C11A (incident cases), C11B (recurrent genital warts) and C11C (warts that persist for over 3 months). To prevent biasing the sample towards newly diagnosed cases, patients assigned any KC60 code were eligible. Consenting participants completed three questionnaires during an interview by a member of the research team at the time of recruitment: a study-specific questionnaire including demographic data, the EQ-5D and a disease-specific HRQoL tool, the CECA10.18 The control group was derived from UK general population reference values for the EQ-5D and accompanying self-reported health state scores.
The EQ-5D is a generic measure of HRQoL, widely used in economic evaluations, consisting of five dimensions. For each dimension, respondents indicate whether they have no, some or extreme problems in that area. All EQ-5D scores were converted into a weighted index from 0 to 1 (0, dead; 1, perfect health) using UK population preference values. The EQ-5D self-reported health state (EQ VAS) is a visual analogue scale in which respondents indicate their perceived health state at the time of answering on a scale from 0 to 100 (0, worst imaginable health state; 100, best imaginable health state). All UK population reference (control) values and preference scores were derived from the 1993 UK-TTO dataset provided by the EuroQol executive office.16
The CECA10 is a disease-specific HRQoL tool, consisting of 10 statements relating to the impact of genital warts on emotional and sexual wellbeing. Respondents indicate (using a five-point Likert scale) the extent to which they agree or disagree with each statement.18 The CECA10 was used to investigate what areas of life might be particularly affected by having genital warts and to explore the relationship between EQ-5D scores and the perceived impact of genital warts.
Wart severity was coded as “mild” (1–3 lesions), “moderate” (4–7 lesions) or “severe/multiple” (>7 lesions) according to the patient’s medical records, which were completed as normal throughout the study period.
Case and control data were truncated at the age of 30 years, as a result of the paucity of case data above that age (only 14% of cases were aged 31 years or over). EQ VAS scores were analyzed using generalised additive models to take into account non-linear age-related EQ VAS score effects. The difference between the case and control score was adjusted for age and interactions between age and case–control status. EQ-5D scores were analyzed with analysis of covariance with the difference between the case and control score being adjusted for age and sex. Model residuals were found to be non-normal; therefore confidence intervals were validated using studentised bootstrap confidence intervals. Differences among cases according to the KC60 code, wart severity and type of visit were tested using analysis of variance. Statistical analyses were performed using R version 2.6.0 and SPSS version 14.0. Generalised additive models were fitted with the mgcv library for R.19 20
RESULTS
Eighty-one cases (43 men, 38 women) were recruited, with a mean age of 26 years (table 1). The nature of the clinic environment meant it was not practical to record all instances of eligible patients declining an invitation to take part in the study. Although the exact response rate is therefore not known, KC60 statistical returns for the clinic show that 179 diagnoses of C11A, C11B or C11C were made during the study period. There were no significant differences in age or sex between our study population and the KC60-reported genital warts population. Our study sample included a higher proportion of patients with persistent warts compared with those receiving a genital warts diagnosis during the study period and a lower proportion of first episode cases (64% of the 179 KC60-reported genital warts population were diagnosed as C11A, 28% as C11B and 8% as C11C). The EQ-5D control group included 1977 people in the same age range as our sample (mean age 34 years). A total of 746 were aged under 30 years (318 men, 428 women) and this group had a mean age of 25 years.
When asked whether genital warts affected their quality of life, almost half of the cases answered “significantly” or “very significantly” (table 1). The unadjusted mean EQ-5D index score among all cases was 0.90 (compared with 0.91 for controls) and 72 (compared with 86 for controls) on the EQ VAS.
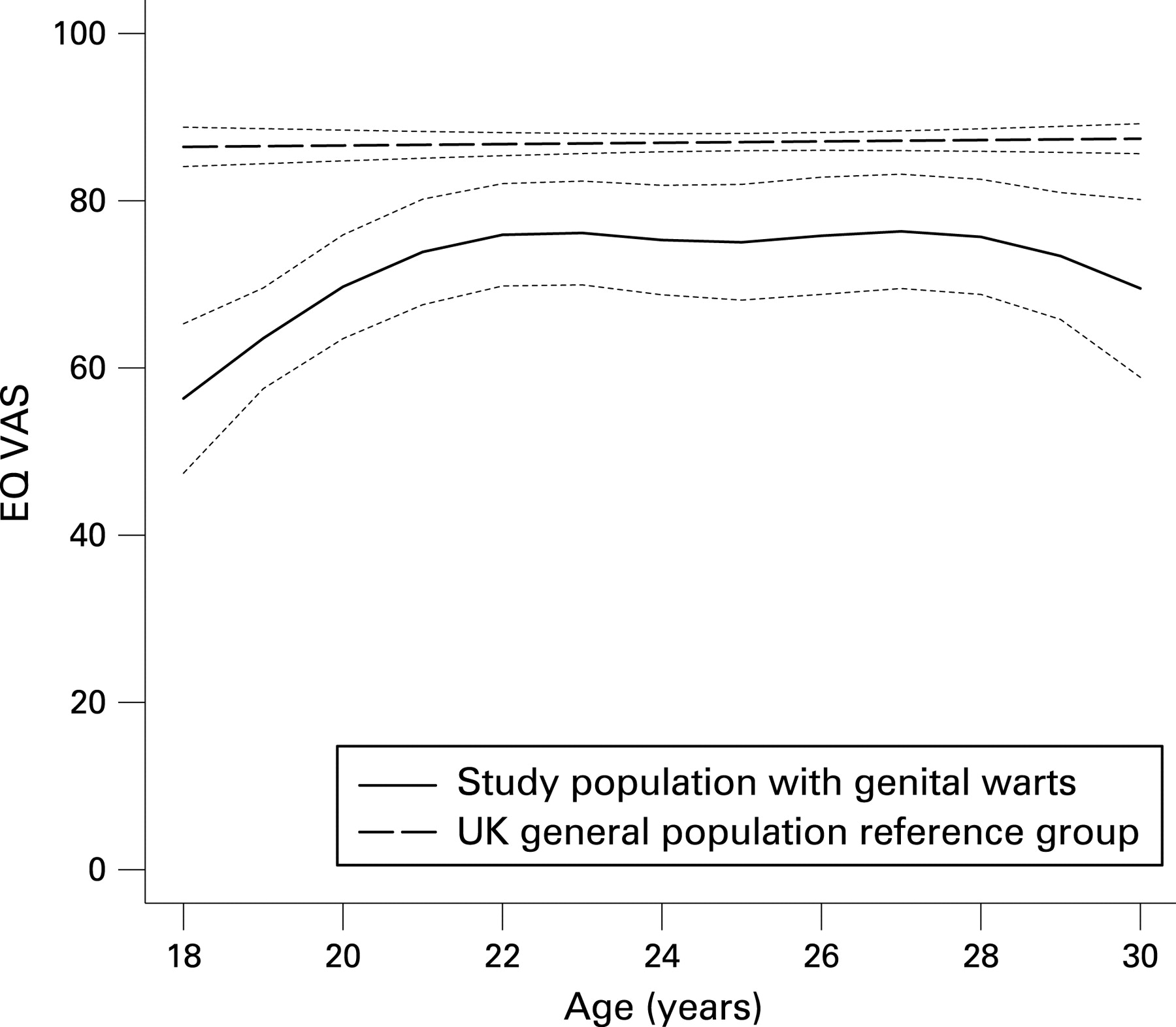
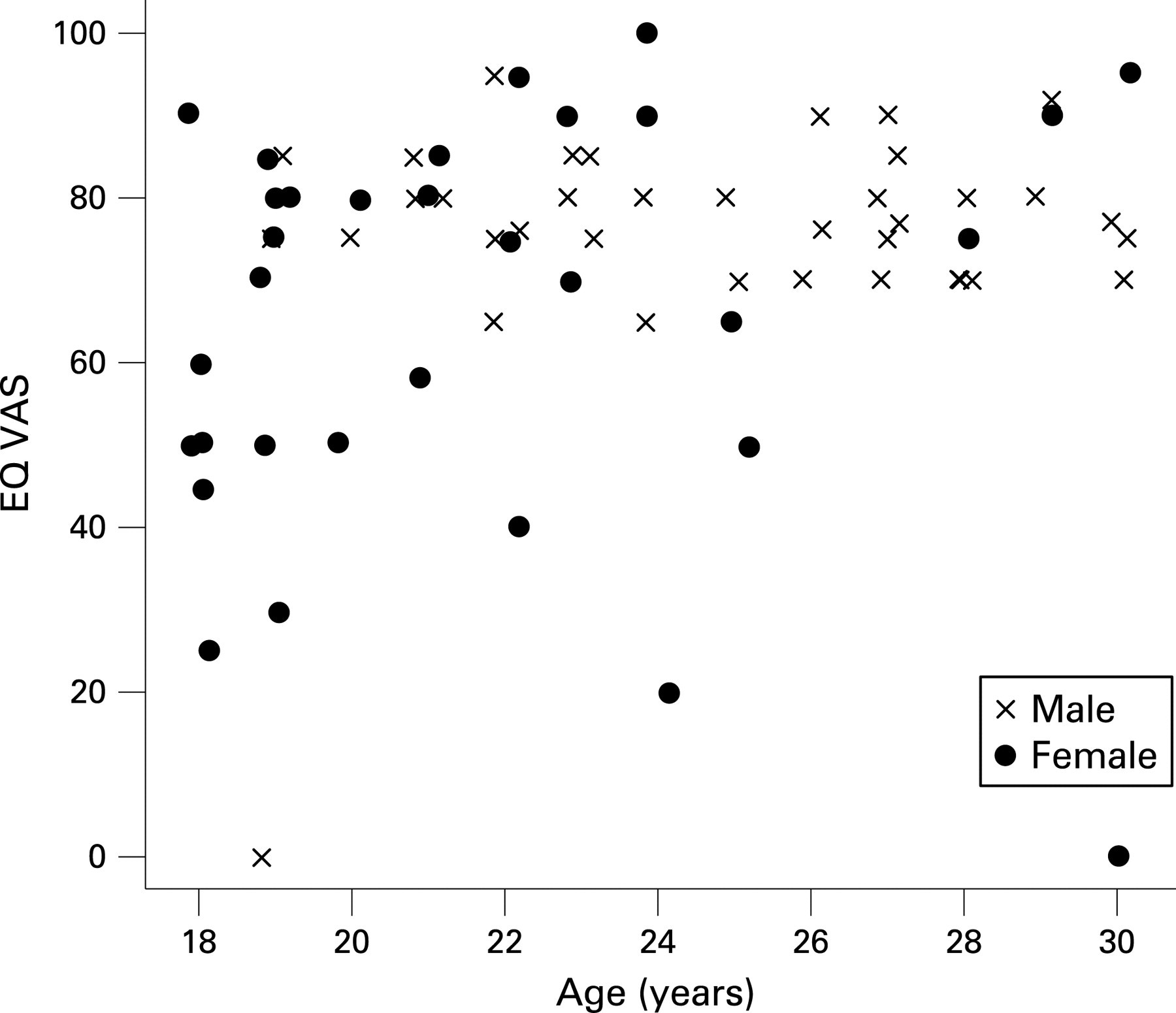
For EQ VAS scores, the fitted model (and 95% CI) adjusting the non-linear age effect is shown in fig 1. After truncating the data at the age of 30 years, compared with controls the EQ VAS was an average of 13.9 (95% CI 9.9 to 17.6) points lower among cases (p<0.001 based on 70 cases). Figure 2 shows the distribution of case scores by age and sex. Young women in the sample exhibit lower EQ VAS scores than men of the same age. After re-fitting the models for men and women separately, male cases had EQ VAS scores an average of 10.9 points (95% CI 5.7 to 15.5; p<0.001) lower than controls. Women had EQ VAS scores an average of 19.9 points (95% CI 11.7 to 26.2; p<0.001) lower than controls. The EQ-5D index was 0.039 points (95% CI 0.005 to 0.078; p = 0.02) lower among cases than controls when adjusted for age and sex. Among cases, the EQ VAS and EQ-5D scores did not differ significantly by KC60 code, wart severity or type of visit (either first or follow-up).


{kind=link}
{kind=link}
Table 2 shows responses for each dimension of the EQ-5D. Most of the detriment to HRQoL among the cases can be attributed to two dimensions of the EQ-5D: pain/discomfort and anxiety/depression. In response to the CECA10, cases indicated the highest level of agreement with the statements: “I am anxious to know whether I am going to recover from the infection for good” (mean 2.1, on a scale of 1 to 5, where 1 indicates complete agreement and 5 complete disagreement), “I feel worried during sexual relations” (mean 2.3) and “I worry about whether the warts will get worse or whether there will be some complications” (mean 2.3). Respondents reported the highest level of disagreement with the statement “Knowing that I have the illness affects me in my daily life” (mean 3.4). Compared with men, female cases had a lower mean score on every item of the CECA10. Women also had a higher, statistically significant level of agreement on two items of the CECA10: “My state of mind is upset” (p = 0.003) and “I avoid sexual relations” (p = 0.016) (full results provided in the Appendix). There was a moderate positive correlation between the EQ VAS and the CECA10 (r = 0.37, p<0.01). A weaker relationship was seen between the EQ-5D index and CECA10 scores (r = 0.26, p = 0.02).
DISCUSSION
We studied unselected cases of genital warts attending a GUM clinic in York, a city of approximately 200 000 population. We are not aware of any attributes of these cases that make them different to cases presenting at other centres in the United Kingdom. We observed slight differences in the proportions of new, recurrent and persistent cases in our total sample compared with data overall from England, but our sample aged 30 years or less appeared very similar to the national picture (York total versus York ⩽30 years versus England: C11A: 49%, 54%, 56%; C11B: 33%, 31%, 31%; C11C: 17%, 14%, 13%).5
People with genital warts reported a lower HRQoL than the reference sample of the UK population. This was especially evident for the EQ VAS score. The small number of studies carried out to date estimate between a 5% and 30% reduction in utility attributed to genital warts13 14 21 22 and the EQ-5D and EQ VAS results reported here are consistent with those estimates.
We found evidence to support the hypothesis that the detriment to HRQoL measured on the EQ VAS and EQ-5D index can be attributed to the current diagnosis of genital warts. First, the majority of the detriment to HRQoL measured on the EQ-5D registered in the anxiety/depression dimension. This is consistent with what is known about the experience of genital warts, in that most of the associated morbidity is thought to be psychological.8–12 The relationship between STI diagnosis and psychological impact may not be straightforward, as previous studies of patients attending sexual health clinics have shown high levels of psychological morbidity among those with and without an active diagnosis.8 23 The correlation in the cases with genital warts seen between the EQ VAS score, a generic measure, and the CECA10, a disease-specific measure (and to a lesser extent that between the EQ-5D index and CECA10), however, suggests that the detriment to HRQoL registered using the EQ-5D tool was associated with genital warts.
Key messages
Data on the effect of genital warts on HRQoL are needed for economic evaluation of HPV vaccination.
The burden of disease from genital warts is substantial, both in terms of the detriment to HRQoL, incidence of infection, cost of treatment and chronic nature of the condition.
The potential added benefit of preventing the majority of cases of genital warts by HPV vaccination should be considered in decisions about HPV vaccine implementation.
This is the first study to use a standardised measure of HRQoL in patients with genital warts in the United Kingdom and to compare these results with a UK population to quantify the extent to which genital warts affect an individual. As well as studies of sexual health clinic patients in general, a substantial body of research exists on the psychological impact of genital herpes in particular. Although herpes is a more painful condition than genital warts, both are viral, recurring and visible STI. As in our study of genital warts, genital herpes is associated with reduced HRQoL and a relatively high incidence of anxiety and depression.8 24–26 Those studies have also provided some evidence that the psychological impact of an STI diagnosis may be greater in women than in men.26 27 The origin of these differences is presently unclear but may be caused by factors such as concerns about sexual infectivity and reproductive health. Further research would be required to explore these issues more fully and to address the differential nature of perceptions of the diagnosis in men and women.
The main limitation of this study was the size of our case group. The study was only designed to look at an overall difference between cases and controls, and as such we were unable to investigate fully the potential impact of sex, KC60 code (including the oversampling of recurrent cases), wart severity or type of visit (first or follow-up) on HRQoL outcomes.
The EQ-5D index only registered a small difference in HRQoL between cases and controls. The EQ-5D was designed as a generic tool and may not have accurately captured the loss of HRQoL associated with having genital warts. The five dimensions of the tool are not as relevant to genital warts as they are to other conditions. An alternative generic tool is the Short Form 36, which covers a wider variety of domains, has been used successfully in genital herpes24 25 and may be more appropriate for future research in this area.
In order to understand better the impact of genital warts on HRQoL, information about the typical duration of an episode as well as the frequency of recurrence would be useful, but is beyond the scope of this report. In one study episodes of care were found to have lasted for an average of 3 months,28 but this did not include the period when individuals had genital warts but were not receiving treatment. A prospective study with active follow-up of incident cases of genital warts would be required to investigate this further, as well as to explore whether HRQoL changed over the course of an episode. The recurrent nature of genital warts and the potential for a single episode to persist for several months, or even years, means that even a small difference in HRQoL caused by genital warts could have a considerable impact on the loss of quality-adjusted life-years.
The burden of disease from genital warts is substantial, both in terms of the incidence of infection, cost of treatment,29 30 the chronic nature of the condition and, as demonstrated by this study, the detriment to HRQoL attributable to genital warts. The potential added benefit of preventing the majority of cases of genital warts by HPV vaccination should be considered in decisions about which HPV vaccine to implement in the United Kingdom.
Acknowledgments
The authors would like to thank the clients and the staff at Monkgate Sexual Health Clinic, York, for making the study possible, Professor Paul Kind for his advice on the use of EQ-5D, the EuroQol executive office for the provision of the UK population norms dataset, and Dr Xavier Badia for his permission to use, and assistance with, the CECA10.
Appendix
REFERENCES
Footnotes
Contributors: CJNL was the chief investigator for the study. SW, CJNL, MJ, WJE and RN designed the study. SW, TR and CC carried out the data collection. SW and SC performed the statistical analyses. SW wrote the manuscript with contributions from all authors.
Funding: This work was supported by funding from a Department of Health Grant “Studies to inform the design, implementation and monitoring of a human papillomavirus vaccination programme in England”, grant no 039/0030. The funding body were not involved in the design of the study, nor the analysis or write-up and were not involved in the decision to submit the manuscript.
Competing interests: None.
Ethics approval: The study was approved by the South Humber Research Ethics Committee.
Linked Articles
- Brief encounters
- Correction