Article Text

Abstract
Objective: To determine the extent of testing, diagnostic episodes and management of genital Chlamydia trachomatis (CT) infection in UK primary care using a large primary care database.
Methods: The incidence of CT tests, diagnostic episodes, treatments and referrals was measured for all adult patients in the General Practice Research Database between 1990 and 2004.
Results: Rates of CT testing in those aged 12–64 years in 2004 increased to 1439/100 000 patient years (py) in women but only 74/100 000 py in men. Testing rates were highest among 20–24-year-old women (5.5% tested in 2004), followed by 25–34-year-old women (3.7% tested in 2004). 0.5% of registered 16–24-year-old women were diagnosed as having CT infection in 2004. Three-quarters of patients with a recorded diagnosis of CT had had an appropriate prescription issued in 2004, a proportion that increased from 1990 along with a decrease in referrals to genitourinary medicine. In 2004, general practitioners treated 25.0% of all recorded diagnoses of CT in women and 5.1% of those in men.
Conclusions: Testing for and diagnostic episodes of CT in primary care have increased since 1990. Testing continues disproportionately to target women aged >24 years. Extremely low rates of testing in men, together with high positivity, demonstrate a missed opportunity for diagnosis of CT and contact tracing in general practice.
- CT, Chlamydia trachomatis
- GP, general practitioner
- GPRD, General Practice Research Database
- GUM, genitourinary medicine
- NCSP, National Chlamydia Screening Programme
- OXMIS, Oxford Medical Information System
- STI, sexually transmitted infection
Statistics from Altmetric.com
- CT, Chlamydia trachomatis
- GP, general practitioner
- GPRD, General Practice Research Database
- GUM, genitourinary medicine
- NCSP, National Chlamydia Screening Programme
- OXMIS, Oxford Medical Information System
- STI, sexually transmitted infection
Genital Chlamydia trachomatis (CT) infection is widespread among young adults,1 and 10% of women aged <25 years who accepted screening in the primary care setting tested positive in pilots for a national screening programme in England.2,3 England is now in the process of rolling out an opportunistic National Chlamydia Screening Programme (NCSP)4 that will rely heavily on screening in primary care. The National Strategy for Sexual Health and HIV mandates the growth of sexually transmitted infection (STI) work in the primary care setting,5 whereas limited capacity in genitourinary medicine (GUM) services and the wider availability of laboratory tests has encouraged general practitioners (GPs) to provide more STI care.6 However, there is a dearth of information on recent trends in chlamydia testing, diagnoses and management in the primary care setting, against which the effect of the NCSP can be measured. Existing surveillance of STIs in the UK relies on “KC60” data collected from the national network of GUM (sexual health) clinics, and voluntary laboratory reports that are incomplete and subject to bias, while not distinguishing between different settings.7 High-quality data on the diagnosis and management of chlamydia in primary care are therefore required for service planning.
We used the General Practice Research Database (GPRD) as the basis for our study, to study current testing patterns, incidence, treatment and referral of CT in primary care, and how this has changed over time. The GPRD contains anonymised data on 4.7% (2.8 million in 2005) of the UK population, recorded in the primary care setting, which are updated within 3 months of recording. Practices using VISION administrative software are invited to contribute and paid for data. It is held by the Medicines and Healthcare Regulatory Agency, who undertake checks on the quality and completeness of data, which have been collected continuously since 1988. The GPRD is broadly demographically representative of the UK population, although there is a slight under-representation of inner London and Scotland. It has been used and validated for pharmacoepidemiological, epidemiological and public health uses as described elsewhere.8,9 Primary care data in the UK are now recorded almost exclusively on computer systems, and the emergence of several such large datasets based on different systems has been facilitated by routine collection of data by an overwhelming majority of GPs, and no longer only enthusiasts.
In this study, we aim to determine the extent of testing, diagnostic episodes and management of genital CT infection in UK primary care using the GPRD.
METHODS
Study population
All male and female patients in the GPRD aged 12–64 years between 1990 and 2004 were included in the analysis of CT testing and diagnosis.
Definitions of CT diagnostic episodes, tests, treatments and referrals
Diagnoses are recorded in the GPRD using “Read” or “Oxford Medical Information System (OXMIS)” codes that represent diagnoses, symptoms or tests, and are assigned to individuals during clinical consultation, on recording a test or on producing a prescription, along with prescription codes.
Diagnostic episodes of CT
The definition of a diagnostic episode of CT included all diagnoses, referrals and positive test results recorded in the database, which had Read and OXMIS terms denoting CT infection (supplementary table 1, available at http://sti.bmj.com/supplemental). All diagnosis episodes of chlamydia not explicitly specified as “genital” were assumed to be diagnoses of sexually acquired CT, after a review of the wider patient record in a sample of anonymised complete individual records confirmed that these almost exclusively denoted genital infection. These cases had age distributions similar to those explicitly designated as genital.
Tests for CT
A CT test was defined as an event with a Read or OXMIS term indicative of a CT test, whether positive, negative or ambiguous, as well as those indicative of a diagnosis of CT (supplementary table 1 available at http://sti.bmj.com/supplemental). We included diagnoses where no test code was recorded on the assumption that a diagnosis of CT would usually be given after receipt of a positive test result, although some diagnoses made elsewhere may have been self-reported by the patient.
Treatment for CT
Patients were assumed to have been treated for CT if they had a record of an appropriate drug prescribed 30 days on either side of the date on which a diagnosis code was recorded. Treatments before the date on which a diagnosis code was recorded were included to allow for presumptive treatment before a confirmed test result. Appropriate treatments included the current recommended treatments for CT infection: doxycycline, azithromycin, erythromycin and oxytetracycline.
Referrals for CT
In the GPRD, information on referrals can be stored in medical records as Read and OXMIS codes, in structured data areas of the database that record referral speciality and in the free text fields. All Read and OXMIS codes in the medical records indicating a referral for CT infection or a referral to a GUM clinic within 30 days of the diagnosis of CT were included. All referrals to a GUM specialist within 30 days of the diagnosis, which were recorded in the structured data area, were also included. In addition, for patients diagnosed as having CT but who did not have a prescription to treat CT, all non-specific referrals and all referrals to gynaecology within 30 days of the diagnosis were included.
A minority of patients with CT infection had neither treatment nor referral information recorded in coded or structured data. Anonymised free text of the subgroup of 158 such patients from 2003 was examined manually to determine their management.
Data analysis
The incidence of the outcomes of interest was calculated by dividing the number of episodes by the total person-time for the 12–64-year-old population of patients registered in the GPRD. Rates were expressed per 100 000 patient years (py). The frequency of events in patient records was plotted, which suggested that events occurring within 30 days of each other formed part of the same test, diagnosis, treatment or referral episode. As a result, all events occurring within 30 days of each other were grouped as a single episode. Patients were permitted to have repeat episodes in the analysis. To check the validity and sensitivity of the 30-day episode definition (which reflects GUM clinic practice), all analyses were repeated using a 60-day episode definition. Varying the time period used to define an episode was found to have negligible impact on incidence estimates. Positivity was estimated by dividing all positive test episodes by all test episodes.
The percentage of diagnoses of CT made in general practice versus those made in GUM clinics in the UK in 2004 was estimated from the population rate of treated CT infections in the GPRD and the rate of diagnoses of CT in GUM clinics estimated using data from statistical returns.10 It was assumed that patients treated in general practice were unlikely to have appeared as new diagnoses of CT in GUM clinics even if they had been referred there for partner notification.
All analyses used only “up-to-standard data”’, which are records scored as adequately consistent and complete according to protocols implemented by the holders of the database.11 The study was approved by the GPRD Scientific and Ethical Advisory Group.
RESULTS
In the GPRD, between 1990 and 2004, 70 717 CT tests were recorded, 95% of which were in women, and 9261 were diagnoses of CT, 88% of which were among women.
Figure 1 shows the incidence of CT testing in general practice by gender and age group. Until 1998, rates of testing were low, never rising above 100/100 000 py (ie, rates per 100 000 py as recorded for registered patients) in women, or above 10/100 000 py in males. Testing rates increased after 1998 in both men and women, although by 2004 overall testing rates were 19.4 times higher in women (1439/100 000 py) than in men (74/100 000 py). Among female patients, 5.5% (5509/100 000 py) of those aged 20–24 years, 3.7% (3719/100 000 py) of those aged 25–34 years, 3% (3082/100 000 py) of those aged 16–19 years and 2.3% (2289/100 000 py) of those aged 35–44 years were tested for chlamydia in 2004. Testing in men followed a broadly similar pattern across age groups. Supplimentary tables 2A and 2B give age-specific testing rates with CIs for men and women between 1990 and 2004 (available at http://sti.bmj.com/supplemental).
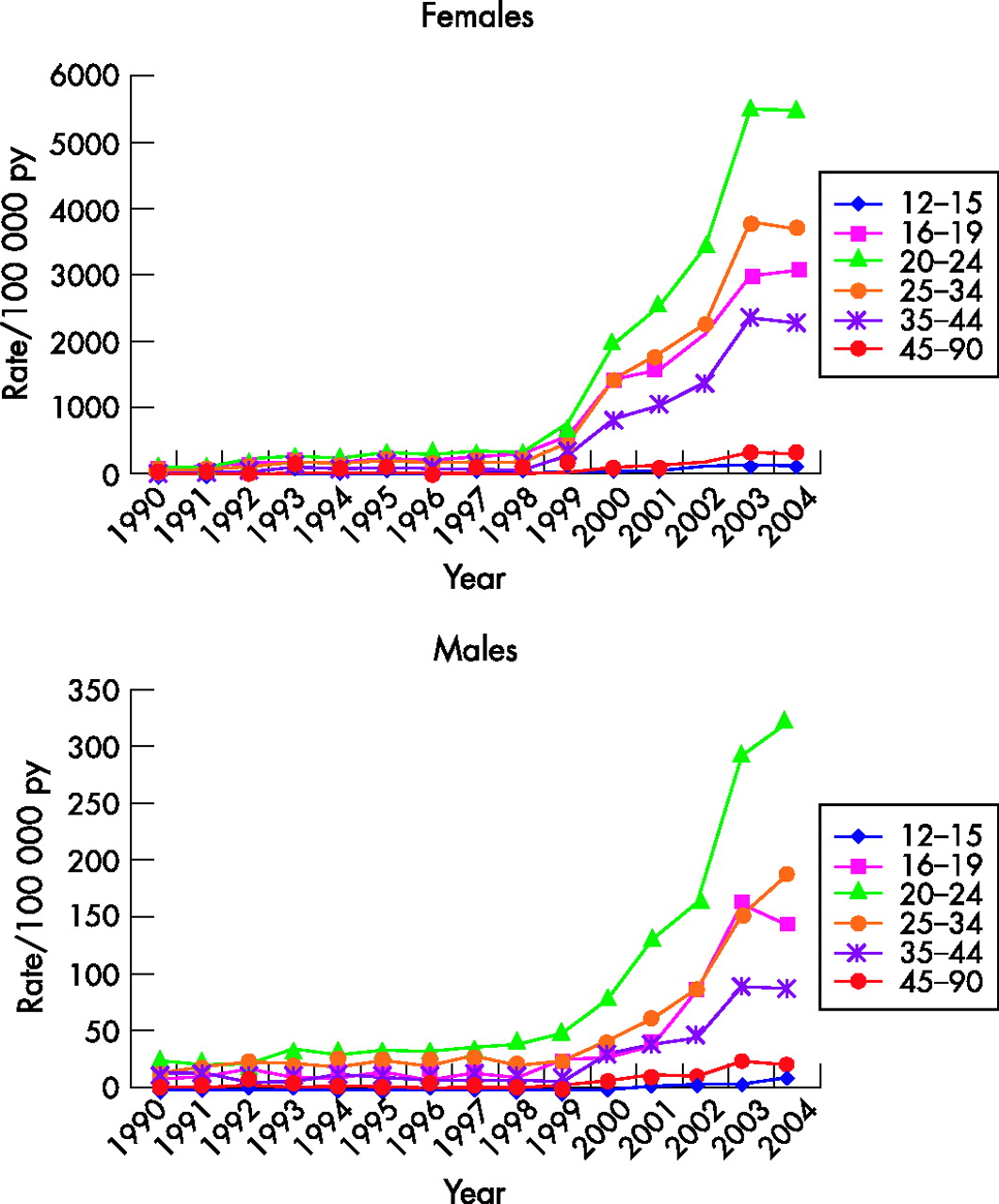
Rate of chlamydia testing in general practice by age group of patients, 1990–2004. Rates per 100 000 registered patient years (py).
Among women tested in 2004, the proportion of positive tests (positivity) ranged considerably by age, from approximately 15% in 12–19-year-olds to 2% in 35–44-year-olds. Positivity was much higher in men, ranging between 30% in those aged 20–24 years and 10% in those aged 35–44 years.
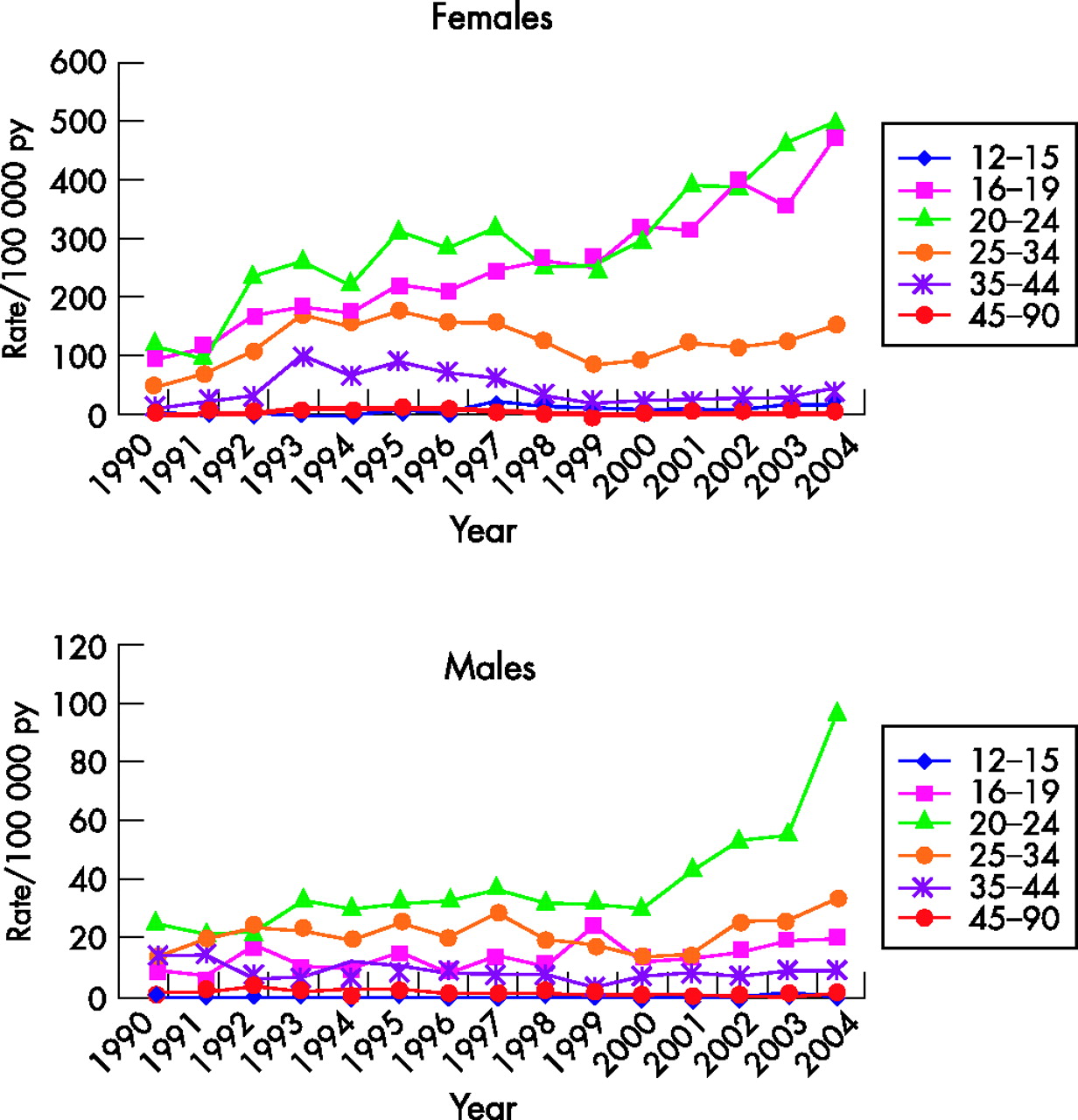
The incidence of diagnostic episodes of chlamydia increased steadily among women and men between 1990 and 2004, primarily because of increased diagnoses among women aged 16–24 years and among men aged 20–24 years (fig 2). In 2004, rates were five times higher in women than in men and were highest in women aged 16–19 and 20–24 years, with about 0.5% of the registered female population in these age groups being diagnosed (473 and 500/100 000 py, respectively). Rates of diagnosis were considerably lower in those aged ⩾25 years. In women, in 2004, rates were 153 and 47/100 000 py in those aged 25–34 and 35–44 years, respectively. Supplimentary tables 1A and 1B give age-specific diagnosis rates with CIs for men and women between 1990 and 2004 (available at http://sti.bmj.com/supplemental).

Diagnoses of chlamydia in general practice by age group, 1990–2004. Rates per 100 000 registered patient years (py).
The proportion of diagnosed patients treated by their GP has steadily increased since 1995 (fig 3). In 2004, 75.1% of women and 67.7% of men were treated in general practice. This corresponded with a sharp decline in patients being referred for further management over the same period (fig 3). Over the period, between 15% and 25% of patients had no record of either treatment or referral held in the structured areas of the GPRD. Examination of the anonymised free text records of the 158 patients who fell into this category in 2003 indicated that 62% had been referred to a GUM clinic for treatment. A further 6% were contacts of those with CT, 4% had a history of CT and 4% were negative for CT. No further information was available for the remaining 24% of these patients.

{kind=link}
{kind=link}
{kind=link}
Management of patients diagnosed with chlamydia in general practice, 1991–2004. Percentage of patients receiving appropriate treatment and/or referred for further management.
In 2004, the rate of new diagnoses of CT in women was 182.7/100 000 in GUM clinics2 and 60.9/100 000 (for treated infections) in general practice, suggesting that 25% of diagnoses of CT in women were made and treated in general practice. In men, the rate of new diagnoses of CT was 165.1/100 000 in GUM clinics,10 but only 8.9/100 000 (for treated infections) in general practice, suggesting that only 5.1% of diagnoses of CT in men were made and treated in general practice.
Of 8698 cases, 7957 had a single diagnostic episode recorded. The proportion of patients with chlamydia recorded as having a further diagnostic episode within 365 days was 6.58% (95% CI 6.02% to 7.19%) in women and 3.08% (95% CI 2.19% to 4.33%) in men. At 180 days, it was 4.64% (95% CI 4.18% to 5.15%) and 2.36% (95% CI 1.6% to 3.47%), respectively.
DISCUSSION
Our study shows that the sharp rise in diagnoses of genital chlamydial infection in GUM clinics in the UK between 1995 and 2004 has been mirrored in general practice, although the onset occurred 3–4 years later. Growth in the numbers of primary care patients being tested since 1999 is a major cause of the rise in diagnoses.12,13 However, it may be, in part, an artefact: electronic reporting of laboratory test results during this period, particularly since 2001, will have improved the ascertainment of chlamydia tests in the GPRD.
Despite increasing rates of diagnostic episodes of CT, there is still little evidence of a shift in the proportion of diagnoses being managed in general practice as might have been expected following publication of the National Strategy for Sexual Health and HIV.5 Overall, 25% of recorded chlamydia diagnostic episodes in women in 2004 were diagnosed and treated in general practice, a modest increase on the 23% estimated in 2000.14 As in 2000, only 5% of men were diagnosed and treated in general practice in 2004.
The targeting of chlamydia testing in the primary care setting remains suboptimal. Our findings on chlamydia testing practice confirm earlier findings13 that GPs disproportionately test women aged 25–44 years. The NCSP currently recommends screening in women aged <25 years.4 Although positivity among women was far higher in teenagers, they were less frequently tested than women aged 25–34 years, yet the rise in diagnoses of chlamydia in general practice was almost exclusively accounted for by diagnoses among women aged 16–24 years. Testing teenage women may be more difficult as they are more likely to refuse testing15,16 or less likely to consult their GP, although there is little evidence for this,17,18 and of course some will not yet be sexually active.
The proportion of repeat CT diagnostic episodes in the GPRD is comparable to the incidence recorded in primary care patients, in a study of reinfection among women diagnosed through the NCSP,19 despite the absence of a routine recall/retest policy in our population. These data further confirm the desirability of repeat testing of patients diagnosed as having genital chlamydial infection.
Key messages
-
Primary care datasets can provide important surveillance data, and show that 25% of all diagnoses of chlamydia in women were made in primary care in 2004, but only 5.1% of those in men.
-
A decreasing proportion of patients with chlamydia diagnosed in primary care are recorded as referred to genitourinary medicine, whereas a growing proportion are treated in primary care.
-
Chlamydia testing rates in primary care are highest in women aged 20–24 years (5.5% tested in 2004), followed by older women aged 25–34 years.
-
A total of 6.6% of women and 3.1% of men diagnosed as having chlamydia infection experience a repeat diagnostic episode within a year in the primary care setting.
Few men are being tested for or diagnosed as having chlamydia in primary care, and the high rate of positivity among those tested suggests that most were symptomatic, or were tested as part of the partner notification process. High rates of syndromic treatment of men with urethral discharge by GPs, shown in other work,14 may also have contributed to the overall lower rates of diagnosis of chlamydia compared with women, despite men presenting to primary care with STI-related symptoms.3
Our data, taken from a routine observational database, have a number of limitations. These include uncertainty about the degree to which full STI data are recorded in primary care. The comparison with data from GUM clinics assumes no double counting; however, patients may present to, and be treated in, both settings. We may have therefore overestimated diagnosed incidence of chlamydia, although from the point of view of service planning patients managed in both settings present a management workload in both. We could not estimate what proportion of chlamydia diagnostic episodes recorded in primary care is recorded in other settings (eg, A & E), nor the absolute incidence of such diagnostic episodes.
A growing proportion of all patients diagnosed with chlamydia in the primary care setting are treated by their GP, with about three-quarters of patients being issued appropriate prescriptions in recent years. This has coincided with a corresponding drop in the proportion of patients being referred for further management and hints at a growing confidence among GPs to manage patients with genital chlamydial infection. Such a development would be welcome since a significant proportion of patients referred to a GUM clinic may not attend and may therefore remain untreated, whereas practice-based management, when this includes partner notification and treatment, can be at least as effective as referral for further management by a GUM clinic.20 However, given the evidence that partner notification is generally not undertaken by primary care practitioners, and that referral to GUM clinics is undertaken informally,21 it will be important from a public health perspective to develop incentives and care pathways to support this important element of disease control.
In the context of the rollout of the NCSP and of the National Strategy for Sexual Health and HIV, data from the GPRD provide an important source of valuable baseline and monitoring data that should be used to contribute to the evaluation of the impact of the NCSP and the National Strategy for Sexual Health and HIV until purpose-built data collection systems are developed through the Connecting for Health programme of IT development for health services in England.22
REFERENCES
Supplementary materials
Files in this Data Supplement:
Footnotes
-
Published Online First 14 March 2007
-
Competing interests: None.
Linked Articles
- Editorial