Article Text

Abstract
Objectives Men who have sex with men (MSM) are disproportionately impacted by HIV. Criminalisation of homosexuality may impede access to HIV services. We evaluated the effect of the enforcement of laws criminalising homosexuality on access to services.
Methods Using data from a 2012 global online survey that was published in a prior paper, we conducted a secondary analysis evaluating differences in perceived accessibility to health services (ie, ‘how accessible are ____’ services) between MSM who responded ‘yes’/‘no’ to: ‘have you ever been arrested or convicted for being gay/MSM?’
Results Of the 4020 participants who completed the study and were included in the analysis, 8% reported ever being arrested or convicted under laws relevant to being MSM. Arrests and convictions were most common in sub-Saharan Africa (23.6% (58/246)), Eastern Europe/Central Asia (18.1% (123/680)), the Caribbean (15% (15/100)), Middle East/North Africa (13.2% (10/76)) and Latin America (9.7% (58/599)). Those arrested or convicted had significantly lower access to sexually transmitted infection treatment (adjusted OR (aOR)=0.81; 95% CI 0.67 to 0.97), condoms (aOR=0.77; 95% CI 0.61 to 0.99) and medical care (aOR=0.70; 95% CI 0.54 to 0.90), compared with other MSM, while accounting for clustering by country and adjusting for age, HIV status, education and country-level income.
Conclusions Arrests and convictions under laws relevant to being MSM have a strong negative association with access to HIV prevention and care services. Creating an enabling legal and policy environment, and increasing efforts to mitigate antihomosexuality stigma to ensure equitable access to HIV services are needed, along with decriminalisation of homosexuality, to effectively address the public health needs of this population.
- HIV
- PUBLIC HEALTH
- LAW
- HIV TESTING
- HOMOSEXUALITY
Statistics from Altmetric.com
Introduction
Men who have sex with men (MSM)—a term used to refer to men who engage in sexual behaviours with other men, regardless of self-identified sexual orientation—bear a disproportionate HIV burden across low-income and middle-income countries, and are undergoing a re-emergence of HIV in high-income countries.1 W1 Scale-up of evidence-based HIV services for MSM are needed to ameliorate this HIV pandemic.W1 W2 Nevertheless, in many places where these services exist, criminalisation of homosexuality still impedes access to these services.2 W3 Moreover, there is some evidence that countries criminalising homosexuality are less likely to allocate resources toward HIV programmes for MSM and more likely to have funding attrition for these programmes.3
Supplementary references
Determining whether a country criminalises homosexuality is challenging because of the wide range of punitive laws concerning same-sex sexual acts and sexual orientation that may be part of civil or penal codes, and may be enforced at varying levels.3 ,4 Currently, there are 78 countries worldwide that criminalise homosexuality, defined by the International Lesbian, Gay, Bisexual, Trans and Intersex Association (ILGA) as countries with legal provisions criminalising same-sex sexual acts between consenting adults.4
Criminalisation of homosexuality has been associated with reduced access to HIV services worldwide,2 as well as with increased odds of being HIV-infected among MSM, particularly in African and Caribbean countries.5 Where homosexuality is criminalised, studies have shown that MSM avoid accessing HIV prevention services due to fear of being persecuted, extorted or blackmailed.6 ,7 W4 Dramatic reductions in access to HIV services have also been observed immediately after laws criminalising homosexuality were put into place.8 W5 Additionally, enforcement of laws criminalising homosexuality can limit availability of services as they can force healthcare providers to suspend or deny services to avoid potential arrests and threats of violence.9
However, little is known about the prevalence of arrests or convictions related to being MSM. Furthermore, information on the magnitude of effect that arrests or convictions related to being MSM have on access to health services are sparse. As a first step to address these gaps, we sought to evaluate the association between arrests or convictions related to being MSM and access to services, using a global survey among MSM.
Methods
We conducted a secondary analysis of the Global Men’s Health and Rights Survey. This study's methodology has been previously described.W6 In brief, from April to August 2012, participants completed an anonymous 30 min online survey using Survey Monkey, in either English, Chinese, French, Georgian, Russian or Spanish. Perceived accessibility of different HIV services were measured in separate question items (ie, ‘how accessible are ____’ services) and were coded as ‘1’ for participants who reported ‘easy access’ to services, and ‘0’ for those who did not. We evaluated differences in accessibility to services between MSM who responded ‘yes’ and MSM who responded ‘no’ to: ‘have you ever been arrested or convicted for being gay/MSM?’, using the χ2 tests. We also evaluated the association between arrests and convictions and living in countries that criminalised homosexuality (as identified by the ILGA).W7 In multivariable analyses, we determined the association between arrests and convictions and accessibility of HIV services by fitting generalized estimating equation (GEE) logistic regression models with robust SEs, accounting for clustering by country while adjusting for participant age, HIV status and education, as well as country-level income (income of country of residence defined World Bank).W8 In sensitivity analyses, we stratified GEE models by region. The anonymous survey in the study met the Human Subjects exemption criteria—as determined by Research Triangle Institute International's Institutional Review Board—and did not require informed consent.
Results
Of the 6095 individuals who began the survey online, 4020 MSM had complete data and were included in this analysis. The self-reported prevalence of HIV was 18%. The mean age was 36.4 (SD=12.53), 86% self-identified their sexual orientation as gay, 32% reported being part of the ‘working class’ and 82% reported at least some postsecondary education.
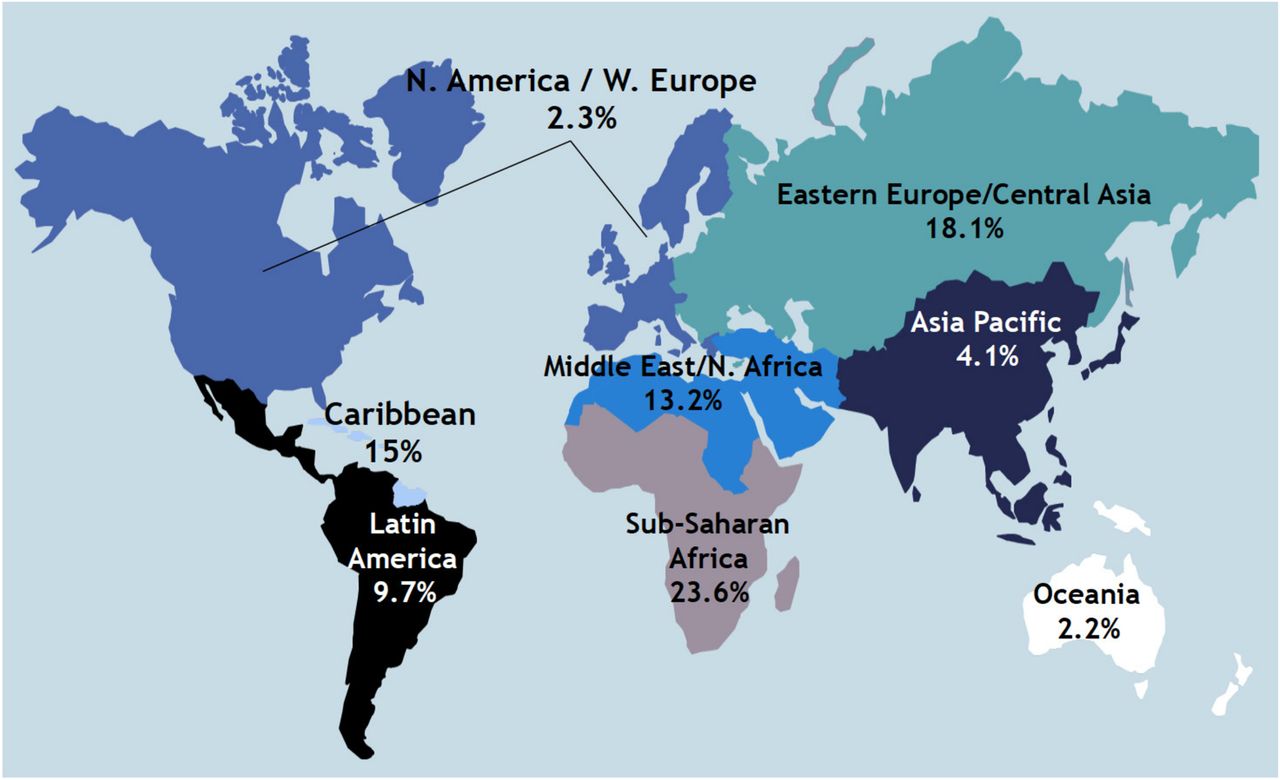
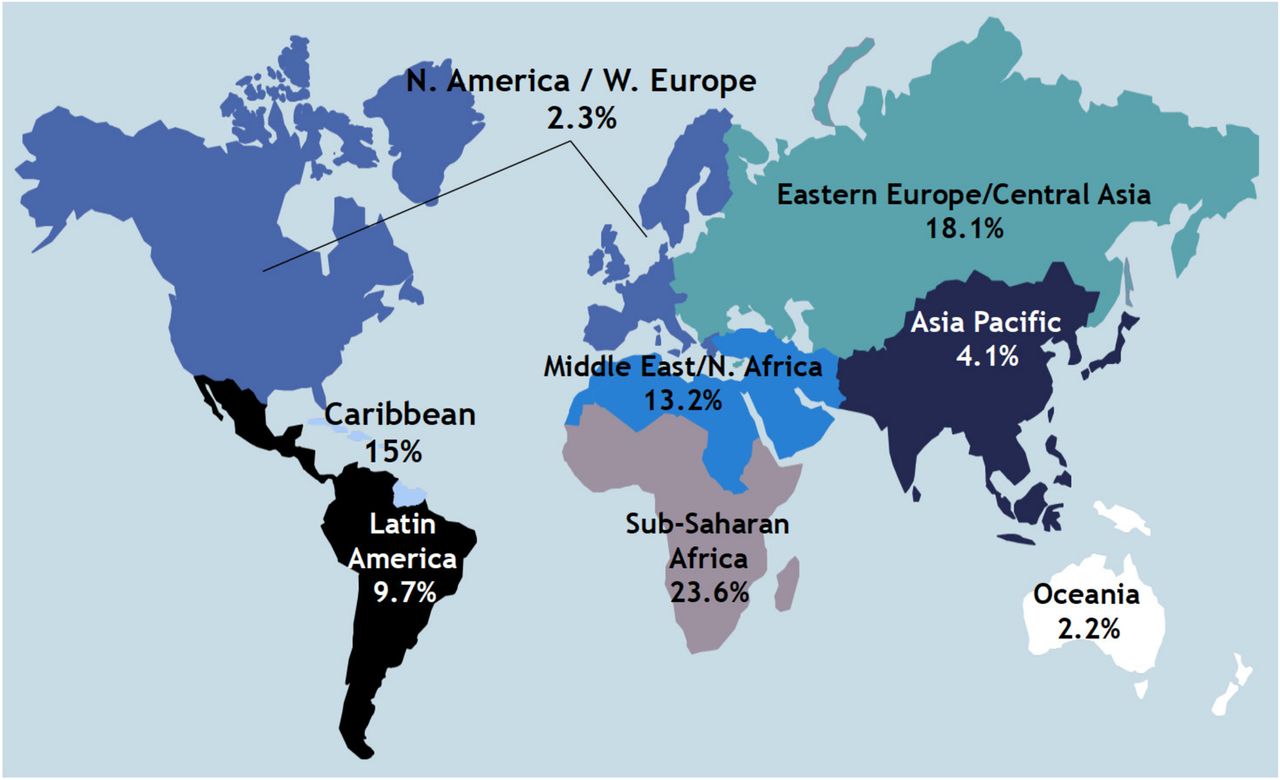
Overall, 8% of MSM reported ever being arrested or convicted under laws relevant to being MSM. Those who live in countries that criminalise homosexuality had significantly higher lifetime prevalence of arrests and convictions, compared with those who do not (12.2% vs 7.6%; p<0.001). By region, arrests or convictions were most prevalent in sub-Saharan Africa (23.6% (58/246)), Eastern Europe and Central Asia (18.1% (123/680)), the Middle East and North Africa (13.2% (10/76)), the Caribbean (15% (15/100)) and Latin America (9.7% (58/599)) (see figure 1). Arrests or convictions were less prevalent in Asia Pacific (4.1% (43/1048)), North America and Western Europe (2.3% (24/1038)) and Oceania (2.2% (5/233)). In bivariate analyses, MSM with arrests or convictions had significantly lower access to sexually transmitted infections (STIs) testing (59% vs 70%; p<0.001), STI treatment (41% vs 58%; p<0.001), condoms (64% vs 72%; p=0.002), lubricants (46% vs 54%; p=0.005), mental health services (27% vs 40%; p<0.001), medical care (41% vs 57%; p<0.001) and HIV testing (68% vs 74%; p=0.013). In addition, among HIV-positive MSM, arrests or convictions were significantly associated with lower access to HIV treatment (65% vs 80%; p=0.003).
{kind=link}
Lifetime prevalence of arrests or convictions for being gay or being a man who have sex with men, by region*. MSM, men who have sex with men.
In multivariable analyses, arrests or convictions were not significantly associated with differences in access to STI testing, lubricants, HIV testing and HIV treatment. Arrests or convictions were associated with significantly lower access to STI treatment (adjusted OR (aOR) 0.81; 95% CI 0.67 to 0.97), condoms (aOR 0.77; 95% CI 0.61 to 0.99) and medical care (aOR 0.70; 95% CI 0.54 to 0.90).
In sensitivity analyses, participants in Western Europe and North America with arrests or convictions relevant to being MSM had significantly reduced access to STI treatment (aOR 0.44; 95% CI 0.25 to 0.79) and medical care (aOR 0.41; 95% CI 0.23 to 0.74). Participants in Oceania with arrests or convictions had significantly reduced access to condoms (aOR 0.08; 95% CI 0.07 to 0.09) and medical care (aOR 0.07; 95% CI 0.03 to 0.18). Participants in Latin America with arrests or convictions had significantly reduced access to condoms (aOR 0.50; 95% CI 0.28 to 0.87) and borderline significant reduced access to medical care (aOR 0.53; 95% CI 0.26 to 1.05). Participants in sub-Saharan with arrests or convictions had significantly reduced access to condoms (aOR 0.48; 95% CI 0.25 to 0.94) and borderline significant reduced access to STI treatment (aOR 0.60; 95% CI 0.33 to 1.10).
Discussion
In this study, lifetime prevalence of arrests or convictions relevant to being MSM was high, especially in sub-Saharan Africa, the Caribbean, Eastern Europe/Central Asia and the Middle East/North Africa. As expected, higher prevalence of arrests or convictions was observed in countries that criminalise homosexuality. To our knowledge, this is the first global MSM survey to assess the prevalence of arrests or convictions from enforcement of laws criminalising homosexuality. There is a paucity of studies on the persecution of individuals relevant to being MSM by law-enforcement and government officials. One study among Southern African MSM from Malawi, Namibia and Botswana observed that 12.2% of MSM have experienced violence from government or police officials.10 More empirical data are needed to systematically describe the extent of enforcement of full spectrum of laws relevant to being MSM, including laws criminalising homosexuality and anal intercourse, as well as enforcement of other charges against MSM due to their sexual orientation.
Furthermore, our data suggests that enforcement of punitive laws for sex between men, as measured by arrests or convictions relevant to being MSM, has a strong negative association with access to HIV prevention and care services. While it is known that those incarcerated for other crimes are less likely to receive HIV and other services,W9–W11 this study adds to the literature because it specifically asked about arrests or convictions relevant to being MSM. Our findings document how those arrested or convicted under laws relevant to being MSM have significantly lower access to evidence-based interventions proven to reduce HIV acquisition and transmission.
This study has several limitations. It used a convenience sample and may be subject to selection bias. Participants from areas that criminalise homosexuality may also be less likely to participate or hear about this study. The cross-sectional study design also precludes any causal inferences. Moreover, there may be other unmeasured confounders that we did not account for that may be associated with both arrests or convictions, and access to services. Additionally, our measures are based on self-report, which may be subject to measurement bias. Furthermore, participants might not be informed of the underlying reason for their arrest or may be charged with other crimes unrelated to being MSM (eg, through vagrancy or nuisance laws), resulting in misclassification and under-reporting in our outcome. Unfortunately, we did not ask participants to specify what type of law related to being MSM they were arrested or convicted under. Hence, our study is unable to differentiate between the wide spectrum of laws that may have been applied to arrest or convict participants relevant to being MSM.
Despite these limitations, our study empirically documents the extent of arrests and convictions relevant to being MSM among a global sample. Furthermore, this data builds on prior ecological analyses that have documented how criminalisation of homosexuality undermines public health efforts and correlates with increased odds of HIV infection.2 W3 Decriminalising homosexuality may improve access to HIV services among MSM and enhance HIV prevention efforts. Creating an enabling legal and policy environment and increasing efforts to mitigate antihomosexuality stigma to ensure equitable access to HIV services are needed, along with decriminalisation, to effectively address the public health needs of this population.
Footnotes
Handling editor Jackie A Cassell
Collaborators Pato Hebert; Jack Beck; Patrick Wilson.
Contributors All authors contributed to and approved the final draft of the manuscript. G-MS conceptualised the analysis, wrote the manuscript and conducted the data analysis and interpretation. KM, SA, TD and GA were responsible for the design of the study, assisted in the writing of the manuscript and interpretation of data.
Funding The Bill and Melinda Gates Foundation funded this study.
Competing interests None declared.
Ethics approval Research Triangle Institute International's IRB provided the IRB exemption.
Provenance and peer review Not commissioned; externally peer reviewed.