Article Text

Abstract
Background Repeat infection with gonorrhoea may contribute significantly to infection persistence and health service workload. The authors investigated whether repeat infection is associated with particular subgroups who may benefit from tailored interventions.
Methods Data on gonorrhoea diagnoses between 2004 and 2008 were obtained from Sheffield sexually transmitted infection clinic. Kaplan–Meier survival curves were used to estimate the percentage of patients with repeat diagnoses within a year, and a Cox proportional hazard model was used to investigate associated risk factors.
Results Of 1650 patients diagnosed with gonorrhoea, 7.7% (95% CI 6.5% to 9.1%) had a repeat diagnosis within 1 year. Men who have sex with men under 30, teenage heterosexuals, black Caribbeans, people living in deprived areas and those diagnosed in 2004 were most likely to re-present. Of those patients (53%) providing additional behavioural data, repeat diagnosis was more common in those reporting prior history of gonorrhoea, any previous sexually transmitted infection diagnoses, two or more partners in the past 3 months and a high-risk partner in the past year. In an adjusted analysis, repeat diagnosis was independently associated with being a young man who has sex with men, living in a deprived area, a history of gonorrhoea and being diagnosed in 2004 but was most strongly associated with non-completion of behavioural data forms.
Conclusions Groups most at risk of repeat infection with gonorrhoea are highly predictable but are disinclined to provide detailed information on their sexual behaviour. Care pathways including targeted and intensive one-to-one risk reduction counselling, effective partner notification and offers of re-testing could deliver considerable public health benefit.
- Gonorrhoea
- surveillance
- sexual behaviour
- epidemiology (general)
- Chlamydia trachomatis
- syphilis
- antimicrobial resistance
- chlamydia infection
Statistics from Altmetric.com
- Gonorrhoea
- surveillance
- sexual behaviour
- epidemiology (general)
- Chlamydia trachomatis
- syphilis
- antimicrobial resistance
- chlamydia infection
Introduction
Gonorrhoea is the second most common bacterial sexually transmitted infection (STI) in England.1 In Western industrialised countries, gonorrhoea disproportionately affects black ethnic minorities and men who have sex with men (MSM)2 and controlling the spread of infection is probably best achieved through intervention measures targeting these populations.3 With the global emergence of gonococcal resistance to antimicrobials, primary prevention could become increasingly important for infection control.4 ,5
Repeat infection with gonorrhoea may account for a significant proportion of gonorrhoea diagnoses.6 ,7 Individuals who repeatedly acquire gonococcal infection play a key role in onward transmission and infection persistence,8 represent a failure of prevention activities within the treating clinic setting and may add significantly to clinic workload. Determining the characteristics of patients most likely to re-attend with gonorrhoea presents an opportunity for developing targeted, relevant and efficient approaches to reducing infection incidence.9 There is little recent published literature quantifying repeat gonococcal infection and very few studies outside the USA.10 To date, studies have suggested gonococcal reinfection is associated with a range of factors including a history of STIs, younger age and non-white race but associations between reinfection and risky sexual behaviour have been inconsistent.10
Survival analysis is a convenient tool for investigating risk of repeat infection.11 In this paper, we used this approach on an enhanced surveillance data set from the STI clinic in Sheffield, UK, to estimate risk and important socio-demographic and behavioural determinants of gonorrhoea reinfection, which could be used to tailor intensive interventions in the UK setting.
Methods
Population studied
Sheffield is a city in central England with a relatively stable population of over 500 000; 150 000 are aged 15–30 years, including approximately 50 000 students during term time.12 It comprises 339 geographic units known as lower-level super output areas.12
Gonorrhoea diagnosis
One STI clinic (also known as a genitourinary medicine clinic) serves this population and diagnoses about 300 gonorrhoea infections per year. Patients were routinely tested for gonorrhoea at all genital and extra-genital sites as indicated by sexual history.13 The testing protocol for gonorrhoea was altered to routinely include screening by strand displacement assay as well as culture in February 2005, following demonstration of good concordance in results by both methods.13 It is likely that most diagnosed infections in Sheffield residents are referred to the STI clinic as part of an established collaborative local sexual health network. About 10% of gonorrhoea cases seen in Sheffield STI clinic were diagnosed in, and referred from, other clinical settings, especially through the National Chlamydia Screening Programme.
Data collection
The enhanced surveillance scheme collected clinical, demographic and behavioural data relating to patients attending the STI clinic in Sheffield (the Royal Hallamshire Hospital). Patient clinical and behavioural information was recorded on proformas and in the patient's clinical record during the clinical consultation, whereas socio-demographic data were recorded at patient registration. Patients self-assigned their ethnic group. Coded data relating to patient attendances for gonorrhoea between 2004 and 2008 were extracted from electronic patient records held in the clinic database. Data collection and extraction methods have been described in greater detail previously.14 ,15
Data analysis
Diagnoses of uncomplicated gonorrhoea (genital, anorectal and pharyngeal) and complicated gonorrhoea between 2004 and 2008 were included in the analysis. Patients were grouped into lower-level super output areas of residence which were then mapped to the 2007 English index of multiple deprivation (IMD).16 The IMD is a deprivation score at the small area level (combining seven distinct domains of deprivation).16 In this study, we used the IMD score's rank among all areas in England and categorised these into four percentile groups to ensure similar group sizes (1 (least deprived): <60th percentile; 2: 60th to <85th percentile; 3: 85th to <95th percentile; 4 (most deprived) ≥95th percentile).
Coded personal identifiers were used to link patient attendances. Repeat diagnosis with gonorrhoea was defined as having a second attendance for gonorrhoea at least 42 days after the first episode. Attendances for gonorrhoea within 42 days of the first attendance were excluded as they were assumed to relate to the same episode of infection. The 42-day episode length reflected the typical clinical practice in managing bacterial STIs, and previous sensitivity analysis (unpublished) indicated that shortening or lengthening this period by several weeks had minimal impact on diagnosis rates. Patients whose first attendance in the data set was within 42 days before the end of the available follow-up period were also excluded. Behavioural data linked to the first patient attendance were analysed.
The percentage of patients who became re-infected with gonorrhoea within 1 year was estimated by the Kaplan–Meier method. Patients became at risk from 42 days after the time of first attendance with gonorrhoea and were censored at the end of the study period (31 December 2008). Cox regression was used to estimate HRs for groups defined by the following variables: gender, age group, sexual orientation, ethnic group, year of first recorded attendance for gonorrhoea, IMD rank, residence in Sheffield, history of gonorrhoea or any STI, number of sexual partners in the past 3 months, sex abroad in the past 3 months, having a high-risk sex partner in the previous year (eg, known HIV positive, homo/bisexual man, from a high prevalence area, injecting drug or sex worker), being a sex worker and history of injecting drugs. Data on number of new sexual partners were quite incomplete among those completing the behavioural proforma and were excluded from regression modelling to allow a greater number of patients to be included in the analysis. Log-rank tests were used to test for any difference between the groups.
Multivariable Cox regression was then used to estimate independent associations between the variables and repeat diagnosis. Sex abroad in the past 3 months was not entered into the multivariable model because it was far from statistical significance and was a small group. Heterosexual men and women were combined because they displayed a similar relationship with risk. All other variables were retained. Likelihood ratio methods were used to test significance. For those variables included in the final model, we investigated the possibility of effect modification by either completion of the behavioural proforma, being an MSM, or year. A global test of the proportion hazards assumption was performed.
Missing values were a particular concern for the behavioural variables. For estimating survival curves, the percentage of patients with a repeat diagnosis within 1 year and HRs between groups, the analysis excluded patients with missing values. For multivariable Cox regression, patients who did not complete the behavioural proforma were included by making ‘non-completion’ a risk factor and adding categories of ‘non-completion of behavioural proforma’ to all behavioural variables. Perfect co-linearity of these new categories resulted in just one parameter for ‘non-completion’ being fitted. The disadvantage of this method is that adjustment for behavioural risk factors was incomplete which could have resulted in bias due to residual confounding. The advantages of this approach are that all adjusted HRs were based on the same model and the same observations, and estimates included more data than the usual complete case analysis. Including those who did not complete the forms made little difference to the HRs for the other behavioural risk factors.
Results
Study population
During the study period, there were 1889 episodes of gonorrhoea in 1650 patients who could be followed up for at least 42 days. Where recorded, 41% of patients were women, 44% heterosexual men and 15% MSM (table 1). Three-quarters of patients were younger than 30 years, two-thirds were white and a quarter lived in the most deprived areas of Sheffield (IMD group 4) (table 1). Additional behavioural information on the proforma was available for just over half (880/1650; 53%) of patients.
Gonorrhoea repeat diagnosis by patient characteristics
Repeat diagnosis
Eleven per cent (183/1650) of patients presented with at least one repeat diagnosis, which comprised 9% with one repeat diagnosis and 1.6% with two repeat diagnoses (maximum five repeat diagnoses per patient).
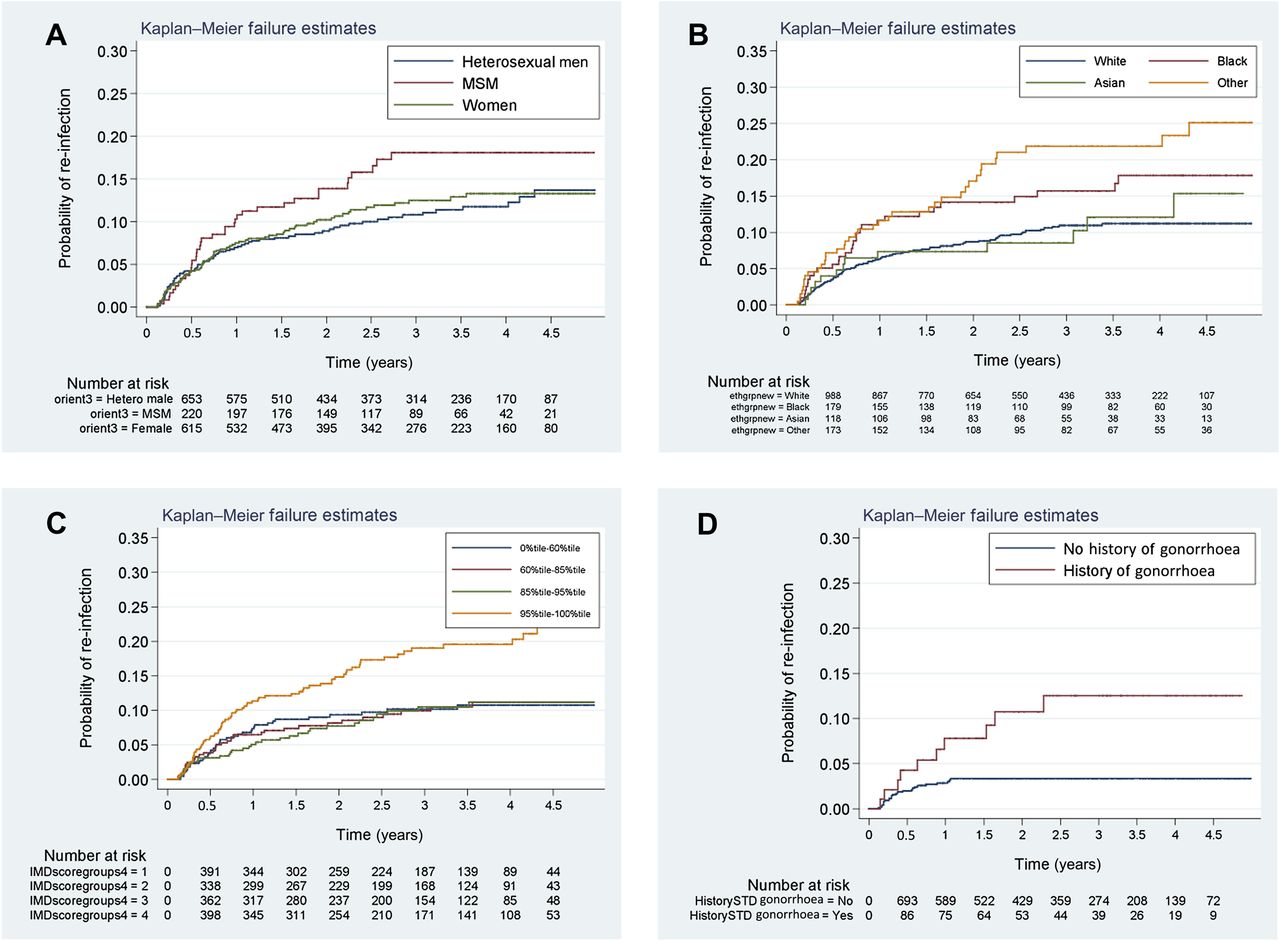
From the Kaplan–Meier analysis, the overall rate of re-attendance with gonorrhoea was estimated at 7.7% (95% CIs 6.5% to 9.1%) within 1 year. The groups of patients most likely to be re-infected with gonorrhoea within 1 year were those diagnosed in 2004 (11.3%), MSM under 30 years (15.1%), teenage heterosexual men (10.5%) and women (9.6%), those of black Caribbean (12.0%) or mixed (11.6%) ethnic origin, and those living in the most deprived areas of Sheffield (11.3%) (table 1A, figure 1A–C). Patients with behavioural data recorded on the proforma were much less likely to re-attend with gonorrhoea than those with missing behavioural data (3.4% and 12.1%, respectively; table 1A). Nevertheless, within the subset of patients with behavioural data, repeat diagnosis with gonorrhoea was more common in those reporting a history of gonorrhoea, a history of any previous STI diagnosis, two or more partners in the past 3 months and having a high-risk sex partner in the past year (table 1B, figure 1D).
{kind=link}
Repeat infection with gonorrhoea by patient characteristics: Kaplan–Meier estimate. (A) Sexual orientation, (B) ethnic group, (C) deprivation group and (D) history of gonorrhoea.
In univariable regression modelling, repeat diagnosis was significantly associated with being diagnosed in 2004, being of black Caribbean or mixed ethnic origin, living in the most deprived areas of Sheffield and having no behavioural data recorded on the proforma (table 1A). Among those with behavioural data, reporting a history of gonorrhoea, a history of any previous STI diagnosis, two or more partners in the past 3 months and a high-risk sex partner in the past year were all significantly associated with repeat diagnosis (table 1B). There was evidence of non-proportional hazards over time between those that did and did not complete the behavioural proforma with the HR increasing over time (p=0.01).
In the multivariable model, being diagnosed in 2004, being an MSM (especially a teenage MSM), living in the most deprived areas of Sheffield, having a history of gonorrhoea and having no behavioural data recorded on the proforma were independently associated with a greater risk of repeat diagnosis (table 2). Having two or more partners in the past 3 months was weakly associated (table 2). However, there was evidence of non-proportional hazards (p=0.01), with the risk of repeat diagnosis continuing to increase over time in those without behavioural data.
Gonorrhoea repeat diagnosis by patient characteristics
Discussion
In this UK-based study, the overall risk of repeat infection with gonorrhoea within 1 year was estimated as 8% and was strongly associated with particular patient characteristics, being highest in teenage heterosexuals, young MSM, black ethnic minorities and in those living in the most deprived areas of the city. Only just over half of patients provided additional behavioural data, but of those that did, repeat infection was strongly associated with markers of higher risk sexual behaviour, especially higher rates of partner change and a history of gonorrhoea. However, those at greatest risk of repeat infection were disinclined to provide any information on their sexual behaviour.
There are a number of limitations to our study. Our sample was taken from patients attending one clinic in England between 2004 and 2008 and is clearly not representative of all those diagnosed with gonorrhoea in the UK. We used repeat diagnosis as a proxy measure of repeat infection, so repeat infection rates will have been underestimated as some patients will have become re-infected but remained undiagnosed and since repeat diagnoses at other clinics could not be included. However, probably the most important limitation concerns the bias caused by missing behavioural data. In our study, the estimated risks among those with and without behavioural risk factors were lower than they should be because the risk of repeat diagnosis was considerably lower among those completing behavioural forms. It is likely that those with higher risk sexual behaviours are less willing to disclose this information.17 The risk of repeat diagnosis in those reporting a history of gonorrhoea and in those reporting two or more partners in the previous 3 months was only about 8% and 4%, respectively. If not for the missing data in our study, these subgroups would most likely have had the highest risk of repeat infection.
An earlier study of repeat infection with gonorrhoea in heterosexuals in Sheffield during 1976–1979 found a considerably higher repeat infection risk of 18% per year in the context of much higher incidence, but otherwise, the defining characteristics of those with repeat infection were remarkably similar.9 These findings are also consistent with a systematic review of US-based studies10 and suggest that potential gonorrhoea ‘repeaters’ are highly predictable and could be the focus of enhanced interventions. Because we were able to collect detailed and comprehensive longitudinal data on a large urban clinic population, we believe that our study strengthens the evidence for the relationship between repeat infection and sexual risk-taking behaviour, previously found to be inconsistent,10 and also puts it into a UK context.
Rapid partner turnover, concurrent partnerships and short gaps between partnerships are likely to drive incidence among population groups experiencing disproportionately high rates of gonococcal infection,8 ,18–21 and to some extent, high repeat infection rates will reflect assortative sexual mixing patterns among these groups. Concurrent partnerships and barriers to condom use, such as associating condom use with lack of trust and pleasure, may contribute to repeated STI risk exposure among young black Caribbeans in particular.22 Despite the limitations of the behavioural information in our study, in the adjusted model associations between gonorrhoea repeat diagnosis and demographic characteristics such as ethnic group were less important than behavioural indicators such as having a history of gonorrhoea and reporting two or more recent partners. Living in the most deprived areas of Sheffield also remained independently associated with increased risk of repeat diagnosis. These findings are consistent with a picture of densely connected sexual networks (ie, people with multiple links to other people who are themselves closely linked) in defined geographical areas, which favours the persistence of gonorrhoea.23 ,24
Some subsequent presentations with gonorrhoea could have resulted from treatment failure. Cephalosporins, usually cefixime, were routinely used in accordance recommended treatment guidelines at that time; however, reduced sensitivity may have led to suboptimal treatment of infection in some individuals.25 ,26 Treatment compliance may also be a problem, particularly in teenagers.27
The significant reduction in repeat infection rates in this clinic since the 1970s, and between 2004 and 2005, coincided with a decrease in new diagnoses which may have reduced the likelihood of repeat exposures within dense sexual networks. It suggests an accumulative impact from a range of sustained control measures. Historically, an intensive approach to partner notification has been adopted in Sheffield.28 Provider referral has been particularly successful in reaching casual partners whom patients are least likely to inform themselves29 but who may play a disproportionate role in onward transmission.30 In Sheffield, community control of gonorrhoea has also benefited from centralised management of partner notification by health advisers in the STI clinic, with established referral pathways from other services. The establishment of a collaborative local sexual health network may have facilitated a more systematic approach to STI control. Initiatives included extending gonorrhoea testing beyond the STI clinic setting and implementing the National Institute for Health and Clinical Excellence guidance31 to offer one-to-one structured risk reduction discussions to all patients at risk of an STI.
Our data strongly suggest that intensive interventions in the GUM clinic setting tailored to the needs of those at high risk of repeat infection with gonorrhoea could potentially reduce infection rates and deliver considerable public health benefit. There are clear behavioural drivers for repeat infection and groups at highest risk are highly predictable. Care pathways for those at high risk may be improved by intensive one-to-one risk reduction counselling by a dedicated team of health advisers working to agreed protocols and standards32 effective partner notification including regular audit of outcomes and regular offers of re-testing.33 Further research is needed to strengthen the evidence that such intensive interventions could deliver a sustained reduction in onward transmission and repeat infection in other UK settings.
Key messages
-
Teenage heterosexuals, young MSM and those of black ethnic origin were at highest risk of repeat infection with gonorrhoea.
-
Repeat infection may have been fuelled by densely connected sexual networks, often in deprived areas of the city.
-
Those at higher risk of repeat infection were less inclined to provide detailed information on their sexual behaviour.
-
Intensive risk reduction counselling, partner notification and offers of re-testing targeting those at high risk could bring considerable public health benefit.
Acknowledgments
Mike Catchpole was involved in setting up the sentinel surveillance scheme. We are grateful to Jonathan Spate for downloading data from the clinic database and André Charlett, Parnam Seyan, Chinelo Obi and Chris Lane at HPA Health Protection Services Colindale for help with data collation and analysis.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.