Article Text

Abstract
Context Abdominal aortic calcification (AAC) is a common finding in patients with atherosclerosis.
Objective The aim of this study was to demonstrate the incremental value of AAC in predicting long term cardiovascular (CV) outcome by conducting a meta-analysis of observational studies.
Data sources MEDLINE and Cochrane databases.
Study selection Longitudinal studies with at least 2 years of follow-up, reporting the influence of AAC on CV outcome of general population patients.
Data extraction Four separate end points—coronary events, cerebrovascular events, all CV events and CV related death—were tested for their relationship with AAC at baseline, using weighted random effects meta-analysis. Heterogeneity was calculated using Q and I2 statistic tests. Publication bias was assessed by funnel plot symmetry and trim and fill methods. The importance of calcium quantification was also explored (sensitivity analysis).
Results 10 studies were included. An increased relative risk (RR) was found for all end points: for coronary events (five studies, n=11250) 1.81 (95% CI 1.54 to 2.14); for cerebrovascular events (four studies, n=9736) 1.37 (1.22 to 3.54); for all CV events (four studies, n=4960) 1.64 (1.24 to 2.17); and for CV death (three studies, n=4986) 1.72 (1.03 to 2.86). Analysis of studies presenting results in categories (no/minimal, moderate and severe calcification) revealed a stepwise increase in the RR for all end points. Significant heterogeneity was found in the included studies. Sources of heterogeneity were identified in the publication date, duration of follow-up, and mean age and gender differences in the included patient cohorts.
Conclusion Existing data suggest that AAC is a strong predictor of CV related events or death in the general population. The predictive impact is greater in more calcified aortas. The generalisability of the meta-analysis is limited by heterogeneity in the coronary events, all CV events and CV death end points.
Statistics from Altmetric.com
Introduction
The role of vascular calcification in cardiovascular (CV) risk estimation has been investigated in recent years. Atherosclerosis is a systemic condition known to affect different vascular beds in varying degrees. Symptoms are frequently episodic in nature, involving a single organ or system, and may remain absent for long periods. Arterial wall calcification, a common byproduct of arterial plaques, may serve as an objective marker of asymptomatic atherosclerotic disease and as a tool for CV risk assessment.1–3
In contrast with coronary artery calcification (CAC), which is well established as a CV prognostic tool,2–6 abdominal aortic calcification (AAC) has been scarcely investigated as a diagnostic marker of atherosclerosis or as a tool for CV risk assessment. It is generally accepted that plaque formation in the abdominal aorta is present during the early stages of the atherosclerotic process. Progression of disease eventually results in plaque calcifications, which can easily be identified and quantified using simple lateral lumbar radiography.7 A strong correlation between AAC and atherosclerosis in other vascular beds was recognised in post mortem studies decades ago.8 However, few studies have attempted to correlate calcification of the abdominal aorta with CV events or CV related death.
We conducted a systematic review and meta-analysis with the objective of clarifying the role of AAC (measured through calcium scoring) as an independent predictor of CV events in the general population. Furthermore, we assessed how the prognostic capacity is influenced by the amount of calcification present.
Methods
Literature search strategy
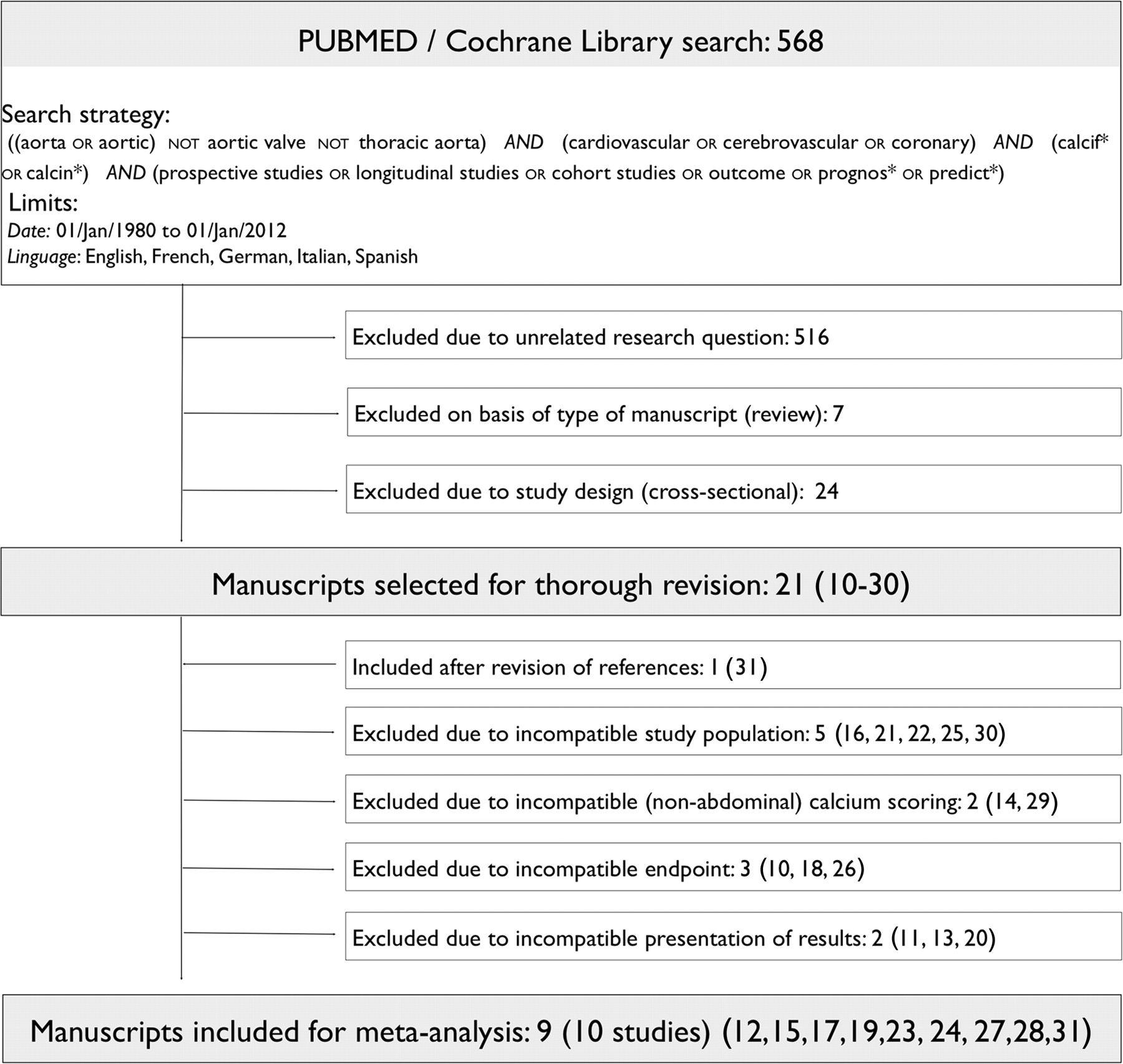
Two reviewers (FBG and MTV) independently performed the search according to the MOOSE criteria.9 The objective was to find all longitudinal studies on general population cohorts, correlating AAC to subsequent CV events and presenting the results adjusted for traditional CV risk factors, hence demonstrating the independent influence of AAC. A systematic internet based search was performed using the PUBMED and Cochrane Library databases. The following search strategy was used: ((aorta OR aortic) NOT aortic valve NOT thoracic aorta) AND (cardiovascular OR cerebrovascular OR coronary) AND (calcif* OR calcin*) AND (prospective studies OR longitudinal studies OR cohort studies OR outcome OR prognos* OR predict*). The search was limited to original articles in English, German, French, Spanish or Italian, published from January 1980 to December 2011. A manual search of references from the selected publications was also performed (figure 1).
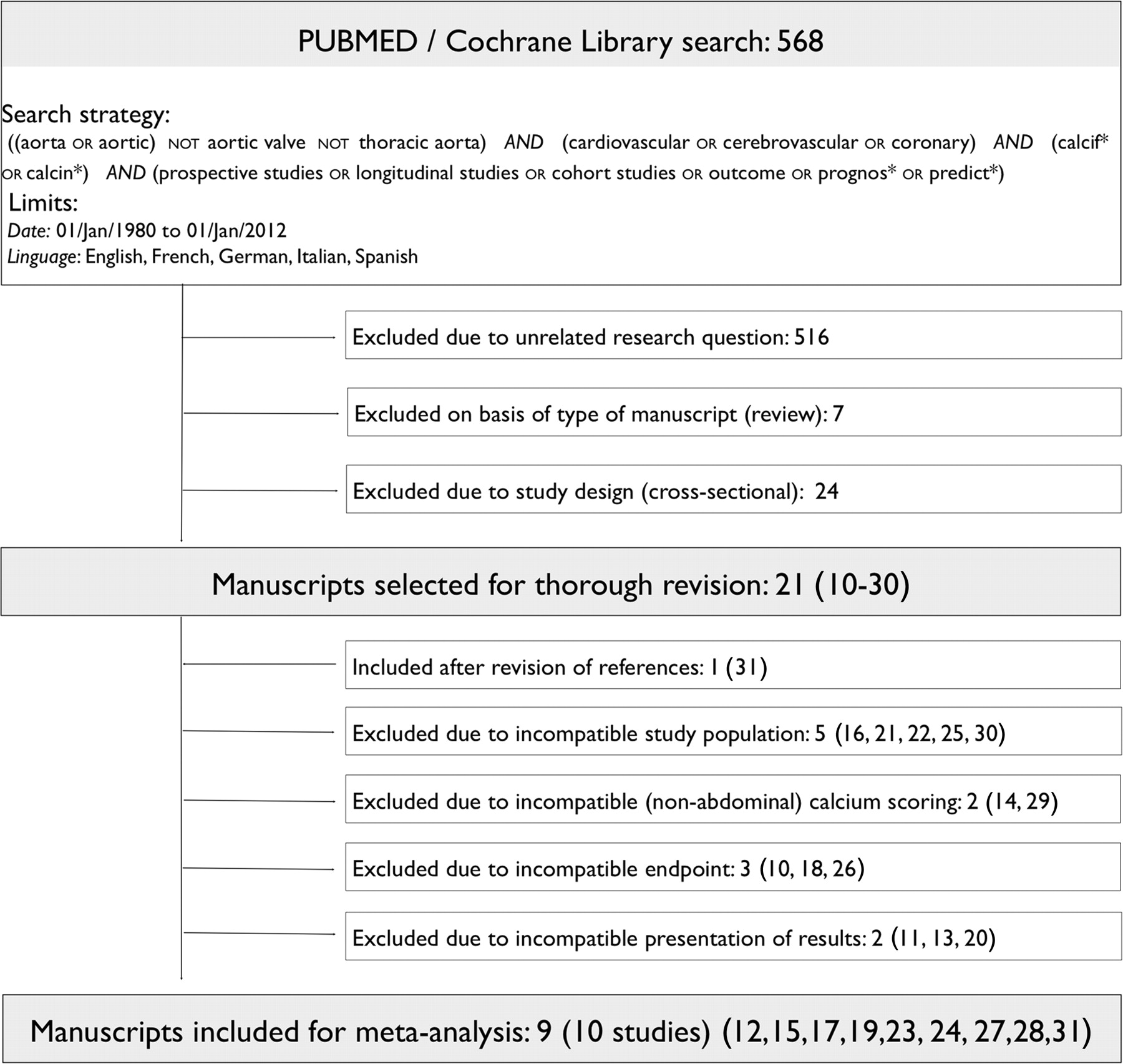
Search strategy flowchart.
Study selection
The initial search retrieved 568 manuscripts of potential interest. Of these, 516 were excluded after examining the title and abstract due to unrelated research questions. Seven manuscripts were excluded because they were review articles and another 24 due to cross sectional design. Twenty-one articles were left for thorough revision.10–30 A search in the references of these resulted in one more manuscript being added for review.31
Twelve publications were subsequently excluded from the overall analysis: five studies included only patients in high CV risk groups: end stage renal disease (Okuno et al, Verbeke et al, Hanada et al and Ohya et al) and peripheral arterial disease (Parr et al).16 21 22 25 30 Walsh et al reported heart failure as end point26; Alexandersen et al reported on the influence of hormonal therapy on AAC progression10; and Kushiya et al included all thrombotic events (such as pulmonary embolism and arteriovenous fistula problems) in a combined end point.18 Two studies (DeLoach et al and Danielsen et al) correlated thoracic aortic calcification with CV prognosis.14 29 The studies by Blacher et al and Nielsen et al presented HR as per SD increase, making the results not comparable with the remaining.11 20 The study by Davila et al was excluded due to methodological incompatibility with the remaining studies (CT based scoring method, selected cut-off at the 75th percentile and no multivariate analysis).13 Contact was made with the authors of the manuscript by Bolland et al in order to obtain data not originally presented.12 It resulted in the inclusion of this manuscript in the overall analysis. A summary of the included studies is presented in table 1.
Overview of studies included in the meta-analysis
Patient duplication
Four manuscripts published results on the same two cohorts of patients: Wilson et al and Levitzky et al used the Framingham Heart Study population,19 27 and Hollander et al and van der Meer et al used the Rotterdam Study cohort.17 31 In the first case there was an overlap of two out of three study end points (both studies reported on coronary and all CV events). After careful consideration we opted to include all end points of the first published study (Wilson et al) and include only the cerebrovascular outcome for the subsequent study, which was not reported in the former. The rationale was to preserve all available data but avoid duplication within each outcome analysis. We should point out that the HR for both studies was very similar (as expected since they derive from the same cohort) and if we opted for the inclusion of results from the latter study the pooled analysis would remain practically unchanged. Regarding duplication in the Rotterdam Study, the study end points were completely independent from one another. Since a separate pooling was made for each end point there is no influence on the quality of the results by including both studies.
Calcification scoring
The methods used for scoring were AAC-24 and AAC-8 using lumbar roentgenograms.17 19 21 23 24 27 28 These scoring methods are discussed in detail in the correspondent publications. Briefly, the AAC-24 system scores aortic calcification as 0 (no calcification), 1 (a third or less of the aortic wall), 2 (one third to two thirds) or 3 (more than two thirds). Scores range from 0 to 6 for each vertebral level (L1–L4), to a total of up to 24. The AAC-8 scale is the sum of the total length of calcification for each of the anterior and posterior aortic walls in front of vertebrae L1–L4 (table 2).
Calcium scoring methods of the included studies
End points
Four different end points were independently analysed: coronary events, cerebrovascular events, all CV events and CV related death. Several studies presented multiple end points and were included in more than one pooled analysis. No overall analysis including all studies was attempted, for two main reasons: (1) the comparison between different types of CV outcomes would result in unacceptable heterogeneity; and (2) significant overlap of patients within multiple end point studies would be present. Five studies presented quantitative results in function of the presence or absence of AAC12 15 23 28 31 while three presented results in tertiles17 24 27 and one in categories.19 In the latter studies the lowest groups corresponded to the absence or near absence of aortic calcification (table 2). Pooling of the two highest ranges allowed homogeneity with the other studies (ie, comparison between patients with aortic calcification and those without) at the cost of reducing the prognostic impact of a higher score.
Subgroup analyses/sensitivity
A separate analysis including only studies that presented results in tertiles/categories according to the amount of calcium present in the aorta (none/minimal, moderate or severe) was used to address the impact of calcium load on prognosis.17 24 27 31 The thresholds used for these studies were equivalent and are detailed in table 2. The influence of age and gender on results was analysed by pooling the RR from studies including only elderly women.12 23 24
Statistical methods
We interpreted HRs as RR. Meta-analyses were performed using fixed and random effects modelling. Results are presented in Forest plot illustrations and the overall effect (Z) was measured. We assessed the results for heterogeneity by calculating the Q statistic, which we compared with a χ2 distribution and the I2 index.32 The Q statistic test indicates the statistical significance of the homogeneity hypothesis and the I2 index measures the extent of heterogeneity. We considered heterogeneity significant if p<0.10 (two sided). Publication bias was assessed by visually examining funnel plot symmetry and was also quantified using the Egger regression test, considered significant if p<0.10 (two sided).33 The implications of publication bias were assessed using the Duval and Tweedie trim and fill method.34 Statistical analysis was performed using MIX software (BiostatXL, Utrecht, The Netherlands).35
Results
Nine manuscripts published from 1986 to 2010 were included in the meta-analysis, contemplating 10 independent studies (table 1). All studies were assumed to be representative of the general western European and North American populations (although the exact ethnic proportions were not reported). In five studies, patients were part of large cohort studies (EPOZ, Framingham and Rotterdam cohorts).17 19 27 28 31 The remaining five study populations were derived from bone densitometry/osteoporosis screening studies in the general population, four of which included only women and one included only men.12 15 23 24 Mean follow-up time of the included studies varied from 2.8 to 32 years.
Meta-analysis
Four independent weighed meta-analyses were performed, one for each end point (figure 2). Using random effects modelling, the pooled RRs were: for coronary events 1.81 (95% CI 1.54 to 2.14); for cerebrovascular events 1.37 (1.22 to 3.54); for all CV events 1.64 (1.24 to 2.17); and for CV death 1.72 (1.03 to 2.86). Overall effect was significant for all end points (p<0.0001). Comparison between fixed and random effects modelling revealed only minor differences in the pooled RR but random effects modelling resulted in larger CIs. Significant heterogeneity was observed for coronary events (I2=59%), for all CV events (I2=58%) and for CV death (I2=80%). No heterogeneity was observed for the cerebrovascular end point.

Forest plot representation of weighed meta-analysis of cardiovascular end points.
Subgroup analyses/sensitivity
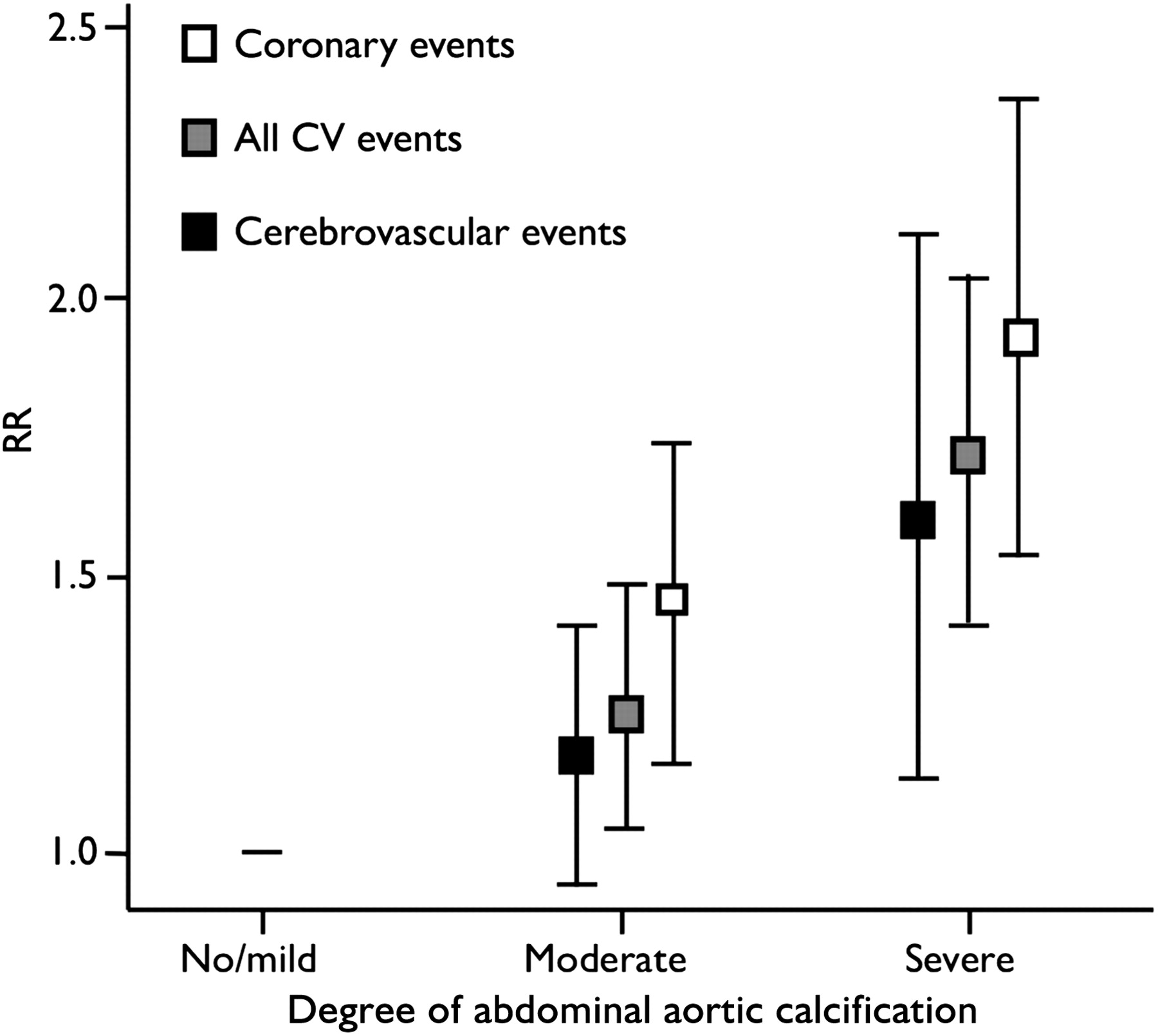
For studies that presented AAC quantification in tertiles, a significant stepwise increase in risk was observed, as demonstrated in figure 3. The RRs for the middle tertile (moderate calcification) and higher tertile (severe calcification) were: for coronary events 1.43 (1.17–1.77) and 1.92 (1.54–2.38); for cerebrovascular events 1.17 (0.95–1.43) and 1.56 (1.13–2.16); and for all CV events 1.26 (1.06–1.50) and 1.71 (1.42–2.05), respectively. No pooling was possible for the CV death end point, as only one study reported results in tertiles.
A pooled analysis for studies including only elderly women was not possible because the number of studies was small (three studies) with disparity between end points: comparable end points were present in only two studies.12 23 24 However, simple observation of an increase in RR in each individual study in comparison with the overall results of each pooling suggests a general tendency towards a lower RR for AAC in elderly women.
Publication bias analysis
Funnel plot asymmetry was apparent for all end points. The Egger regression test resulted in a non-significant p value for all end points. Funnel plots including imputed studies and adjustment of RR and 95% CI for publication bias are reported in figure 4. As shown, the adjusted RR did not differ significantly from the unadjusted results obtained using random effects modelling.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Publication bias (trim and fill method). Included studies are represented as filled circles and imputed studies are represented as white circles. The black line represents the log relative risk (Ln RR) before adjustment for publication bias while the broken line represents the adjusted Ln RR.
Discussion
Prevention of CV disease presents significant challenges, as the clinical course is frequently silent until a major event occurs. Well accepted CV risk models based on traditional CV risk factors, such as the Framingham Risk Score,36 lack the desired accuracy, and additional risk predictors with incremental prognostic value are anticipated. Direct indicators of atherosclerosis, such as vascular calcification, may significantly improve the accuracy of CV risk prediction in asymptomatic patients.
Calcification of the coronary arteries has been extensively investigated as a prognostic biomarker: patients with a high CAC score are known to be at higher risk for future CV events compared with those with low scores. In this regard, the predictive value of CAC scoring is greater than that of the Framingham Risk Score alone in the general population, supporting its potential as a complementary screening and risk assessment tool.2 3 There are standardised and validated techniques for CAC scoring, measuring area, mass or volume, using either electron beam CT or, more recently, multidetector CT, all with fairly equivalent results.4–6
Inversely, the abdominal aorta has been scarcely investigated for CV risk stratification. However, this vascular site is particularly prone to the development of atherosclerotic lesions. In susceptible subjects, atheroma probably develops earlier and more significantly in this vascular territory than in any other, despite a common lack of related symptoms.8 37 The presence of plaque calcification (indirect evidence of advanced atherosclerosis) at this location may prove to be at least as valuable as coronary artery calcium scoring in CV risk stratification.
Interestingly, there are several publications correlating abdominal aortic calcification with traditional risk factors for atherosclerosis, biomarkers and bone demineralisation (see references in the supplement, available online only). From these, one can safely conclude that AAC is a common finding in patients with other traditional CV risk factors, such as hypercholesterolaemia, hypertension, obesity or smoking habits. The unanswered questions were: (1) can the presence of aortic calcification per se contribute to CV risk prediction in the general population; and (2) is more extensive aortic calcification associated with a greater CV risk.
It is clear from the results of this meta-analysis that the presence of AAC uniformly increases the risk of subsequent CV events or CV related death in the general population. Importantly, this increment in CV risk is still evident after adjustment for traditional CV risk factors. This observation provides robust evidence supporting a role for AAC as a biomarker for CV risk modelling. As previously shown with CAC, integration of AAC in risk models for asymptomatic subjects may have the potential for risk reclassification and therefore influence primary prevention strategies.2 3 A more accurate risk estimation may justify aggressive lifestyle modification and drug therapy for patients with a high risk profile. The role of AAC in secondary prevention remains less clear, however, as studies analysing these patients are generally smaller and have several methodological discrepancies, and these patients should generally be on intensive therapeutic regiments anyway.16 21 22 25 30
Two interesting observations could be drawn from comparing the pooled RR from each study end point: first, the RR of the cerebrovascular end point is lower that the remaining, suggesting that, while AAC is still a valid predictor of stroke, it puts patients at a proportionally lower risk for that specific type of event. This is further corroborated by the absence of statistical significance in the RR for the middle tertile of this end point, as shown in figure 3. Although division by tertiles reduces the number of events ‘per tertile’ and consequently increases the interval size, this absence of statistical significance most likely reflects the diversified aetiology of stroke. It is suggested that the prognostic influence of AAC for stroke is only relevant with higher degrees of calcification.
Also, the impact of AAC in CV risk appears to be gradually decreasing with increasing age, which is evident for studies that recruited only elderly patients.23 24 This inverse relationship between the prognostic capacity of AAC and age is intuitive: a young patient with aortic calcification (and therefore atherosclerosis) is at a much higher CV risk than a young patient without atherosclerotic disease. Conversely, elderly patients are more likely to have both calcified vessels and CV events, making AAC a less sensitive marker. However, the number of studies that included only elderly subjects was too small and biased by gender to draw any definitive conclusions in this regard.
Subgroup analysis on studies that reported calcification stratified into tertiles revealed that more extensive calcification was associated with a higher RR for CV events. The observed stepwise increase in RR was uniform across three different end points (coronary events, cerebrovascular events and all CV events). This observation suggests an additional quantitative dimension to AAC as a biomarker for CV risk. As previously mentioned, only the highest tertile of calcification significantly increased the RR of cerebrovascular events. Therefore, our findings can only support the prognostic value for highly calcified vessels in regard to this end point.
With the exception of studies included in the cerebrovascular events end point, significant heterogeneity was identified among studies. Despite a uniform demonstration of independent prognostic significance in AAC across all included studies, some inconsistency in the gradation of risk was observed. This can be attributed to differences in patient characteristics (particularly mean age and gender proportions although all subjects derived from healthy general population cohorts) and in follow-up duration. Also, one of the studies included28 showed significant discrepancy, pending towards a higher RR: this is likely due to the publication date (1986) when primary CV prevention was not yet generalised. Also, two very large and relevant studies, both derived from the Framingham cohort, had much longer durations of follow-up than the remaining studies (22 and 32 years). We opted not to exclude studies based on duration of follow-up in order to conserve all the data available, however this contributes to the heterogeneity in the results.
Some limitations must be considered. First, the sample size of studies included in each pooled analysis was small, despite large numbers of patients. Also, all studies were based in cohorts with predominantly healthy western European or North American subjects. Therefore, the significance of AAC for other ethnic groups or higher CV risk populations cannot be deduced from these results.
Visual analysis of funnel plots suggested the presence of publication bias, which was not demonstrated by Egger regression testing (with the exception of the cerebrovascular end point), an observation most likely due to the sample size of the included studies. The non-randomised nature of studies also increases the likelihood of bias. However, the proximity of the unadjusted RR using random effects modelling and the adjusted RR using the trim and fill method suggest no reason to doubt the validity of the core findings, despite a possible variation in the true RR effect size.
In conclusion, this systematic review and meta-analysis suggests that the presence of AAC is a relevant and independent predictor of future CV events, and higher degrees of calcification correspond to a higher RR. This supports a role for AAC as a clinically important biomarker that could improve CV risk prediction in asymptomatic patients. Reclassification in CV risk category as a result of AAC scoring may improve patient care, directing more aggressive primary prevention strategies at patients with higher risk profiles.
References
Footnotes
Funding FMVBG and SEH are supported by an unrestricted research grant from the Dutch Organisation of ‘Lijf & Leven’. MTV is supported by an unrestricted research grant from The Netherlands Heart Foundation (No 2009B020).
Competing interests None.
Provenance and peer review Not commissioned; not externally peer reviewed.