Article Text

Abstract
Context HCM is commonly associated with AF. Current guidelines for AF management omit detailed advice for HCM because of a lack of clinical prediction tools that estimate the risk of developing AF and an absence of adequately powered treatment studies.
Objective To critically review current literature on atrial fibrillation (AF) and thromboembolism in hypertrophic cardiomyopathy (HCM) and meta-analyse prevalence and incidence.
Data Sources PubMed and Web of Science.
Study Selection Studies investigating AF and stroke in HCM as primary or secondary endpoint.
Data Extraction Two investigators independently reviewed and extracted data from the identified articles. A random effect meta-regression model and I2 statistics were used for analysis.
Results A population of 7381 patients (33 studies) revealed overall AF prevalence of 22.45% (95% CI 20.13% to 24.77%), I2=78.9% (p<0.001). Overall prevalence of thromboembolism in HCM patients with AF was 27.09% (95% CI 20.94% to 33.25%), I2=61.4% ( p<0.01). Overall AF incidence was 3.08% per 100 patients per year (95% CI 2.63% to 3.54%, I2=86.5%, p<0.001) and incidence of thromboembolism in HCM patients with AF was 3.75% per 100 patients per year (95% CI 2.88% to 4.61%), I2=37.9% (p=0.1). Left atrial (LA) dimension and age were common predictors for AF and thromboembolism. Meta-analysis revealed an LA diameter of 38.03 mm (95% CI 34.62% to 41.44%) in sinus rhythm and 45.37 mm (95% CI 41.64% to 49.04%) in AF. There were no randomised controlled trials of therapy; anticoagulation was associated with lower stroke incidence but data on other interventions were limited and contradictory.
Conclusions AF is common in HCM and associated with high thromboembolic risk. LA dimension and age are independently associated with AF but the literature is insufficient to create robust clinical tools to predict AF or thromboembolism. Most data suggest that AF patients should be anticoagulated.
Statistics from Altmetric.com
Introduction
Hypertrophic cardiomyopathy (HCM), defined as left ventricular hypertrophy in the absence of abnormal loading conditions, occurs in 1 in every 500 adults. In most individuals, it is inherited as an autosomal dominant trait caused by mutations in cardiac sarcomere protein genes and is associated with an increased risk of sudden cardiac death and long-term morbidity from progressive ventricular dysfunction.1 ,2 Many cohort studies have shown that atrial fibrillation (AF) is a common complication of the disease and that it is associated with adverse clinical outcomes. However, current guidelines for the management of AF lack detailed advice on the management of AF in patients with HCM because of an absence of adequately powered studies on pharmacological treatment strategies in this setting. The primary aim of this study was to perform a systematic review and meta-analysis of the published literature on AF and thromboembolism in patients with HCM to determine the feasibility of developing a disease specific algorithm for the management of AF.
Methods
The methodology and presentation of the review are based on the recommendations of the PRISMA statement.3
Study selection
Two independent reviewers (OPG and AA) performed the literature search and checked the eligibility of each study. Disagreement between the two reviewing authors was resolved by consensus with a third author (PME).
PubMed and Web of Science electronic databases were searched using the terms ‘hypertrophic cardiomyopathy’, ‘atrial fibrillation’, ‘stroke’ and ‘thromboembolism’ in title and abstract. Reviews, case reports and abstracts were excluded from the analysis. The reference lists of reviews, letters and editorials were scrutinised for additional papers. All searches were limited to ‘human’ and ‘English’. The last search was performed on 1 September 2012. Studies were eligible if they investigated AF and/or stroke or thromboembolism as primary or secondary outcome in a prospective or retrospective study.
The following variables were extracted from each study: number of patients, sex, mean age, predictors of AF and thromboembolism, prevalence of AF and thromboembolism, definitions of AF and stroke/thromboembolism and length of follow-up (see online supplementary tables S1 and S2). Where available, the effect of antiarrhythmics, anticoagulants and AF ablation on morbidity and mortality was investigated.
Meta-analysis
Studies reporting prevalence data for AF and thromboembolism were included in the meta-analysis. Not all studies provided SE of the prevalence and so SE was calculated using the prevalence data and sample size in each study with the following formula:
 Assuming that the estimated values for prevalence follow a normal distribution we calculated 95% CI for population prevalence. Incidence rate for each study was calculated using number of new cases and median follow-up time provided by the study. SE of incidence rate was calculated assuming Poisson distribution of number of new cases. A random effect meta-regression model4 was then used to combine the prevalence data and to obtain the pooled (overall) prevalence and incidence for AF and thromboembolism separately. The overall prevalence was the weighted average of the prevalence across different studies, where weights were calculated using measures of precision (inverse of the variance of the prevalence). Intra- and inter-study variances were used in the calculation of precision. The intra-study variance was the variance of the prevalence obtained as above (square of SE) for each study. The inter-study variance, a parameter of the random effects meta-regression model, was estimated using method of moments.4 The inter-study variance was used to adjust for the heterogeneity in prevalence between studies. Heterogeneity between studies was further assessed using the I2 statistic, which represents the proportion of total variability in the prevalence data attributable to the heterogeneity between the studies. The overall estimate, obtained using this method, takes more weight from the study with higher precision associated with smaller SE. A random effect meta-analysis was conducted to obtain an overall cut-off value of LA diameter for both sinus rhythm (SR) and AF, using average median values of LA diameter from individual studies in patients with SR and AF. All these computations were conducted using Stata V.11.
Assuming that the estimated values for prevalence follow a normal distribution we calculated 95% CI for population prevalence. Incidence rate for each study was calculated using number of new cases and median follow-up time provided by the study. SE of incidence rate was calculated assuming Poisson distribution of number of new cases. A random effect meta-regression model4 was then used to combine the prevalence data and to obtain the pooled (overall) prevalence and incidence for AF and thromboembolism separately. The overall prevalence was the weighted average of the prevalence across different studies, where weights were calculated using measures of precision (inverse of the variance of the prevalence). Intra- and inter-study variances were used in the calculation of precision. The intra-study variance was the variance of the prevalence obtained as above (square of SE) for each study. The inter-study variance, a parameter of the random effects meta-regression model, was estimated using method of moments.4 The inter-study variance was used to adjust for the heterogeneity in prevalence between studies. Heterogeneity between studies was further assessed using the I2 statistic, which represents the proportion of total variability in the prevalence data attributable to the heterogeneity between the studies. The overall estimate, obtained using this method, takes more weight from the study with higher precision associated with smaller SE. A random effect meta-analysis was conducted to obtain an overall cut-off value of LA diameter for both sinus rhythm (SR) and AF, using average median values of LA diameter from individual studies in patients with SR and AF. All these computations were conducted using Stata V.11.
Results
A total of 256 articles in PubMed and 79 in Web of Science fulfilled the search criteria. After adjustment for duplicates, 262 unique records remained. Following exclusions (figure 1), 33 records reporting data on 7381 patients remained (see online supplementary table S1).5––37 All studies were observational or used retrospective data collection.

Study selection process.
Incidence and prevalence of thromboembolism and AF
The definitions of AF varied between studies, but most included patients with paroxysmal and chronic AF. Six studies investigated only paroxysmal AF. Four studies defined paroxysmal AF by duration or symptoms (see online supplementary table S1).
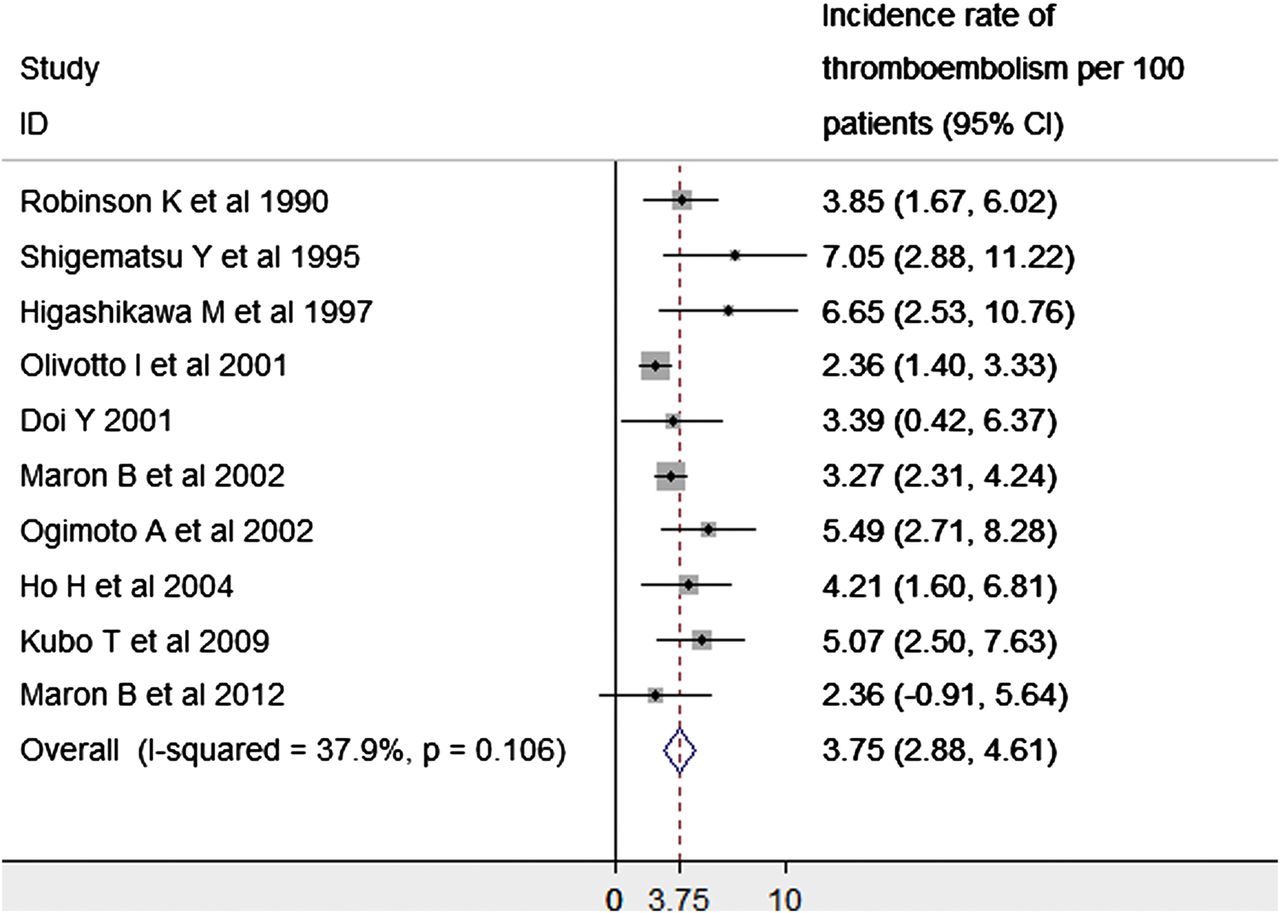
The pooled overall prevalence of paroxysmal and permanent AF was 22.45% (95% CI 20.13% to 24.77%, I2=78.9%, p<0.001; figure 2). The pooled overall prevalence of all thromboembolic complications in patients with HCM and AF was 27.09% (95% CI 20.94% to 33.25%, I2=61.4%, p<0.01; figure 3). The pooled overall incidence of paroxysmal and permanent AF was 3.08% (95% CI 2.63% to 3.54%, I2=86.5%, p<0.001; figure 4). The reported overall incidence of AF in two studies was 2% and 2.6%, respectively.15 ,22 The pooled overall incidence of all thromboembolic complications in patients with HCM and AF was 3.75% (95% CI 2.88% to 4.61%, I2=37.9%, p=0.1; figure 5).

Prevalence of atrial fibrillation (AF). The forest plot from random effect meta-analysis shows study specific prevalence and the pooled (overall) prevalence of AF. The heterogeneity between the study was estimated as I2=78.9% (p<0.001). The overall prevalence is 22.45%.
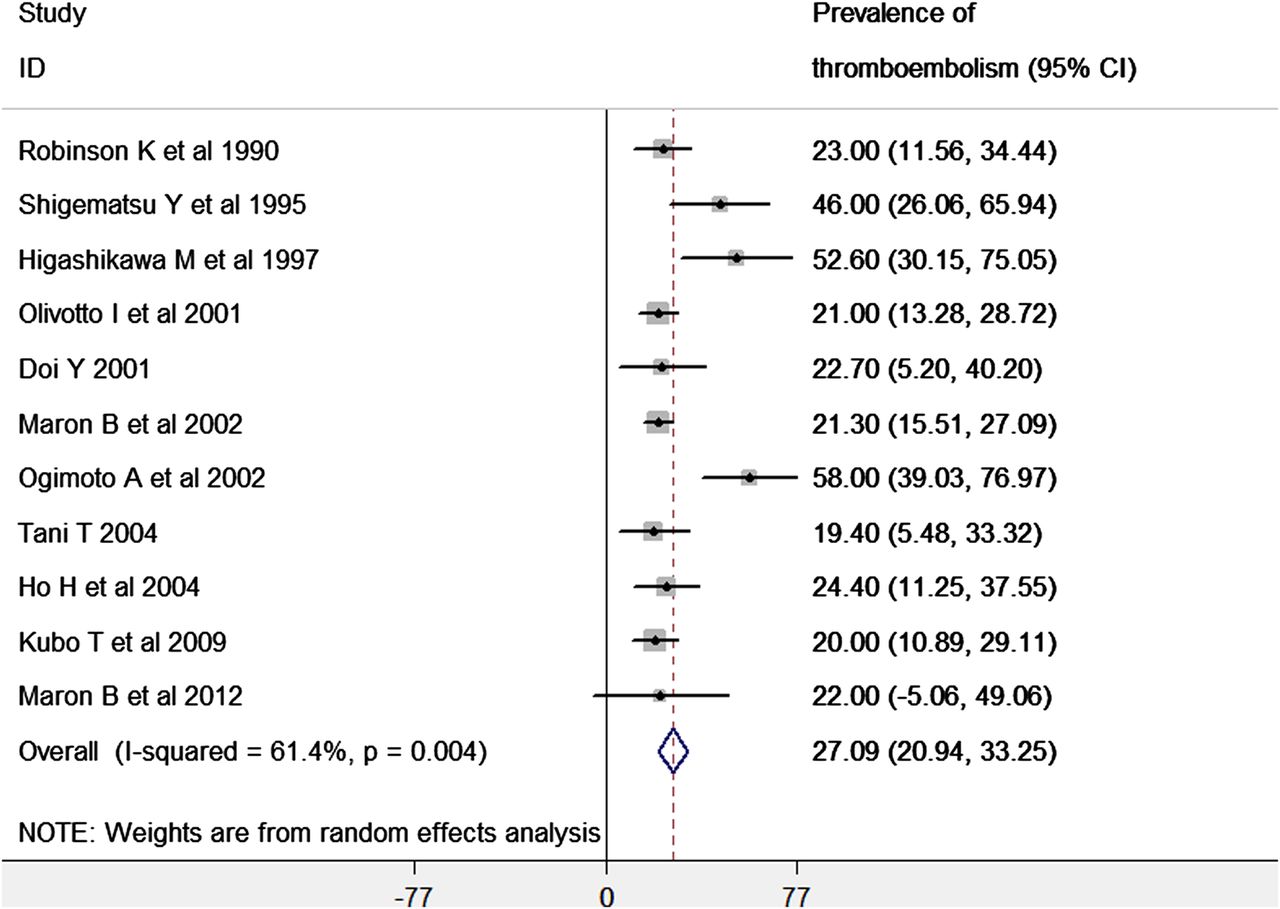
Prevalence of thromboembolism. The forest plot from random effect meta-analysis shows study specific prevalence and the pooled (overall) prevalence of thromboembolism in patients with hypertrophic cardiomyopathy and atrial fibrillation. The heterogeneity between the study was estimated as I2=61.4% (p<0.01). The overall prevalence is 27.09%.
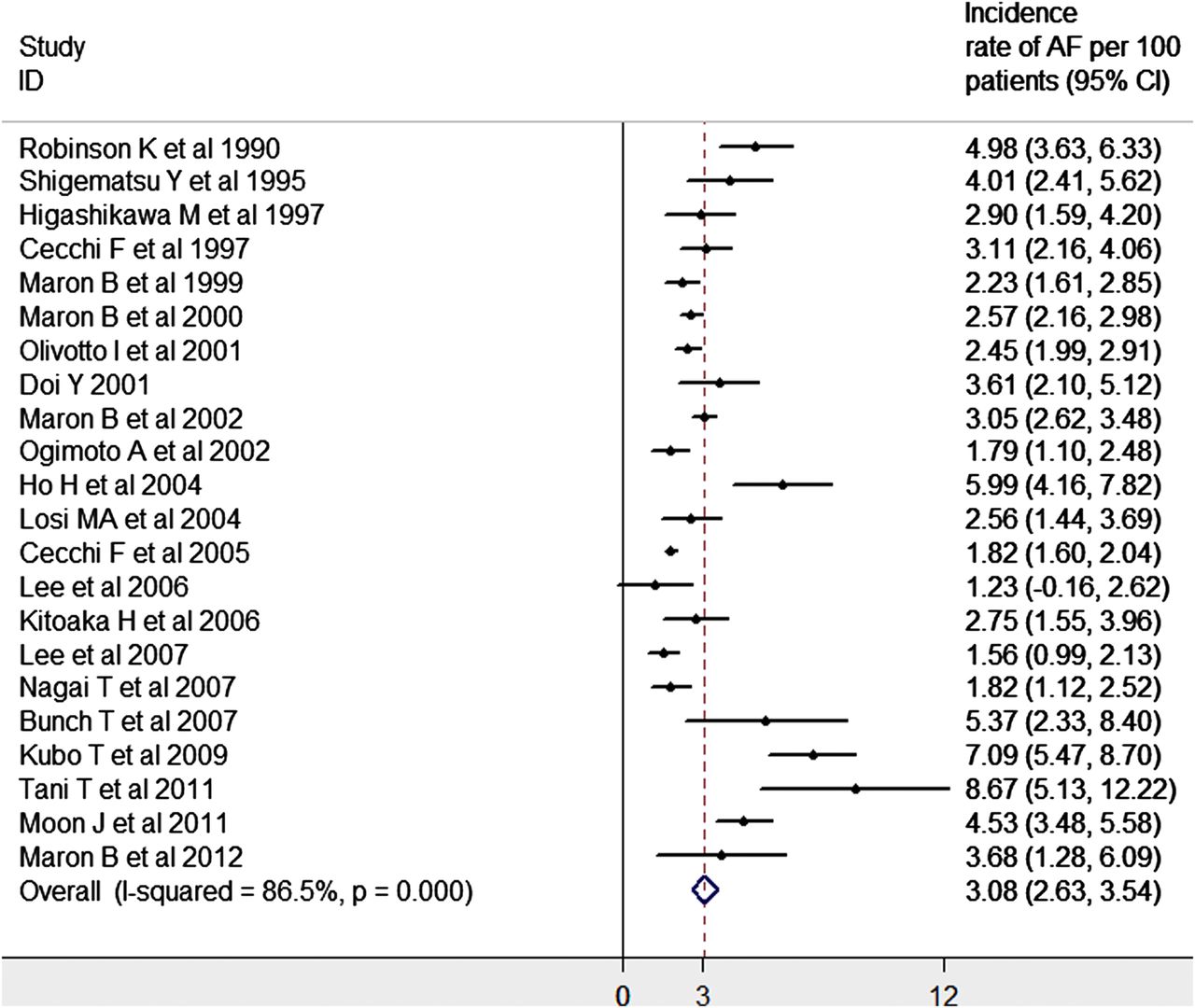
Incidence of atrial fibrillation (AF). The forest plot from random effect meta-analysis shows study specific incidence and the pooled (overall) incidence of AF. The heterogeneity between the study was estimated as I2=86.5% (p<0.01). The overall incidence rate is 3.08 per 100 patients per year.
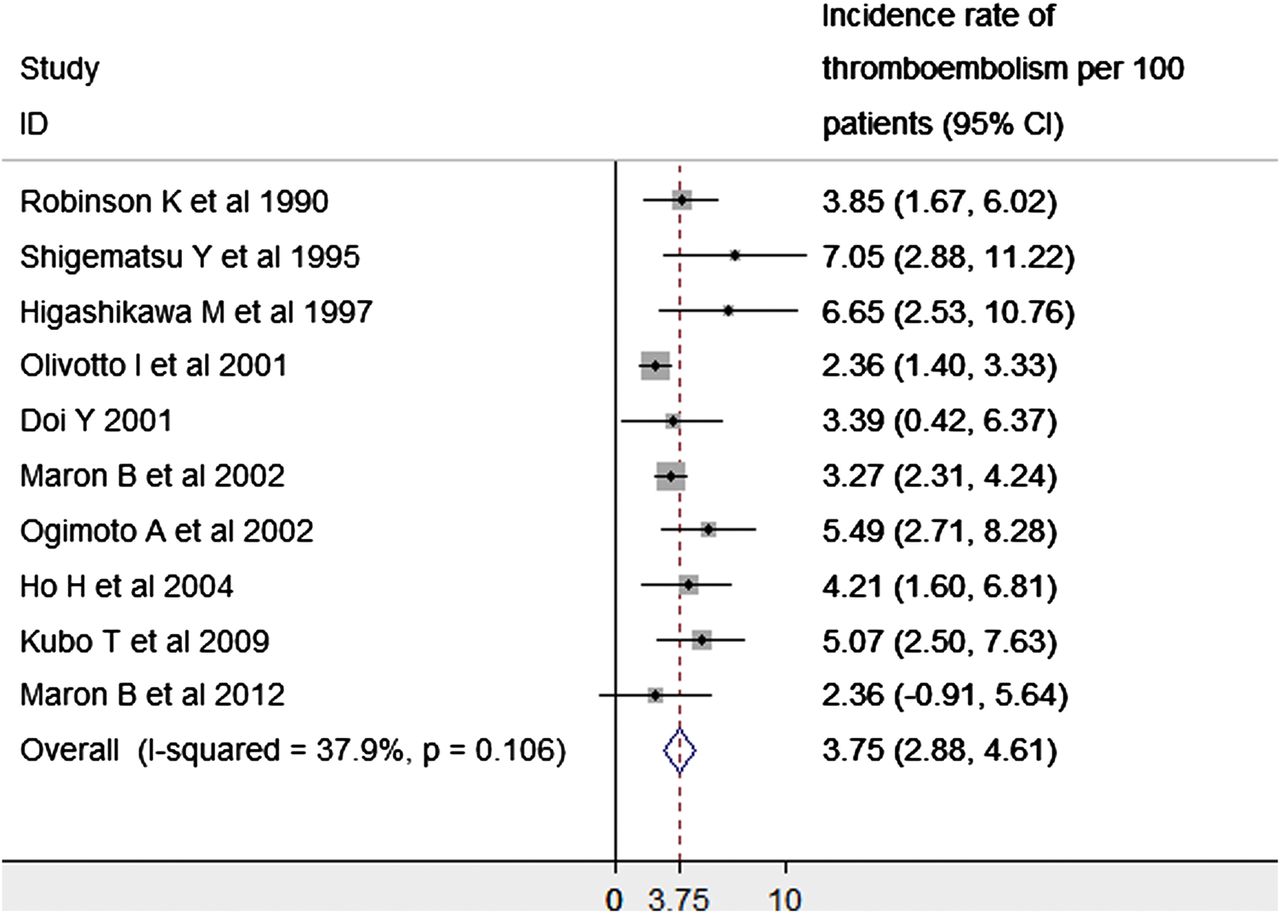
Incidence of thromboembolism. The forest plot from random effect meta-analysis shows study specific incidence and the pooled (overall) incidence of thromboembolism in patients with hypertrophic cardiomyopathy and atrial fibrillation . The heterogeneity between the study was estimated as I2=37.9% (p=0.1). The overall incidence rate is 3.75 per 100 patients per year.
Predictors of AF and thromboembolism
The lack of patient level data and heterogeneity between studies means that it is not possible to model clinical predictors of AF and thromboembolism. Left atrial (LA) size and volume were associated with the development of AF in 15 studies and for the development of thromboembolism in three studies. Age was reported as a predictor of AF in seven studies and of thromboembolism in two studies. Other variables reported to be associated with an increased risk of AF and thromboembolism are shown in online supplementary tables S1 and S2.
The pooled overall LA diameter in patients with SR was 38.03 mm (95% CI 34.62 to 41.44; figure 6). The heterogeneity between the studies was estimated as I2=0.02% (p=0.95). The pooled overall LA diameter in patients with AF or paroxysmal AF was 45.37 mm (95% CI 41.64 to 49.04; figure 7). The I2 statistic was estimated as I2=0.01% (p=0.96). One study reported an LA diameter of more than 40 mm to be predictive of AF (p<0.01),17 and another an LA diameter of more than 42 mm predictive of AF with a sensitivity of 96% and a specificity of 81%.8

Left atrial (LA) diameter in patients with sinus rhythm (SR). The forest plot from random effect meta-analysis shows study specific LA diameter for patients in SR and the pooled (overall) LA diameter. The heterogeneity between the study was estimated as I2=0.02% (p=0.95). The overall cut-off point or diameter value is 38.03 in patients with SR.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Left atrial (LA) diameter in atrial fibrillation (AF). The forest plot from random effect meta-analysis shows study specific LA diameter for patients in AF or paroxysmal AF and the pooled (overall) LA diameter. The heterogeneity between the study was estimated as I2=0.01% (p = 0.96). The overall cut-off point or diameter value is 45.37 in patients with AF.
Mortality
A meta-analysis of mortality in the AF population was not possible due to limited data. Studies reporting statistically significant higher mortality in patients with AF compared to patients in SR are presented in Otable 1.
Mortality data in available studies in whole population and in AF patients
Treatment of AF
We identified no randomised trials of antiarrhythmic drugs, oral anticoagulants or radiofrequency ablation. The results from observational studies on drug treatment and AF ablation are reported in tables 2 and 3.
AF ablation in patients with hypertrophic cardiomyopathy
Studies of amiodarone treatment and anticoagulation in hypertrophic cardiomyopathy (HCM) patients
Discussion
This review shows that studies on AF in HCM are very heterogeneous with respect to patient characteristics, follow-up duration, inclusion criteria and endpoint definition. All are retrospective and observational in design and there are no randomised control trials of any treatment strategy. The data do show that AF occurs in about a fifth of patients with HCM, and strongly suggest that it is associated with adverse outcomes.
Data quality
Major limitations of existing data are the difference in age and sex distribution in the study populations and the small size (typically less than 150 patients) of most cohorts. There is also substantial variation in inclusion criteria and in the definition of AF. For example, some studies included patients who were in AF at the time of diagnosis,9 ,11 whereas others excluded patients who were in AF at enrolment and reported only on those individuals that developed AF during the follow-up period.7 ,15 ,31 ,36 Similarly, some reports included only patients with paroxysmal AF, but the definition of paroxysmal AF was highly variable in that some included AF only when associated with symptoms,12 ,30 or when the AF was of a prespecified duration.8 ,18 ,25 ,29 Finally, groups of investigators have published their cohorts in more than one study. It is impossible to discern the overlap in patient populations,12 ,14 ,22 ,24 ,27 ,30 ,31 ,36 but the duplicate studies report different follow-up duration and total population size. We therefore conclude that the overall estimate obtained by meta-analysis was not significantly affected.23 ,28 ,31
Prevalence and incidence of thromboembolism
All studies showed that AF in patients with HCM is associated with thromboembolism. The prevalence figures were influenced by duration of follow-up (the two studies reporting the highest prevalence of thromboembolic events had significantly longer duration of follow-up compared to the other studies10 ,16) and by the definition of thromboembolism. For example, some studies consider all thromboembolic events including cerebral and peripheral emboli in the reported prevalence of thromboembolic events,6 ,10 ,11 whereas others only report the prevalence of stroke.16 ,22
Predictors of AF
The pathophysiological conditions that predispose to atrial arrhythmia in patients with HCM are poorly understood, but diastolic dysfunction and mitral regurgitation (usually in the context of outflow obstruction) are a major cause of increased atrial size and stretch. Small cross-sectional studies show associations with myocardial fibrosis detected by gadolinium enhanced cardiac MRI and reduced hyperaemic myocardial blood flow determined using positron emission tomography, but these phenomena are probable surrogates for disease severity rather than specific mechanisms or triggers for AF.29 ,38 Several workers have postulated that patients with HCM have a primary atrial as well as a ventricular myopathy, but supportive evidence for this is scant. While heterogeneity between studies meant that it was not possible to perform a meta-analysis of all suggested predictors for AF and thromboembolism, the majority of reports examining this question found that LA size, LA volume and age were independently associated with AF, suggesting that these should be considered when evaluating individual patients’ risk of developing AF.
There are no prospective randomised trials of any therapy for AF in HCM and, as this review shows, only limited observational data on pharmacological and non-pharmacological treatment strategies.11 ,17 ,22 Evidence that amiodarone therapy maintains SR and reduces embolic episodes comes from a single study.11 Data on warfarin use are similarly limited, but there are observational data reporting a lower incidence of stroke in patients treated with warfarin compared to those on antiplatelet therapy or no treatment.13 ,14 ,22
To date only small non-randomised studies have examined the efficacy of AF ablation in HCM, but the data accrued so far suggest that repeat procedures are frequently required and long term maintenance of SR is achieved in no more than 50–60% of patients.39 ,40––42
Limitations
The review examined only those studies that investigated AF and/or stroke or thromboembolism as primary or secondary outcome, but we acknowledge that data on prevalence of AF are included in other observational cohort studies reporting on other aspects of the disease.
Conclusions
This review shows that the published literature is insufficient to create a robust clinical tool for the prediction of AF or thromboembolic risk. Nevertheless, most data suggest that once patients have AF, they have a high risk of thromboembolism and should be anticoagulated. More challenging is the management of patients with LA enlargement but no evidence for atrial arrhythmia. Given that LA diameter and volume are consistently shown to be independently associated with AF, patients with atrial enlargement should as a minimum be monitored on a regular basis in order to detect AF. The role of prophylactic anticoagulation in this group should be evaluated in randomised prospective trials.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table 1
- Data supplement 2 - Online table 2
Footnotes
-
Contributors OPG: contributed to: conception and design, acquisition of data, and analysis and interpretation of data; drafting the article or revising it critically for important intellectual content and final approval of the version to be published. MSR: contributed to: analysis and interpretation of data; drafting the article or revising it critically for important intellectual content and final approval of the version to be published. CO’M: contributed to: acquisition of data, and drafting the article or revising it critically for important intellectual content and final approval of the version to be published. AA: contributed to: analysis and interpretation of data; drafting the article or revising it critically for important intellectual content and final approval of the version to be published. PME: contributed to: conception and design, interpretation of data; drafting the article or revising it critically for important intellectual content and final approval of the version to be published.
-
Funding OPG received research support from the British Heart Foundation (FS/12/86/29841).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.