Article Text

Abstract
Context Despite the high incidence of hypertension, the elderly population is not represented in clinical trials as they have upper age limits or do not present age-specific results.
Objectives The present study was designed to systematically review prospective randomized trials and assess the effects of antihypertensive treatment on cardiovascular, all-cause mortality, stroke and heart failure in patients over 65 years of age.
Data Sources We systematically searched the electronic databases, MEDLINE, PUBMED, EMBASE and Cochrane for prospective randomized studies (1970–2012) in which patients were randomized either to antihypertensive treatment and non-drug control group or to different antihypertensive treatments.
Study selection We identified 18 clinical studies, with 19 control arms and 19 treatment arms examining 59285 controls, 55569 hypertensive patients with an average follow up duration of 3.44 years. The mean age of patients on treatment was 71.04 years.
Data Extraction Included studies were divided and analyzed in 2 subgroups: i) studies comparing treatment group vs non-drug placebo group with a BP decrease of 27.3/11.1 mmHg and ii) studies comparing two anti-hypertensive regimens with baseline BP ∼157/86, and BP reduction to less than 140/80.
Results A significant reduction in all four outcomes was found in the first group of studies. In the second group similar BP reduction resulted in equivalent risk reduction in both treatment groups. In the meta-regression analysis mean SBP difference was linearly associated with all-cause, cardiovascular, stroke and heart failure risk reduction.
Conclusion Reducing BP to a level of 150/80 mmHg is associated with large benefit in stroke, cardiovascular and all-cause mortality as well as heart failure risk in elderly individuals. Different antihypertensive regimens with equal BP reduction have similar effects on cardiovascular outcomes. SBP rather than DBP reduction is significantly related to lower cardiovascular risk in this population.
- Antihypertensives
- Hypertension
- Elderly
Statistics from Altmetric.com
Introduction
The prevalence of hypertension in the US population increases progressively with age, and so the majority of elderly are hypertensive. Among participants of the Framingham Heart Study with a normal blood pressure (BP) at age 55, 90% eventually developed hypertension.1 Hypertension in elderly patients is a strong cardiovascular risk factor that affects women more than men and occurs in essentially all races, ethnic groups and countries. The prevalence of hypertension among women 65 and older is over 70% compared with an approximately 65% prevalence rates among men 65 and older.2 Elderly individuals (≥65 years) are more likely to have isolated systolic hypertension, cardiovascular events, target organ damage and are less likely to have hypertension controlled. Despite the high incidence of hypertension, the elderly population is not represented in clinical trials as they have upper age limits or do not present age-specific results. Although several clinical trials have reported beneficial results of treating hypertension in the elderly, these studies have not provided a specific BP value that could be used to use as a target for treatment.
In very old individuals (above 80-years-old) with moderate to severe hypertension, the Hypertension in the Very Elderly (HYVET) trial showed that lowering BP to a goal of 150/80 mm Hg with a combination of low-dose thiazide and with or without an ACE inhibitor (ACE-I) reduced all-cause mortality and non-fatal strokes.3 Among individuals older than 65 years, the risk of Cardiovascular (CV) events continues to increase with the rising systolic blood pressure (SBP). However, studies have proposed that in people with angina a J-shaped curve exists diastolic blood pressure (DBP) reduction to 80 mm Hg decreases the risk of cardiovascular events, but further DBP reduction below 60 mm Hg increases the event rates.4–,6 Evidence about the optimal BP target comes from trials randomly assigning patients to a specified treatment versus another drug or regimen or placebo.
The present study was designed to systematically review prospective randomised trials and assess the effects of antihypertensive treatment on cardiovascular mortality, all-cause mortality, stroke and heart failure and their correlation with BP reduction in patients over 65 years of age.
Materials and methods
Search strategy
We systematically searched the electronic databases, MEDLINE, PUBMED, EMBASE and the Cochrane Library for Central Register of Clinical Trials, using the Medical Subject Headings (MeSH) terms, ‘hypertension or blood pressure’ and ‘elderly or patients over 65 years’ and ‘cardiovascular mortality or all-cause mortality or stroke or heart failure’ and ‘randomised trial’. We limited our search to studies in human subjects and English language in peer-reviewed journals published until December 2012. Additionally, a manual search of all relevant references from the screened articles and reviews of statins was performed for additional clinical studies (figure 1).

Preferred Reporting Items for Systematic Reviews and Meta-analyses flow diagram of study selection.
Study selection
We included only prospective randomised, controlled trials with primary and secondary endpoints including cardiovascular mortality, all-cause mortality, stroke and heart failure, published as original articles in peer-reviewed scientific journals in English. We excluded those trials that did not report any of the following variables: number of events in both the treatment and control groups, length of study, description of the main relevant features of the study population, including gender, age, hypertensive status, description of concomitant therapy, and difference between baseline and end-of-treatment SBP and DBP in intervention and control groups.
Data extraction and quality
The data were independently extracted by two authors (VA and AB) using standardised protocol and reporting form (table 1). Disagreements were resolved by arbitration, and consensus was reached after discussion. We extracted characteristics of each study (type of design with duration of intervention and methods), baseline demographics, number of cardiovascular mortality, all-cause mortality, cerebrovascular and heart failure events as well as SBP and DBP at baseline and at the end of the study for our analysis. The authors of the papers were individually contacted in case the data were unclear. Cochrane's risk of bias tool has been used in order to assess the individual risk of bias of each study.7 The criteria used for quality assessment were sequence generation of allocation, allocation concealment, masking of participants, staff and outcome assessors, incomplete outcome data, selective outcome reporting, and other sources of bias. The two authors independently assessed the risk of bias in each eligible trial. Low quality studies had two or more quality assessment criteria qualified as high or unclear risk of bias.
Characteristics of studies included in the meta-analysis
Outcomes assessed
Our primary outcome was difference in the all-cause mortality, cardiovascular mortality, stroke and heart failure rates between the treatment and control groups.
Data analysis and synthesis
An intention-to-treat traditional meta-analysis was performed in line with recommendations from the Cochrane Collaboration and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Statement. All analyses were performed by Review Manager (RevMan) 5.1 (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011). χ² Test of heterogeneity and the I2 statistic of inconsistency were used to assess heterogeneity between studies. Statistically significant heterogeneity was defined as an χ² p value less than 0.05 or an I2 statistic greater than 75%. In the absence of heterogeneity, pooled estimates of relative risks (RRs) with their 95% CIs were calculated using the Mantel–Haenszel method. A DerSimonian–Laird random-effects model for RR estimation for all outcomes was used in the presence of heterogeneity. Reported values are two-tailed, and hypothesis testing results were considered statistically significant at p=0.05. Small study effect, including publication bias, was tested using funnel plot and Egger test. If publication bias was found, the non-parametric trim and fill method of Duvall and Tweedie was performed to add studies that appeared to be missing. We separately analysed the various groups of statins. We separately examined if there were any differences in the outcomes between the studies that included an uptitration of the antihypertensives during the study versus the studies that kept the dosages of the antihypertensives stable. Meta-regression (OpenMeta analyst) was used to assess whether age, on-treatment SBP and SBP differences score were associated with the effect of treatment on primary outcomes.
No extramural funding was used to support this work. The authors are solely responsible for the design and conduct of this study, all study analyses, the drafting and editing of the paper and its final contents.
Results
Study selection
We identified 18 clinical studies (figure 1), with 19 control arms and 19 treatment arms, which examined the effects of antihypertensive treatment on all-mortality, cardiovascular mortality, stroke risk and heart failure rates based on our inclusion and exclusion criteria (table 1). We included studies of hypertensive patients with mean age above 65 years. These studies enrolled 59 285 controls and 55 569 hypertensive patients with an average follow-up duration of 3.44 years. The mean age of patients on treatment was 71.04 years.
Included studies were divided and analysed in two subgroups: (i) studies comparing treatment group versus non-drug placebo group3 ,8–15 ,16 and (ii) studies comparing two treatment groups with different effects on BP control.17–24 We excluded two pilot studies of trials included in the analysis (SHEP-pilot25 and HYVET-pilot studies26). The Cardiovascular Trial in the Elderly study27 was excluded because of non-specific antihypertensive treatment in the control group. Finally, trials that met the inclusion criteria but which studied antihypertensive agents not currently used for treatment of hypertension in elderly (eg, methyldopa,28 ,29 deserpidine,29 bethanidine30) were excluded from the analysis.
Quality assessment
On the basis of quality assessment, 14 were deemed to be at low risk of bias and the remainder four to be at high risk.9 ,12–14
Effects of antihypertensive treatment on blood pressure
In the first subgroup of studies, BP was decreased in the treatment group from 176.6/88.6 to 149.3/77.4 mm Hg (control group from 176.7/88.4 to 162.8/83.1 mm Hg). In the second subgroup of studies, BP was lower in one arm (mean difference between groups: SBP −2.37 mm Hg (95% CI −0.42 to −4.31, p=0.02) and DBP −0.73 (95% CI 0.05 to −1.45, p=0.05)), with significant heterogeneity between studies (p<0.001).
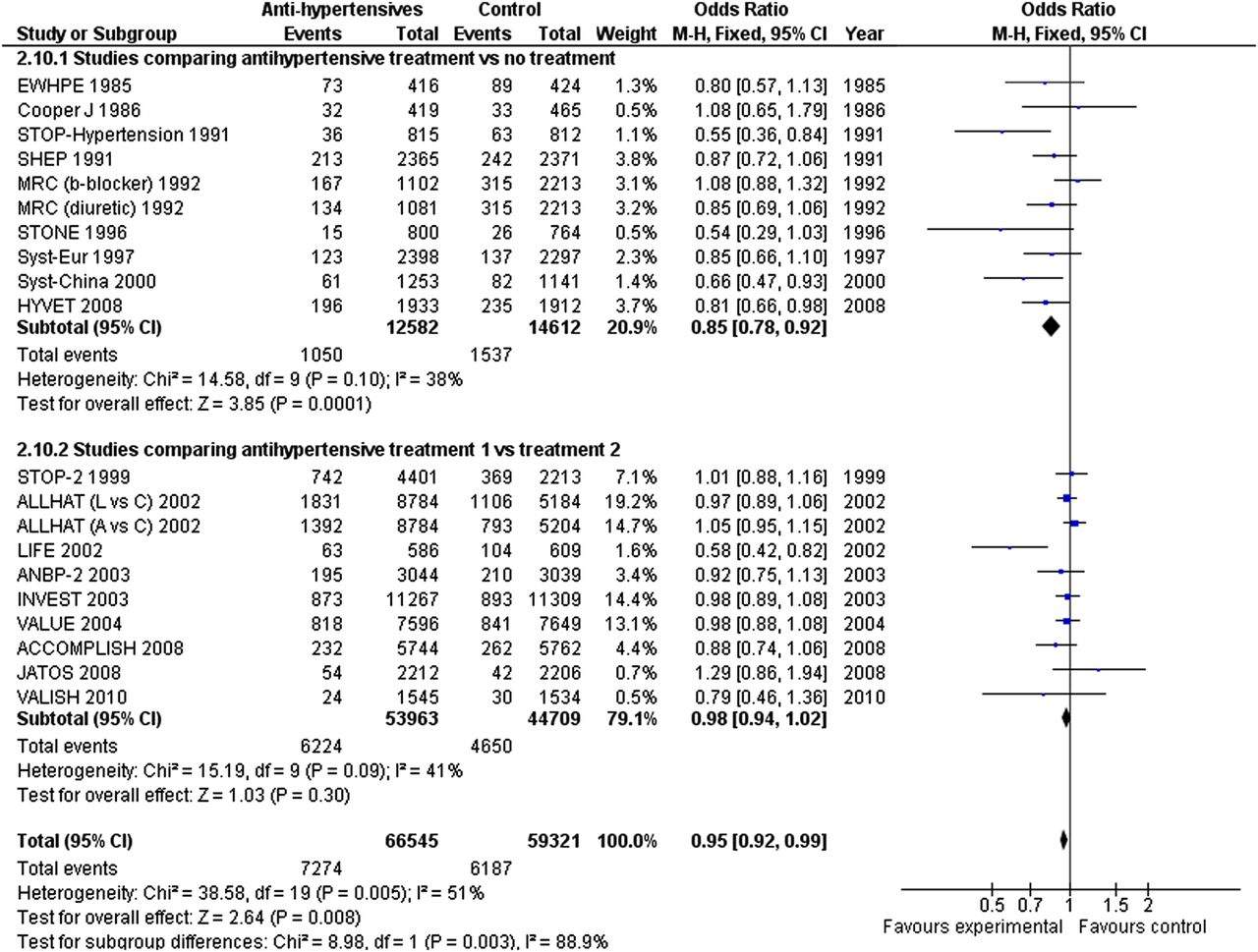
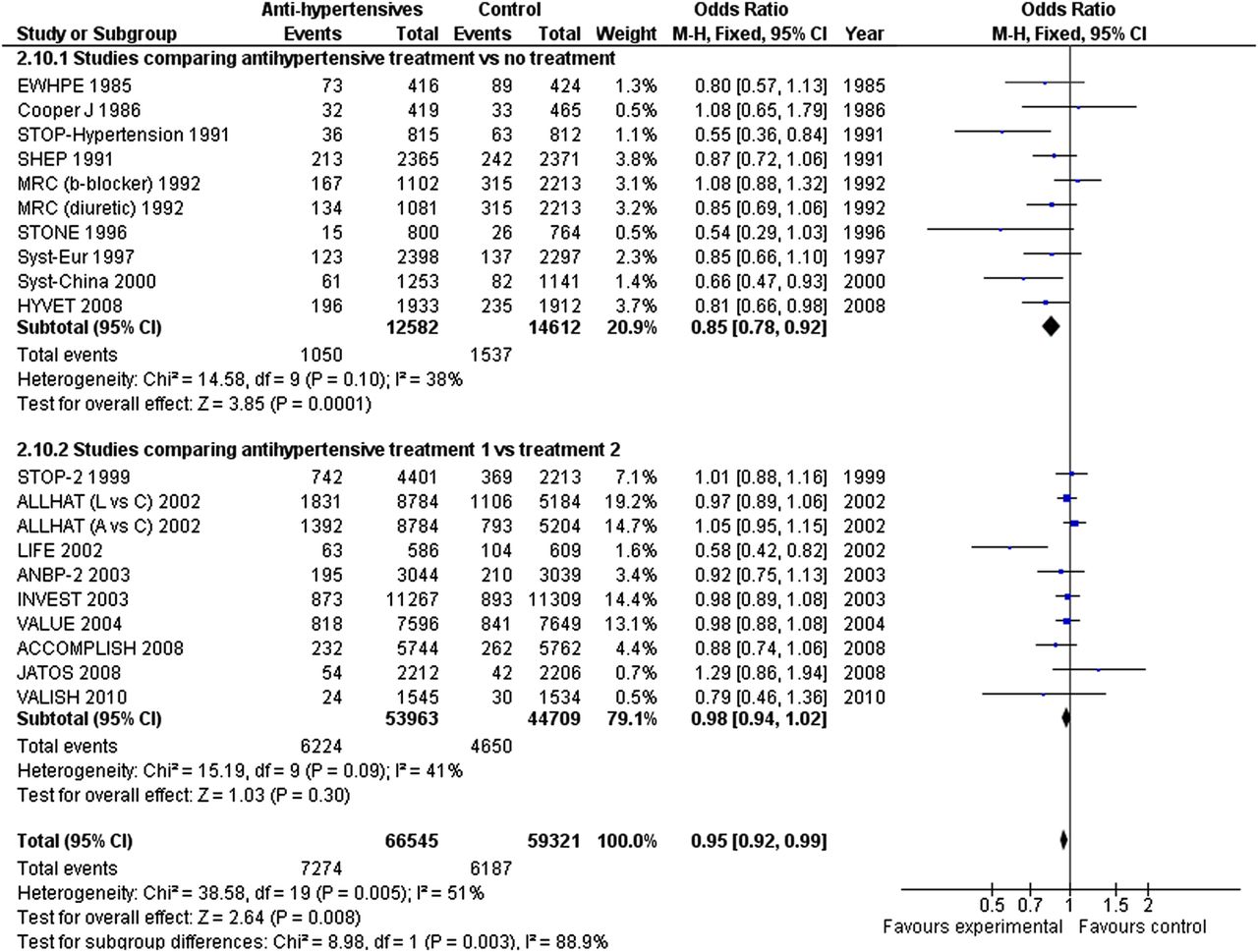
All-cause mortality: In the first group of studies antihypertensive treatment reduced all-cause mortality (OR 0.85; 95% CI 0.78 to 0.92; p<0.0001) (figure 2). However in the second group of studies, lowering BP to 137.3/76.3 mm Hg did not change all-cause mortality (OR 0.98; 95% CI 0.94 to 1.02; p=0.30) compared with the group with higher BP 140.3/77.2 mm Hg. In the subgroup analysis of studies with patients over 70 years, antihypertensive treatment decreased all-cause mortality in the first group of studies (OR 0.86; 95% CI 0.79 to 0.94; p=0.001)3 ,8 ,10 ,11 ,15 ,23 while it did not significantly affect it in the second group (OR 0.99; 95% CI 0.89 to 1.11; p=0.91).12 ,17 ,19 ,20 When studies with baseline SBP<160 mm Hg21 ,22 ,24 were excluded from the sensitivity analysis of the second group, the all-cause mortality risk was not significantly reduced (OR 0.95; 95% CI 0.85 to 1.05; p=0.28).
Fixed-effect meta-analysis for all-cause mortality. The figure presents number of events, number of patients in treatment and control groups, OR and 95% CI for each trial, overall OR estimate with 95% CI and p value for association test, p value for heterogeneity test and between-trial inconsistency (I2) measures.
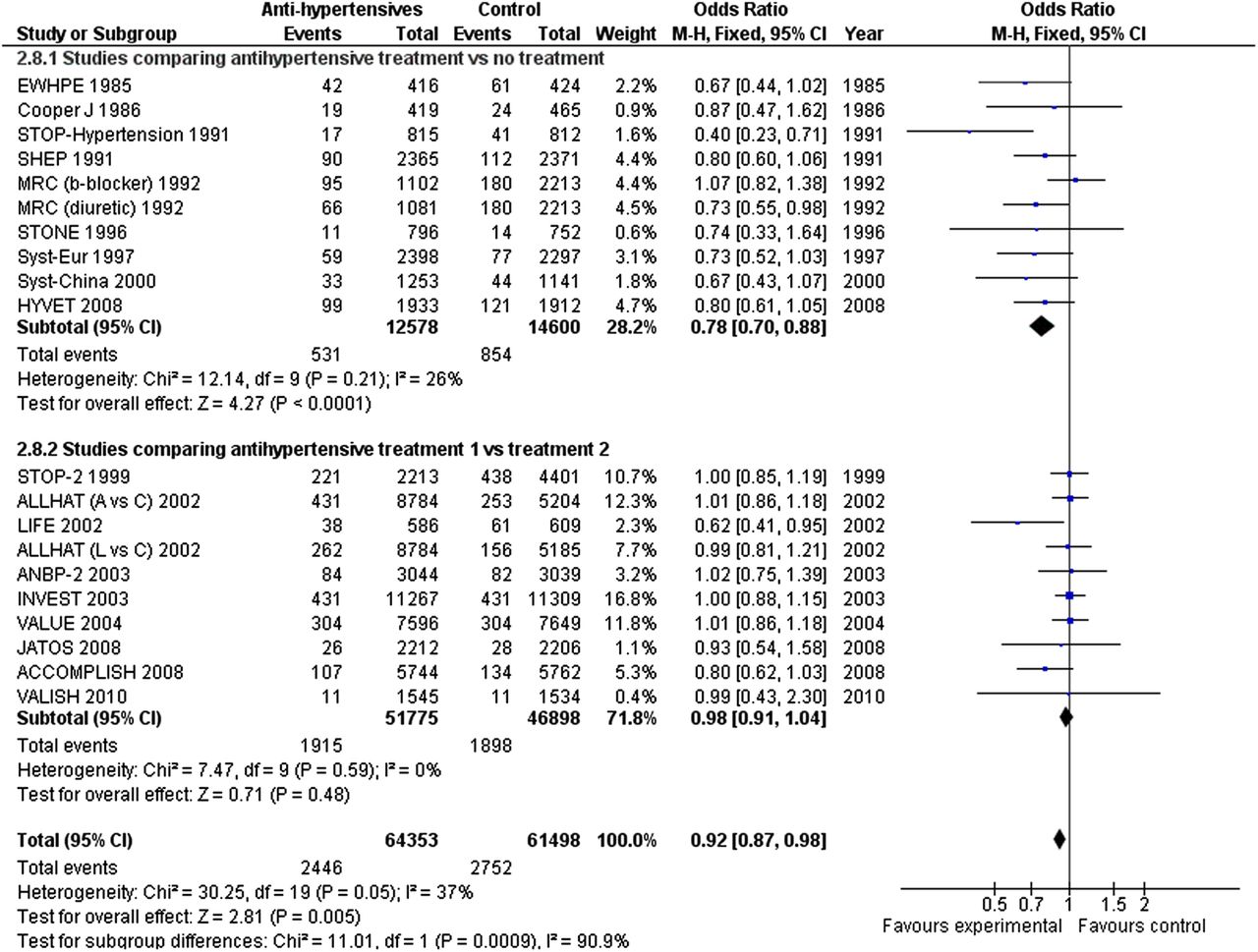
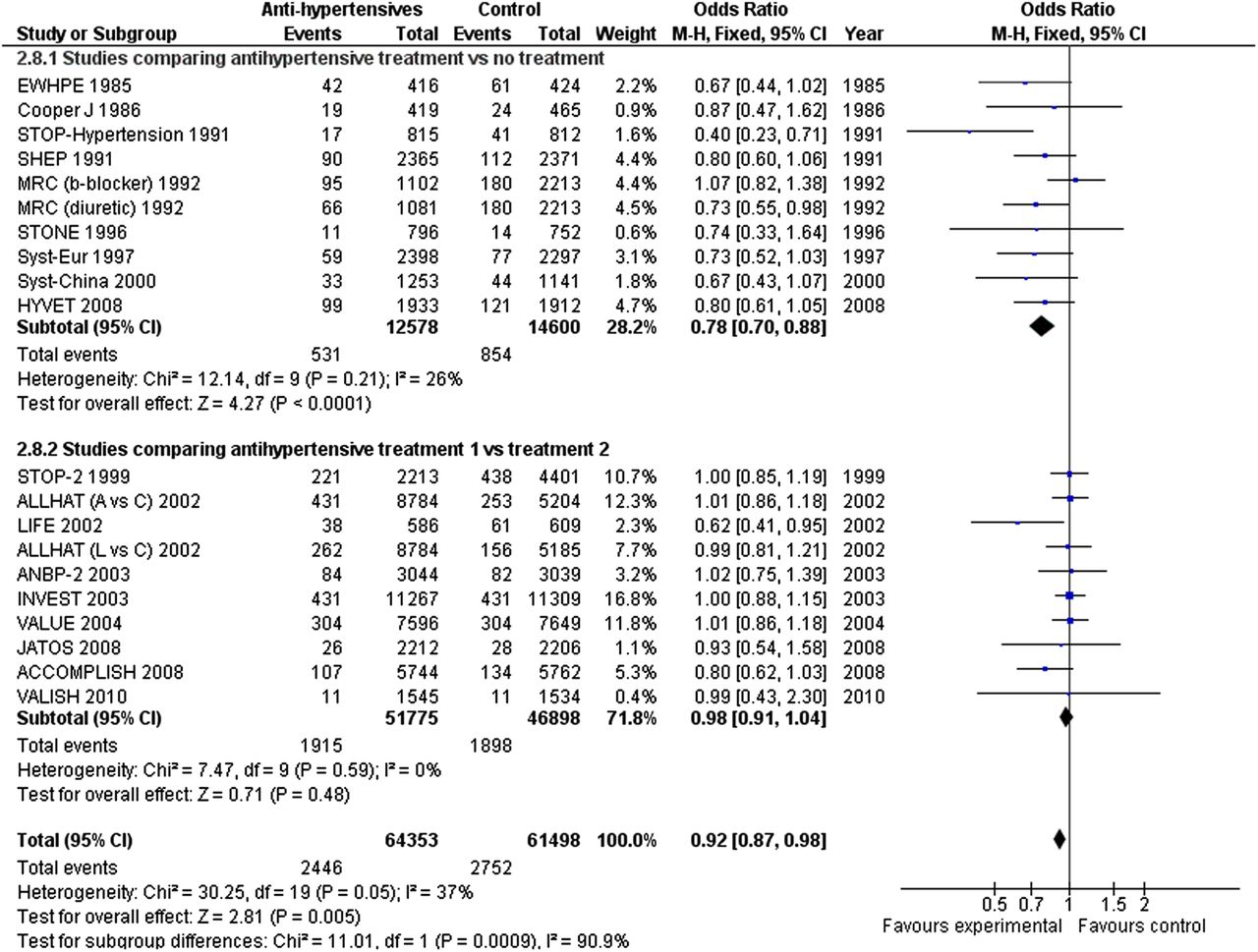
Cardiovascular mortality: There was significant reduction in cardiovascular mortality with treatment in the first group of studies (OR 0.78; 95% CI 0.70 to 0.88; p<0.0001) (figure 3). In the second group, lower BPs did not significantly change cardiovascular mortality (OR 0.98; 95% CI 0.91 to 1.04; p=0.48). The subgroup analysis showed lower cardiovascular mortality in the first group of studies with patients over 70 years (OR 0.79; 95% CI 0.70 to 0.89; p<0.0001) but not in the second group (OR 1.00; 95% CI 0.87 to 1.15; p=0.98). When studies with baseline SBP<160 mmHg were excluded, a small non-significant reduction of cardiovascular mortality was seen (OR 0.95; 95% CI 0.83 to 1.09; p=0.49).
Fixed-effect meta-analysis for cardiovascular mortality.
Stroke: In both groups, there was a significant decrease of stroke risk (large reduction in the first group, OR 0.63; 95% CI 0.56 to 0.71; p<0.0001 and modest reduction in the second group, OR 0.91; 95% CI 0.85 to 0.98; p=0.007) (figure 4). However, in the subgroup analysis of patients over 70 years, the stroke risk was significantly decreased in the first group only (first group OR 0.64; 95% CI 0.56 to 0.73; p<0.0001 and second group OR 0.93; 95% CI 0.81 to 1.06; p=0.27). Stroke risk reduction did not reach statistical significance when studies with baseline SBP<160 were excluded from the second group (OR 0.91; 95% CI 0.81 to 1.04; p=0.16).

Fixed-effect meta-analysis for stroke.
Heart failure: Not all studies included heart failure risk as part of the primary or secondary endpoints. In the first group,3 ,8 ,9 ,10 ,13 ,15 heart failure risk was significantly decreased (OR 0.54; 95% CI 0.44 to 0.66; p<0.0001) (figure 5). Similarly, in the second group,18–,24 lower BP decreased heart failure risk (OR 0.91; 95% CI 0.86 to 0.96; p=0.001). In the subgroup analysis of patients over 70 years, of the first group heart failure risk remained significantly decreased (OR 0.53; 95% CI 0.43 to 0.66; p<0.0001) whereas no reduction was found in the second group of studies (OR 0.94; 95% CI 0.80 to 1.10; p=0.42). Excluding studies with baseline SBP<160 non-significantly reduced risk (OR 0.88; 95% CI 0.76 to 1.03; p=0.11).
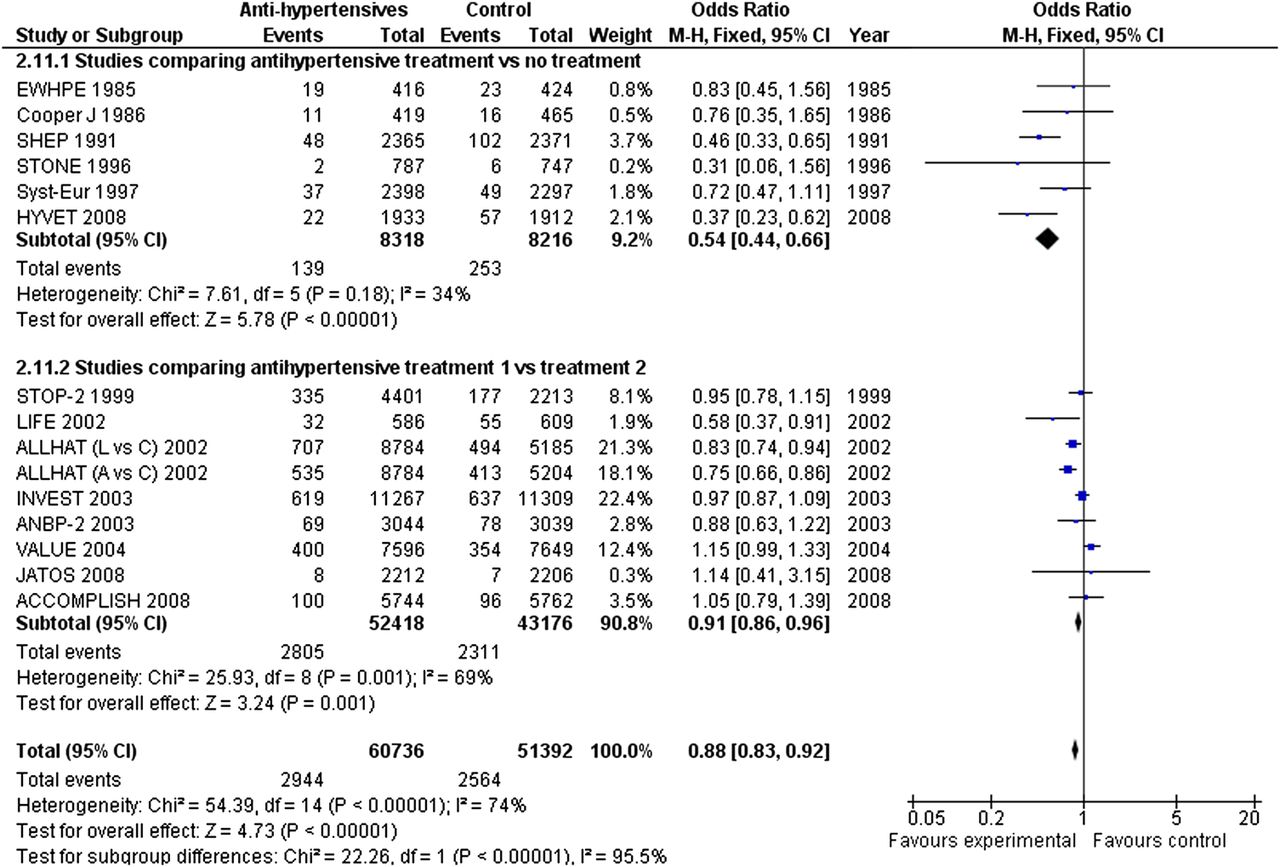
Fixed-effect meta-analysis for heart failure.
Publication bias
The funnel plot did not show asymmetry consistent with publication bias, and Egger's test was not significant for the outcomes studied.
Meta-regression analysis
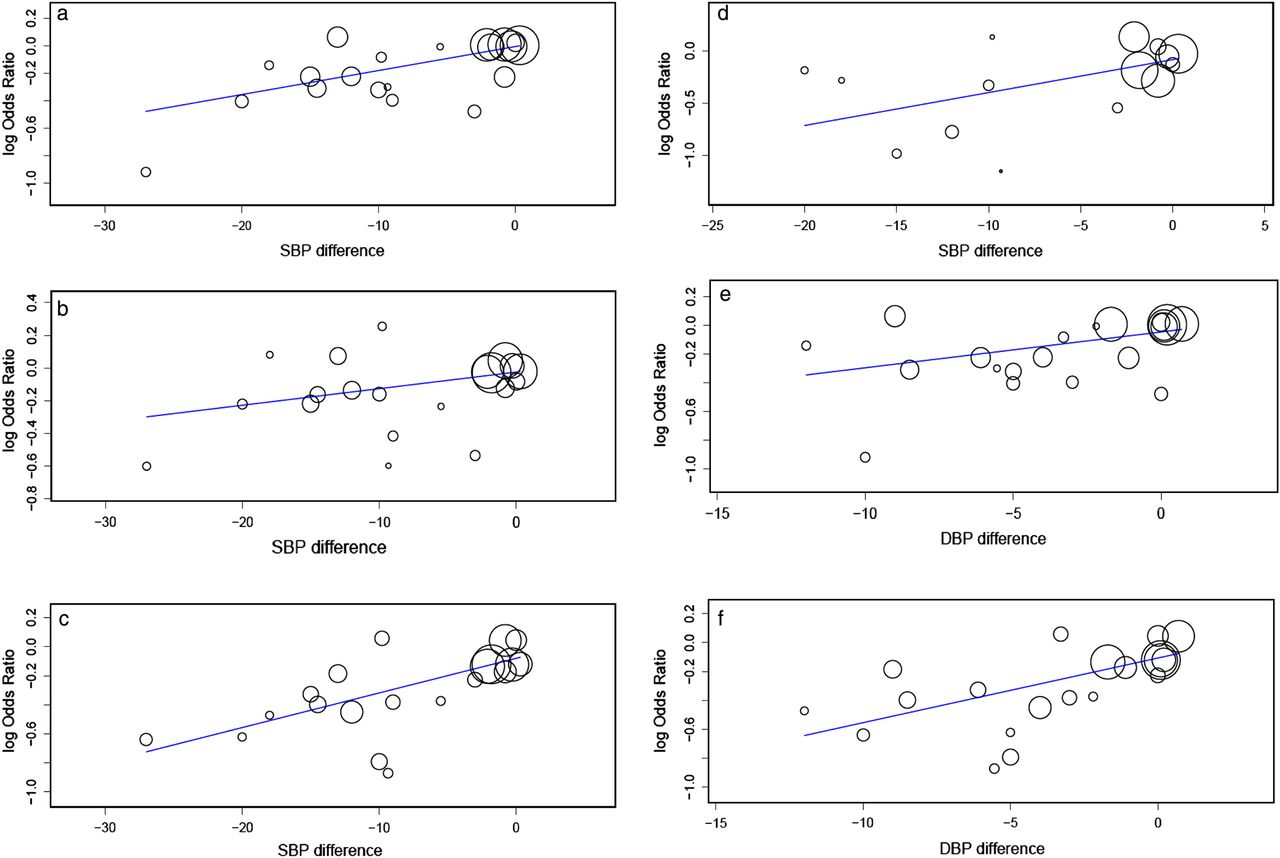
We performed a meta-regression analysis which demonstrated no evidence that age was significantly related to the effects of treatment on outcomes (p = 0.672 for all-cause mortality, 0.783 for cardiovascular mortality, 0.692 for stroke and 0.514 for heart failure). However, on-treatment SBP difference was inversely associated with cardiovascular mortality (slope coefficient 0.017; 95% CI 0.008 to 0.027; p<0.001, figure 6A), all-cause mortality (slope coefficient 0.01; 95% CI 0.002 to 0.019; p=0.018, figure 6B), stroke (slope coefficient 0.024; 95% CI 0.013 to 0.035; p<0.001, figure 6C) and heart failure (slope coefficient 0.032; 95% CI 0.010 to 0.053; p=0.004, figure 6D). DBP difference was inversely associated with cardiovascular mortality (slope coefficient 0.025; 95% CI 0.004 to 0.046; p=0.019) and stroke (slope coefficient 0.045; 95% CI 0.022 to 0.068; p<0.001) but not all-cause mortality (p=0.756) and heart failure (p=0.061).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A–D) Linear meta-regression between the log transformed value of (A) cardiovascular mortality, (B) all-cause mortality, (C) stroke, (D) heart failure, OR and on-treatment systolic blood pressure difference, (E) cardiovascular mortality and (F) stroke, OR and on-treatment diastolic blood pressure difference.
Discussion
In an effort to evaluate the effects of antihypertensive treatment on cardiovascular outcomes in patients over 65 years, we performed a systematic review of the published medical literature and analysed 18 prospective randomised studies. Subgroup analysis of these trials suggested a marked improvement of all-cause mortality, cardiovascular mortality, stroke and heart failure risk when BP was decreased by 27.3/11.1 mm Hg on treatment. In a subgroup analysis of studies comparing two antihypertensive regimens with baseline BP ∼157/86 mm Hg, reduction to less than 140/80 mm Hg modestly decreased stroke and heart failure risk but did not affect all-cause and cardiovascular mortality. Different antihypertensive regimens resulted in similar risk reduction. In the subgroup analysis of studies with patients over 70 years, the beneficial effects of antihypertensive treatment remained significant in the first group of studies. Meta-regression analysis showed that on-treatment SBP difference but not age was inversely associated with all-cause and cardiovascular mortality, stroke and heart failure. On-treatment DBP change was inversely associated with cardiovascular mortality and strokes but not all-cause mortality and heart failure.
The results of our analysis are consistent with the findings of the HYVET study, the largest double-blind, placebo-controlled trial of hypertensive patients over 80 years. The results of HYVET trial provided evidence on the efficacy of antihypertensive treatment on cardiovascular mortality, fatal and non-fatal stroke and heart failure.3 A 2009 Cochrane review that included 15 studies and approximately 24 000 subjects also found that treatment improved rates of all-cause, cardiovascular and cerebrovascular mortality.31 Two recent trials involving Asian populations reported clinical outcomes in elderly patients.17 ,19 Both studies showed no additional benefit of antihypertensive treatment on cardiovascular outcomes and stroke when the target SBP was less than 140 mm Hg. Among elderly individuals, cardiovascular outcomes vary directly with systolic and pulse pressure, whereas the association with DBP is not clear. Analyses of the SHEP10 and INVEST16 trials showed significant increases in cardiovascular events when DBP was ≤60 mm Hg. However, the proposed J-shaped curve of cardiovascular outcomes with DBP is not an adverse effect of antihypertensive treatment but an indicator of increased arterial stiffness and advanced vascular disease. Although our analysis showed that greater DBP change was associated with lower cardiovascular mortality and stroke, mean on-treatment DBP remained above 70 mm Hg.
Among reviewed studies only two had treat-to-target design.17 ,19 Both included Japanese low-risk to intermediate risk (less than 20% had cardiovascular disease) hypertensive patients and showed no benefit in treating elderly patients to an SBP target of lower than 140 mm Hg compared with SBP targets lower than 150 and 160 mm Hg. VALISH17 randomly assigned 3079 patients aged 70–84 years (mean age 76 years) with isolated systolic hypertension to a target SBP of lower than 140 mm Hg or 140–149 mm Hg. Initial therapy in both groups was valsartan once daily with other medications added as necessary to achieve targets. After 3.1 years, there was no statistically significant difference between the two groups in the primary composite outcome. Similarly, in JATOS trial,19 more than 4000 Japanese hypertensive patients were randomised to an SBP target of less than 140 mm Hg or 140–159 mm Hg. The main therapy was a calcium channel blocker. After 2 years of follow-up, no difference in the primary endpoint between the two groups was observed. In both trials, antihypertensive therapy resulted in a greater than 20 mm Hg SBP reduction in all groups. Despite the occurrence of fewer events than predicted and the inclusion of low-risk Asian-only hypertensive patients, the results of these trials were consistent.
In the second group of studies, different antihypertensive regimens were included. The ACCOMPLISH trial suggested greater benefit on cardiovascular and renal outcomes with calcium antagonist–ACE-I combination compared with thiazide diuretic–ACE-I combination.21 Whether such a combination would improve outcomes independently from BP reduction in elderly individuals is a hypothesis requiring further validation. A 2011 consensus document issued by ACC/American Heart Association (AHA) states that in elderly patients over 65 years, the recommended goal of BP lower than 140/90 mm Hg was based on expert opinion rather than on data from randomised controlled trials.32 In light of the evidence presented above, the results of our analysis show a potential benefit from a BP target of less than 150/80 mm Hg but do not support SBP lowering at a level of <140 mm Hg.
Limitations
Most included trials have been treatment studies that assigned patients to two or more treatments arms. The preferred type of study to address the optimal BP target would randomise patients to two or more BP targets and treat them with same antihypertensive regimens. Our results are also subject to limitations inherent to any meta-analysis based on pooling of data from different trials with different inclusion criteria, different designs, variable follow-up duration with differing attrition rates and different patient populations. As in other meta-analyses, given the lack of data in each trial, we did not adjust our analyses for compliance to assigned therapy. In addition, the antihypertensive regimens and dosages used in individual studies were different and may have differential effects on outcomes.
Conclusions
Treatment to BP target of ∼150/80 mm Hg or to BP reduction of >25/10 mm Hg effectively decreases all-cause mortality, cardiovascular mortality, stroke and heart failure. Different antihypertensive regimens with equal BP reduction have similar effects on cardiovascular outcomes. SBP rather than DBP reduction is significantly related to cardiovascular risk reduction in patients over 65 years of age.
References
Footnotes
-
Contributors AB: substantial contribution to conception and design, acquisition of data, analysis and interpretation of data and drafting the article. VA: substantial contribution to conception and design, and acquisition of data. DT and CS: general supervision, editing and final approval of the submitted manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The authors attest that the manuscript represents original work, and that it is not under consideration for publication elsewhere.
-
Correction notice This article has been corrected since it was published online. The online version contained the same figure for figure 2 and 4. This has now been rectified in this issue.