Article Text

Abstract
Heart failure with preserved ejection fraction (HFpEF) comprises almost half of the population burden of HF. Because HFpEF likely includes a range of cardiac and non-cardiac abnormalities, typically in elderly patients, obtaining an accurate diagnosis may be challenging, not least due to the existence of multiple HFpEF mimics and a newly identified subset of patients with HFpEF and normal plasma natriuretic peptide concentrations. The lack of effective treatment for these patients represents a major unmet clinical need. Heterogeneity within the patient population has triggered debate over the aetiology and pathophysiology of HFpEF, and the neutrality of randomised clinical trials suggests that we do not fully understand the syndrome(s). Dysregulated nitric oxide–cyclic guanosine monophosphate–protein kinase G signalling, driven by comorbidities and ageing, may be the fundamental abnormality in HFpEF, resulting in a systemic inflammatory state and microvascular endothelial dysfunction. Novel informatics platforms are also being used to classify HFpEF into subphenotypes, based on statistically clustered clinical and biological characteristics: whether such subclassification will lead to more targeted therapies remains to be seen. In this review, we summarise current concepts and controversies, and highlight the diagnostic and therapeutic challenges in clinical practice. Novel treatments and disease management strategies are discussed, and the large gaps in our knowledge identified.
- heart failure with preserved ejection fraction
Statistics from Altmetric.com
Introduction
Heart failure (HF) with preserved ejection fraction (HFpEF) accounts for up to half of all HF in the developed world.1 The reported population prevalence ranges from 1% to 3%, and is predicted to rise further with lengthening life expectancy, greater diagnostic awareness, and increasing rates of obesity, diabetes, hypertension and atrial fibrillation (AF).1 Whether HFpEF constitutes a single syndrome or a collection of syndromes is debated, neverless the diagnostic label identifies patients with a poor quality of life, high rates of hospitalisation and premature mortality.1–3 Clinical guidelines offer few evidence-based treatment recommendations.2–4 Large randomised clinical trials of therapies improving outcomes in HF with reduced EF (HFrEF) have failed to demonstrate prognostic benefit in patients with HFpEF, obliging us to re-examine our understanding of the mechanisms driving morbidity and mortality in this syndrome, and the extent of their reversibility.
In this review, we summarise current ideas, controversies and challenges in the diagnosis and treatment of HFpEF; discuss our understanding of its pathophysiology; and outline novel targeted therapies and disease management strategies under investigation. The large gaps in our knowledge are clearly evident.
Diagnosis
How is HFpEF diagnosed?
Among patients with a clinical diagnosis of HF, the distribution of EF has been reported variably as either unimodal5 or bimodal.6 The decision to dichotomise HF into HFrEF or HFpEF according to an EF of 50% was arbitrary, but has become enshrined in the literature. Current guidelines advocate using EF≥50% as one component of a diagnostic algorithm for HFpEF,2 3 alongside detection of additional myocardial abnormalities to implicate a cardiac cause for symptoms (table 1).2 3 A streamlined method for identifying left ventricular (LV) diastolic dysfunction has been proposed, based on expert opinion.7 The gold standard to confirm (or refute) a diagnosis of HFpEF is based on demonstration of elevated LV filling pressures during cardiac catheterisation, at which time the presence or absence of concomitant pulmonary arterial hypertension can be assessed.2 3 Non-invasive or invasive stress testing is recommended to unmask symptoms (which often occur exclusively on exertion) and diastolic dysfunction, in order to improve diagnostic sensitivity, particularly in individuals with an intermediate pretest probability of HFpEF.8 Other pathologies giving rise to similar symptoms, such as myocardial ischaemia or anaemia, should be actively excluded before a diagnosis of HFpEF is accepted (table 2).
Diagnostic criteria for HFpEF
Differential diagnosis of HFpEF
Areas of diagnostic uncertainty
‘Normal’ levels of B-type natriuretic peptide (BNP) are reported in up to 30% of patients, despite clinical, echocardiographic and invasive haemodynamic evidence of HFpEF.9 The absence of LV dilatation (and thus lower diastolic wall stress) in HFpEF yields lower BNP concentrations and therefore less sensitive discrimination between the normal and HF state. Further ambiguity may be introduced by obesity, which is associated with lower plasma BNP concentrations and possible heightened pericardial restraint,10 and by AF, which is associated with raised plasma BNP concentrations.11 The phenotypic overlap between HFpEF and ‘AF with associated breathlessness and raised BNP’ may be considerable, though prompt different management strategies.
It is unclear whether patients with HF symptoms, preserved EF and more than mild epicardial coronary artery disease (CAD) can be considered to have HFpEF. CAD is widely noted in HFpEF cohorts and HF symptoms that are disproportionate to the severity of CAD or persist after revascularisation may represent one of several proposed HFpEF patient phenotypes.12 Evidence of microvascular ischaemia (eg, as demonstrated by cardiac stress magnetic resonance imaging [MRI]) would be compatible with microvascular inflammation, which is hypothesised to be important in HFpEF.13
In practice, due to the lack of pathognomonic diagnostic criteria and complex requirement for systematic exclusion of other pathologies, in typically elderly patients with multimorbidity, many individuals with breathlessness or fluid retention may be labelled as ‘HFpEF’ without the phenotype being properly established. Cardiopulmonary exercise testing is empirically used to differentiate HFpEF from exercise intolerance due to non-cardiac limitations such as pulmonary disease or deconditioning, though feasibility may be limited in some elderly or frail patients.
Pathophysiology
Does HFpEF simply represent advanced age?
Observational studies report abnormalities in cardiovascular structure and function in HFpEF which exceed those observed in age, sex and body size matched individuals without HF,14 even after adjusting for the cumulative burden of comorbidities.15 Skeletal muscle mass is reduced in HFpEF, beyond that which is observed with normal ageing, and directly contributes to exercise limitation.16 Furthermore, mortality rates among patients with HFpEF exceed those for patients with similar age, sex and comorbidity distribution in trials of hypertension, diabetes and CAD, with a higher proportion of cardiovascular deaths observed in HFpEF.17 These observations suggest that HFpEF is not simply an ageing heart and vascular system. Indeed, the majority of older adults with comorbidities do not develop HFpEF.
Do advancing age and comorbidities contribute to HFpEF pathophysiology?
Late-onset HFpEF may have a different pathophysiology to HFpEF presenting at a younger age. Observational studies suggest that ‘accelerated’ ageing may be a mechanism for ventricular–arterial stiffening in HFpEF, particularly among women.18 Additionally, senile wild-type transthyretin deposition has been associated with HFpEF in predominantly elderly patients.19
Comorbidities are universal in HFpEF cohorts and uniquely influence ventricular and vascular remodelling and prognosis.15 Recently, it has been suggested that comorbidities are integral to the development of HFpEF.13 Cardiometabolic diseases, including obesity, systemic hypertension and diabetes, are proposed to induce a systemic proinflammatory state which in turn triggers systemic and coronary microvascular inflammation. Nitric oxide (NO) bioavailability is reduced and downstream second messenger signalling at the level of the endothelium and cardiomyocyte (reduced cyclic guanosine monophosphate (cGMP) content and protein kinase G (PKG) activity) promotes myocyte and myocardial hypertrophy, cardiomyocyte stiffness and interstitial fibrosis13. This hypothesis reconciles phenotypic diversity in HFpEF cohorts, with findings at cellular and tissue level in human HFpEF biopsies,20 in vivo endothelial dysfunction21 and autopsy evidence of coronary microvascular rarefaction in HFpEF.22
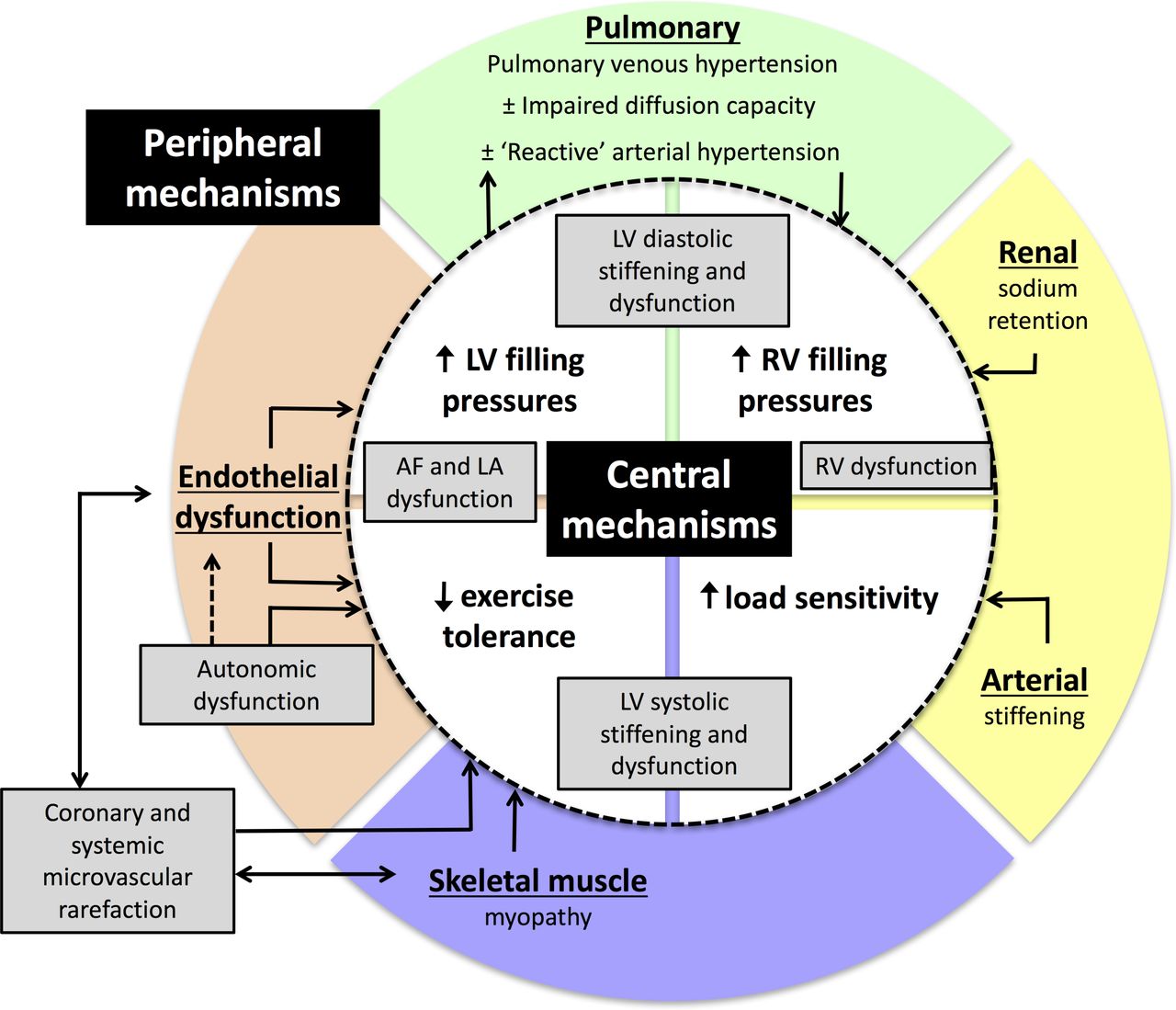
Importantly, however, the heterogeneity of patient characteristics, organ-system involvement and number of pathophysiological abnormalities that have been associated with established HFpEF (Figure 1) support a multifactorial aetiology in most patients. Therefore, identification of vulnerable individuals and specific genetic or environmental aetiological factors is still needed.

Pathphysiological abnormalities associated with the heart failure with preserved ejection fraction syndrome. AF, atrial fibrillation, LA, left atria; LV, left ventricular; RV, right ventricular.
Do distinct pathophysiological subtypes of HFpEF exist?
Pragmatic subphenotypes of HFpEF have been described according to dominant comorbidities or grouped clinical characteristics.23 For example, an HFpEF subphenotype with pulmonary arterial hypertension and right ventricular dysfunction has been well characterised and often signifies advanced stage HF.23 Accumulating evidence suggests that patients with HFpEF and concomitant obesity,10 diabetes15 or AF11 exhibit unique characteristics and a poorer prognosis than patients without these comorbidities. As yet, however, it remains unproven whether these clinical subtypes reflect a spectrum of the same disease or mutually exclusive mechanisms that may respond to different therapies
‘Deep’ phenotyping of individuals with HFpEF, using advanced bioinformatics, is an evolving area of investigation. Initial studies have proposed novel subphenotypes extending beyond individual comorbidity-defined subgroups.23 24 Large dataset-based clustering and machine learning analyses are well suited to model the complex interactions that may contribute to HFpEF pathophysiology . Importantly, however, generalisability and reliability of the output depend on patient selection and the quality and completeness of data entry. Furthermore, ‘omics' methodologies have not yet been applied to HFpEF patient cohorts without elevated BNP or diastolic dysfunction.
Treatment
What is the evidence for current treatment recommendations in HFpEF?
No therapy has yet been shown to improve survival in randomised controlled trials of patients with HFpEF and EF≥50%. Existing treatment recommendations focus on judicious use of diuretics to relieve congestion (when present), and optimal management of comorbidities (table 3).
Current evidence for treatment of HFpEF
What has been learnt from previous trials in HFpEF?
No single reason underlies the neutral or negative outcomes of previous trials (online supplementary table S1). Trials employing a low EF cut-off for HFpEF (eg >40% CHARM-Preserved,25>45% I-PRESERVE26) or recruiting few patients with EF ≥50% (SENIORS27) insufficiently represented symptomatic HFpEF, as defined by current guidelines.3 In TOPCAT, regional differences in placebo group adverse event rates correlated with apparent differences in benefit with spironolactone therapy,28 suggesting possible inappropriate patient inclusion at some sites. The interpretation of PEP-CHF, examining the value of perindopril in the treatment of HFpEF, was hindered by a high drop-out rate (40% treatment arm, 36% placebo arm), and one-third of patients received open-label treatment during the study.29
Supplementary file 1
Therapies targeting the renin–angiotensin system have uniformly failed to demonstrate benefit in HFpEF trials.25 26 28 29 Evidently, neurohumoral stimulation does not exert a dominant impact on the clinical course of unselected patients with HFpEF. RELAX30 tested an alternative therapeutic hypothesis that prevention of cGMP breakdown with phosphodiesterase 5 (PDE-5) inhibition would enhance exercise capacity in patients with HFpEF, but was also neutral. Translational studies have reported low myocardial cGMP content in human HFpEF biopsies;20 hence, low cGMP production may be the key perturbation in HFpEF, rather than excess cGMP breakdown, explaining the neutral result. Since PDE-5 inhibitors improve outcomes in patients with pulmonary arterial hypertension, theoretically targeting patients with HFpEF who have severe pulmonary vascular disease (combined precapillary and postcapillary pulmonary hypertension) may produce a different result.
Randomised controlled trials (RCT) evidence is generally regarded as the most robust evidence for regulatory authorities and guideline writers. Such studies are expensive, often of limited duration, and typically focus on a few ‘hard’ endpoints, such as cardiovascular mortality. However, if HF hospitalisation had been selected as the primary endpoint in CHARM-Preserved25 or TOPCAT,28 the study conclusions might have been different (supplementary table S1).
What therapies for HFpEF are currently under investigation?
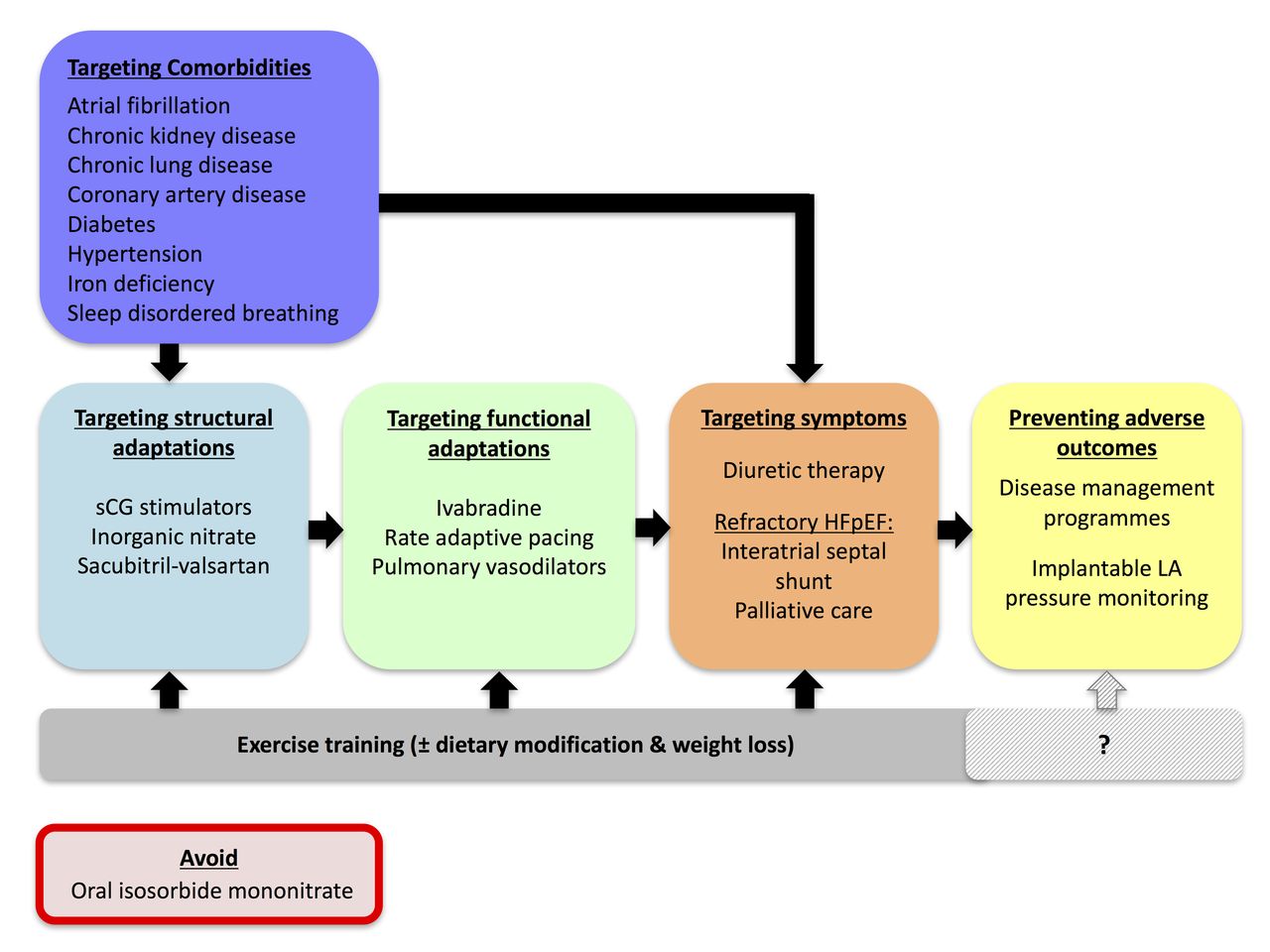
Several novel therapies are currently under investigation in randomised trials (Figure 2)

Therapeutic targets under investigation in HFpEF. HFpEF, heart failure with preserved ejection fraction; LA, left atrial; sCG, soluble guanylate cyclase.
Therapies to modify cellular cGMP and structural adaptations
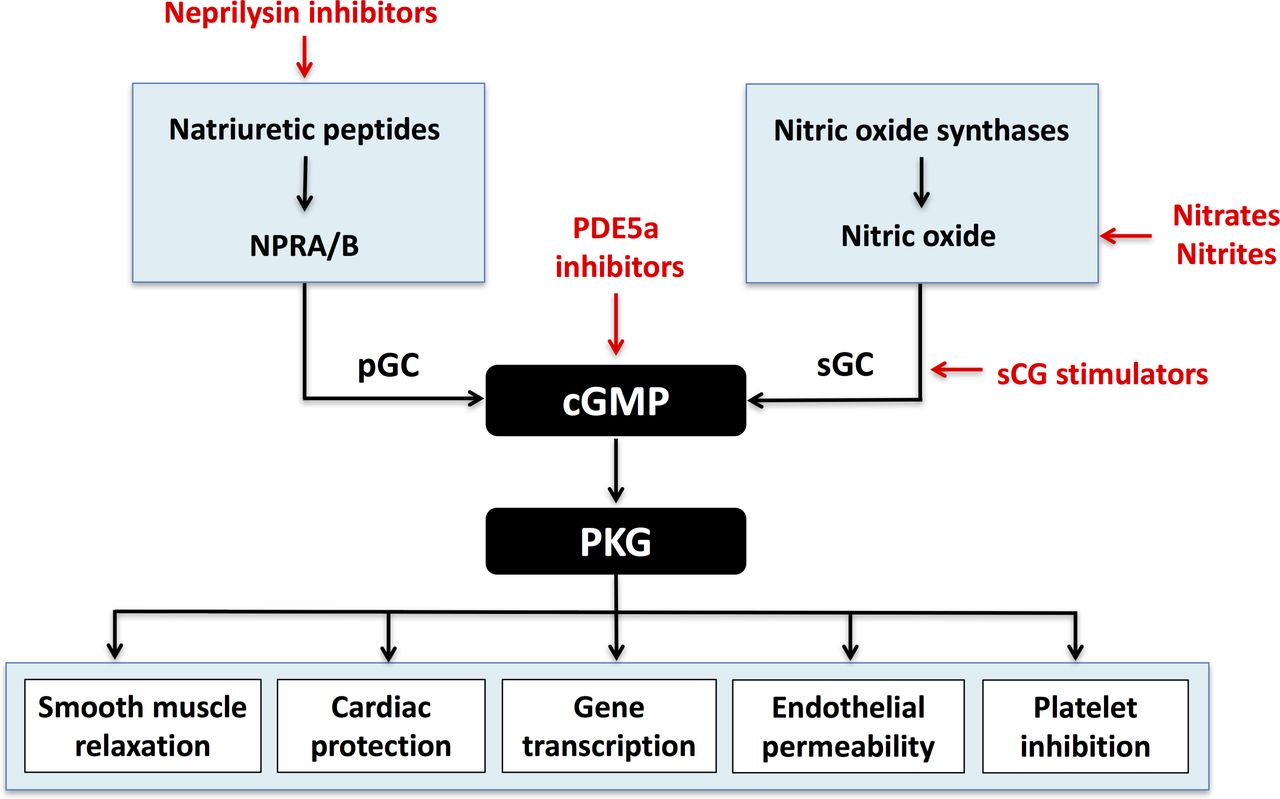
Pharmacological modulation of the NO-cGMP-PKG signalling pathway may increase cGMP content and reduce myocardial stiffness in HFpEF (Figure 3). To date, neither direct replenishment of cGMP, via soluble guanylate cylase stimulators (riociguat,31 vericiguat32), nor indirect cGMP replenishment via the organic NO donor, isosorbide mononitrate33 (ISMN), have met their primary endpoints in HFpEF trials. ISMN reduced patient activity levels in the Nitrate’s Effect on Activity Tolerance in Heart Failure with Preserved Ejection Fraction (NEAT-HFpEF) trial, possibly due to excess hypotension or renal sodium retention,33 and is therefore contraindicated in HFpEF unless required for another indication, for example, angina.4 Inorganic nitrate preferentially delivers NO during hypoxia and acidosis, as occur during stress and exercise, potentially avoiding hypotensive sequelae. In a phase II study, beetroot juice (dietary inorganic nitrate) improved systemic vasodilation during exercise and submaximal exercise endurance in patients with HFpEF.34 Further studies using an inhaled nitrite preparation are in progress (NCT02742129).
{kind=link}
{kind=link}
{kind=link}
Myocardial cyclic guanosine monophosphate (cGMP) signalling in HFpEF (potential therapeutic targets are highlighted in red). Natriuretic peptides bind to the natriuretic peptide receptors A and B (NPRA/B) and stimulate cGMP via particulate guanylate cyclase (pGC). Neprilysin inhibitors act through this pathway. Nitric oxide synthases produce nitric oxide which stimulates cGMP via soluble guanylate cyclase (sCG). sCG stimulators and nitrates/nitrites target this pathway. cGMP activates protein kinase G (PKG) which has a number of beneficial effects (as demonstrated). Phosphodiesterase-5a inhibitors (PDE5a) act directly on this pathway by preventing the breakdown of cGMP.
Natriuretic peptides increase intracellular cGMP (Figure 3). Neprilysin inhibitors prevent the breakdown of biologically active natriuretic peptides. In the phase II PARAMOUNT trial, the combined neprilysin inhibitor/angiotensin receptor blocker, sacubitril–valsartan, was associated with lower NT-proBNP, reduced left atrial size and a trend towards improved functional class compared with valsartan therapy alone,35 implying a disease-modifying effect in HFpEF. A phase III trial with the combined primary endpoint of cardiovascular death or first HF hospitalisation is underway (PARAGON-HF, NCT01920711). The impact of sacubitril–valsartan, compared with individualised medical management of comorbidities, on NT-proBNP, symptoms, exercise capacity and safety in HFpEF is also being studied (NCT03066804).
Therapies to improve exercise intolerance and functional adaptations
It is debatable whether exercise intolerance in HFpEF is predominantly due to impaired cardiac, chronotropic21 or peripheral vascular reserve.36 Theoretically, greater LV filling occurs at lower heart rates, although excess rate lowering may exacerbate chronotropic incompetence in HFpEF. The If current blocker, ivabradine, variably demonstrated improved,37 worsened38 or no effect39 on exercise capacity, quality of life and BNP in phase II HFpEF trials. RAPID-HF will assess whether restoring chronotropic competence using rate adaptive pacing can improve exercise capacity in patients with HFpEF in sinus rhythm who display chronotropic incompetence (NCT02145351).
Pulmonary vasodilation may improve pulmonary hypertension in HFpEF. A number of agents are currently being tested, including oral trepostinil (NCT03037580, NCT03043651), riociguat (NCT02744339) and nitrate therapy (NCT02980068). BEAT-HFpEF (NCT02885636) is investigating whether albuterol improves pulmonary vascular tone in HFpEF.
Therapies to ameliorate advanced symptoms
Creation of a controlled left-to-right interatrial shunt in patients with advanced HFpEF, improved functional capacity and quality of life after 12 months in an open-label study of 64 patients.40 Open-label phase 1 studies are underway for similar devices (CORolla, NCT02499601; Occlutech atrial flow regulator, NCT03030274). A small sham-controlled RCT is due to report shortly (REDUCE LAP-HF I; NCT 02600234).
Monitoring strategies to prevent adverse outcomes
Outcomes from disease management programmes have not been reported stratified by HF type,41 though feasibility of implementing a specialised HFpEF programme has been described in a single centre.42
Following the favourable results of the CHAMPION trial,43 which included patients with a spectrum of EFs, additional prospective studies of remote pulmonary artery pressure monitoring are underway in the USA and Europe/Australia.
Treatment of comorbidities and exercise training
OPTIMIZE-HFpEF (NCT02425371) will determine whether systematic screening and targeted management of comorbidities in HFpEF patients (>60 years of age) will improve a composite outcome comprising symptoms, NT-proBNP, diuretic use, HF hospitalisation and death compared with usual care. The safety, tolerability and efficacy of iron repletion, in the presence or absence of anaemia, on walking distance after 1 year are being investigated in FAIR-HFpEF (NCT03074591).
To date, exercise training represents the only intervention that has demonstrated symptomatic benefit in relatively young patients with HFpEF, likely through beneficial effects on peripheral (arterial and skeletal muscle) targets.44 The exercise protocol employed in early studies may not be feasible in all elderly or frail patients with HFpEF; thus, further studies to refine the content of exercise programmes (Exercise Intolerance in Elderly Patients With HFpEF, NCT02636439), define the mechanism of benefit (Resistance training in HFpEF, NCT02435667) and optimal location of exercise (Implementation of Telerehabilitation In Support of HOme-based Physical Exercise for Heart Failure, NCT02435667) are underway.
Future directions
Definition of HFpEF and its fundamental mechanisms
The lack of consistent diagnostic criteria for HFpEF makes comparison across randomised trials difficult. There is a pressing need to improve the specificity of an HFpEF diagnosis from other HF syndromes and comorbid disease states, such as symptomatic CAD and AF. Novel diagnostics, including multiparametric biomarkers and new imaging techniques, may help to identify unique biological signature(s) for HFpEF (eg, circulating galectin-3 and MRI-T1 mapping techniques may be used to quantify myocardial fibrosis).
Fundamental and specific changes in myocardial structure and function in patients with HFpEF support the ongoing search for mechanistically targeted therapies.15 Few insights are available from the extreme ends of the HFpEF spectrum; thus, identification of key predictors and drivers of HFpEF from at-risk populations with comorbid disease (eg, diabetes, hypertension, AF), as well as better description of the trajectory/ies of HFpEF, including mode of death and cardiovascular events, may lead to identification of pivotal mechanisms and new therapeutic targets. Albeit in the context of a typically elderly population where non-cardiovascular events may also critically determine clinical outcomes.
Validation of HFpEF subphenotypes
Characterisation of HFpEF subphenotypes will provide greatest value if categories can be replicated across populations, clearly distinguished from ‘non-HFpEF’ and linked to unique mechanisms of disease. This will be a starting point for prospective comparative studies. Collection of high-dimensional data from large numbers of patients, with and without HFpEF, should facilitate these aims, provided this is matched to accurate coding practices. Integration of data collection into routine clinical workflow may minimise missing variables and enable correlation with nuanced clinical assessment. One such initiative is being conducted in patients with pulmonary vascular disease, including left-sided heart disease-related pulmonary hypertension, in the multicentre NHLBI-sponsored PVDOMICS network (NCT02980887).
Unfortunately, low availability of myocardial tissue from patients with HFpEF hinders translational research in this field. More broadly representative animal models (beyond hypertension-related remodelling) may identify novel disease mechanisms. The extent to which ‘deep’ phenotyping of HFpEF will advance the field will depend on the demonstration of biological relevance and incremental therapeutic or prognostic value.
Clinical trial design considerations and novel therapeutic strategies
Enrolment in HFpEF treatment trials is challenging. Patients who are very elderly, frail, obese or have a high comorbidity burden are often underrepresented, which limits the generalisability of trial findings and their relevance to clinical practice. Validation of simplified diagnostic algorithms is urgently required, as well as identification of the key clinical or biological characteristics that influence outcome. Invasive stress testing can be very useful but may not be feasible for all centres.
New trial designs may be useful in HFpEF, and this requires discussion between trialists, regulators and reimbursement authorities. Adaptive design features allow flexibility based on interim analysis, and thus may improve the value and efficiency of clinical trials. Such a strategy may have altered the outcome of the TOPCAT trial.28 Flexible trial protocols may also accelerate incorporation of emerging science: for example, enrolment criteria for PARAGON stipulated BNP elevation, though recent data suggest that neprilysin inhibition may preferentially benefit patients with a low BNP.45 Patient-reported outcome measures (symptom burden, quality of life) and non-cardiovascular sequelae associated with HFpEF (eg, sarcopaenia, renal failure) should also feature more prominently among primary or secondary endpoints of clinical trials. The feasibility of a patient-centric endpoint was demonstrated in NEAT-HFpEF,33 and there are signs that regulators are more willing to consider such endpoints in areas of unmet need.46
Ultimately, a single therapy or therapeutic approach may not be effective for all patients with HFpEF. Complex (combined) interventions or therapeutic programmes incorporating exercise and lifestyle modification, including weight loss, should be evaluated and have been beneficial in small trials.44 47 The current focus on cardiovascular-targeted therapies is also unlikely to reduce the burden of non-cardiovascular deaths in HFpEF. Therefore, evidence from randomised trials to guide the management of comorbidities in HFpEF remains vital, and may provide relevant information for primary prevention.48
Conclusion
HFpEF is an evolving concept that, as yet, has failed to translate into meaningful improvement in the outcome of individuals with HF symptoms but no overt reduction in LV systolic function or primary valve disease. The syndrome(s) is/are multifaceted and debilitating, and the prevalence is likely to increase steeply in the coming decades. Several emerging diagnostic and treatment strategies appear promising but require validation. Currently, those writing clinical guidelines have little high-quality evidence on which to base advice for clinicians and their patients. In the future, it is likely that the syndrome will be disaggregated into different phenotypes, where different therapeutic approaches may be appropriate. Certainly however our current knowledge base is inadequate to the task of managing this increasing clinical problem.49–51
References
Footnotes
Contributors RZ and MRC drafted and revised the manuscript.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.