Article Text

Abstract
Objective: To study trends in the use of lipid lowering drugs in the UK, and to assess which patient factors influence prescribing.
Methods: Routinely collected computerised medical data were analysed from 142 general practices across England and Wales that provide data for the Doctors’ Independent Network database. Subjects included were people aged 35 years or more with treated ischaemic heart disease, averaging annually over 30 000. The temporal trend from 1994 to 2001 in prescription of lipid lowering drugs and daily statin dose and the odds ratios (ORs) for receiving a statin prescription in 1998 were examined.
Results: Lipid lowering drug prescribing increased greatly over time, entirely because of statins, so that in 2001 56.3% of men and 41.1% of women with ischaemic heart disease received lipid lowering drugs. However, 33% of these patients were on a < 20 mg simvastatin daily equivalent. In 1998 the OR for receiving a statin fell from 1 at age 55–64 to 0.64 at 65–74 and 0.16 at 75–84 years. The age effect was similar in those without major comorbidity. Revascularised patients were much more likely to receive a statin than those with angina (OR 3.92, 95% confidence interval (CI) 3.57 to 4.31). Men were more likely to receive a statin than women (OR 1.62, 95% CI 1.54 to 1.71) but this difference disappeared after adjustment for age and severity of disease (OR 1.06). Geographical region had little effect but there was a very weak socioeconomic gradient.
Conclusions: Although prescribing has increased, many patients who may benefit from lipid lowering drugs either do not receive it or are undertreated, possibly because of lack of awareness of the relative potency of the different statins. Patients with angina and the elderly are less likely to receive treatment that may prevent a coronary event.
- lipid lowering drugs
- statins
- prescribing patterns
- patient factors
- ACORN, a classification of residential neighbourhoods
- CHD, coronary heart disease
- DIN, Doctors’ Independent Network
- GPRD, General Practice Research Database
- IHD, ischaemic heart disease
- KHS, key health statistics
- MI, myocardial infarction
Statistics from Altmetric.com
- ACORN, a classification of residential neighbourhoods
- CHD, coronary heart disease
- DIN, Doctors’ Independent Network
- GPRD, General Practice Research Database
- IHD, ischaemic heart disease
- KHS, key health statistics
- MI, myocardial infarction
The effectiveness of the hydroxymethyl glutaryl coenzyme A reductase inhibitors (statins) in secondary prevention of ischaemic heart disease (IHD) is well established.1,2 Such secondary prevention is a public health priority.3 Statins have become by far the most widely prescribed lipid lowering drugs4 and yet there is evidence that many patients who may benefit from them are not receiving these drugs. In 1998 fewer than a third of patients with IHD in England were receiving lipid lowering drugs.5 Another recent study reported that use of lipid lowering drugs in patients with IHD remained low and that even among patients receiving them, fewer than half had a total cholesterol concentration below 5.0 mmol/l.6 It has been suggested that sex strongly influences lipid lowering drug prescribing and other secondary prevention measures,7 with 31% of men but only 21% of women in the survey being prescribed such drugs. However, a recent study found older age to be the most important association with lower statin use.8
We used the Doctors’ Independent Network (DIN) database to determine trends in statin prescribing, including dosage, over time and to examine to what degree patient factors and practice affect any inequalities in the prescription of these drugs.
METHODS
The DIN database
The DIN database contains routinely collected anonymised patient records from general practitioners using Torex System 5 practice software. It has been used for epidemiological research9 but to date its main use has been for pharmaceutical market research. About 300 practices and 1400 general practitioners have contributed data, of which we have selected 142 practices on a series of quality indicators including completeness of data recording, linkage of records to prescriptions issued, and duration of data provision. We have processed the registers in these practices to remove patients who remain registered with the practice after they have left the practice or died and to ensure that the distribution of age groups within these practices corresponds well with nationally available data and with the age distribution of patients within the General Practice Research Database (GPRD). Over one million patient years of information are available in DIN annually.
General practitioners in DIN are encouraged to enter all surgery contacts with patients onto their clinical system. Diagnoses, procedures, and investigations are recorded using four-character Read codes, as are all prescriptions. A unique aspect of DIN is that it contains an indicator of social circumstance allocated to patients at the post code level. This is the ACORN index (a classification of residential neighbourhoods), a commercially available geodemographic segmentation system.10 It provides many levels of detail but at its most aggregated level categorises residential neighbourhoods into six groups along a dimension from “thriving” to “striving”. ACORN has been used in research as an indicator of deprivation.11,12 In DIN, the ACORN score is attached to records by the practice computer before anonymisation and data extraction. For technical reasons not all practices or patients in DIN have an ACORN score assigned.
Patient selection
For the years 1994 to 2001 we selected patients aged 35 years or more who were registered with practices on 31 December of that year and who had been registered for at least six months before this date. In doing this we followed the methods used by the compilers of key health statistics (KHS).13 We similarly used the KHS definition of “treated IHD”, this being the presence of a coded entry for IHD anywhere in the records before 31 December plus a prescription for any cardiovascular system drug (British National Formulary, chapter 2) or aspirin in the year of interest.
For these IHD patients, we extracted data on age, sex, registered practice, National Health Service region, smoking status, ACORN score (if present), type of IHD, time from diagnosis, and prescription information. Type of IHD was divided into non-specific IHD Read codes, angina, any myocardial infarction (MI), and revascularisation (any coronary artery revascularisation procedure). Each patient could have only one IHD type, and the most clinically significant diagnosis in each record was chosen, revascularisation being most and non-specific IHD being least significant. For patients who had been prescribed statins, we extracted the type of statin, strength, and dose frequency and used this information to calculate the daily dose in milligrams. From this we derived an approximate equivalent daily dose of simvastatin. This takes into account the different potencies per milligram of the various statins and presents them as an equivalent dose of the most widely used statin.14
To investigate whether any age trends were attributable to increasing levels of comorbidity and prescribing we repeated our analyses of 1998 data restricted to patients with IHD but without a diagnosis of stroke, cancer, mental disorder, or heart failure. We further restricted our analyses to those not receiving a prescription for any other British National Formulary chapter.
Analysis
We examined prevalence of recorded IHD, percentage of IHD patients receiving lipid lowering drugs, and daily dose of statins (where prescribed) annually from 1994 to 2001. For the principal analysis the main outcome variable was prescription of lipid lowering drugs in 1998. This was the year the most recent KHS were published,13 although results were similar for more recent years. Odds ratios (ORs) were derived from logistic regressions to determine the influence of the predictor variables on this outcome. Analyses of variation between the 142 practices in prescribing rates in 1998 were based on analyses of variance with practice as the unit of analysis.
We wished to validate both IHD rates and the proportion of patients with IHD who were prescribed statins against KHS data from the GPRD. Because there are clear regional variations in IHD rates and because of differences in the regional distribution of the two databases (60% of DIN practices are in the south of England compared with 42% of GPRD practices), we used direct standardisation to the GPRD regional structure to derive DIN prevalence rates for treated IHD for comparison with KHS rates.
RESULTS
Prevalence of IHD and lipid lowering drug prescription
Prevalence of treated IHD rose from 6.4% to 7.7% between 1994 and 2001, reflecting both the aging of the population and increasing levels of treatment. Much more pronounced was the rise in lipid lowering drug prescribing among patients with IHD (fig 1 and table w1). The increase in prescribing, nearly all accounted for by prescriptions for statins, is striking, but in 2001 only 56.3% of men and 41.1% of women with IHD received a prescription for lipid lowering drugs. Secular trends in statin prescribing rose steadily in all age groups and separately for those with angina, MI, and those undergoing surgery (table w2), though differentials by age and type of IHD are apparent in all years. The number of patients not currently on any lipid lowering drugs but with a prescription for a statin in a previous year was low (fig 1).

Trends in statin prescription in patients with ischaemic heart disease (IHD) by sex. LLT, lipid lowering treatment.
Statin dose
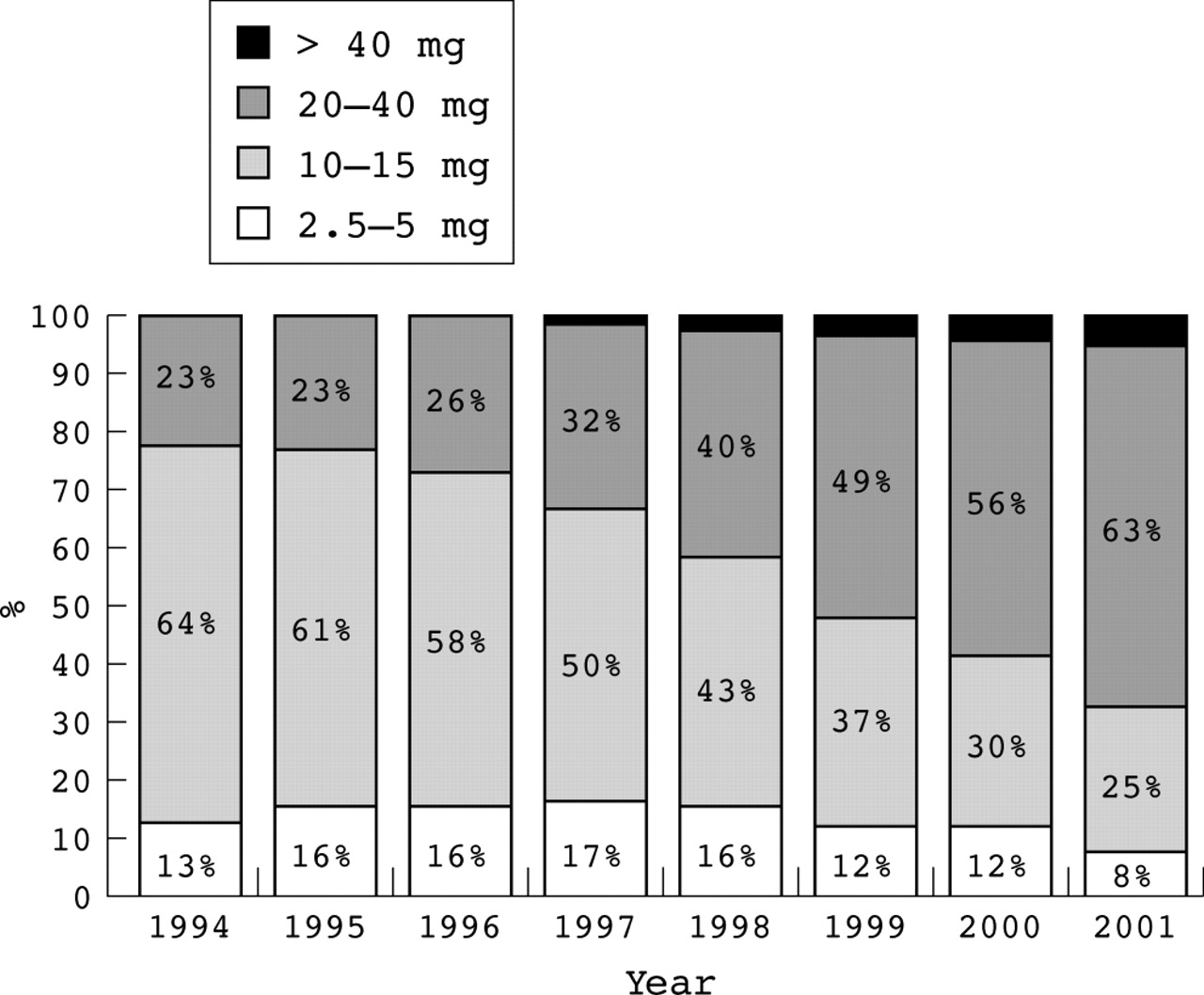
Figure 2 shows the trend in daily dose, adjusted to milligram equivalence with simvastatin, among those prescribed a statin. If a 20 mg daily dose of simvastatin is taken as the amount required to achieve a mean reduction of 25% in total cholesterol1,14 then in 1994 only 22.6% of men and 21.9% of women were given a statin dose likely to achieve this reduction. By 2001 this had risen to 67.6% of men and 67.4% of women. Of those taking a 2.5–5 mg/day equivalent dose (8.1% of men and 7.4% of women in 2001) most were taking lower doses of the less potent statins, pravastatin and fluvastatin (and cerivastatin, now withdrawn in the UK).

Trends in statin doses (equivalent daily doses of simvastatin). Simvastatin 20 mg is required to achieve a mean reduction of 25% in total cholesterol.
Factors influencing statin use in 1998
Age had the strongest association with statin prescription, with 44.9% of patients aged 35–64 years receiving a statin compared with just 10.4% of those aged 75–84 and only 1.2% of those aged over 85. Further analysis was restricted to ages 35–85 (table 1). Type of IHD was also strongly related: revascularised patients had an OR of 3.92 for receiving a statin compared with patients with angina, after adjustment for other factors.
Factors influencing statin usage among IHD diagnosed patients aged 35–84 in 1998 (n = 30 448)
Statin use decreased in a graded fashion with time from diagnosis, from 39.6% for those with a diagnosis in the previous year to 20.3% of those given a diagnosis more than five years previously (OR 2.19 after adjustment). Smokers were slightly less likely to receive statins. There was a weak but significant trend of decreasing statin treatment with increasing ACORN score. Thus, patients in “striving” areas were less likely to receive a statin than in “thriving” areas. Although there was significant regional heterogeneity, there was no evidence of any north–south trend or other geographical patterning.
Men were more likely to receive a statin than women (OR 1.62); however, adjustment for confounding variables effectively removed this difference (OR 1.06). This was because women with IHD were older, more likely to have an angina diagnosis than men (63.1% v 42.1%), and less likely to have been revascularised (3.8% v 12.5%). Further analyses showed that while among patients with angina, men were more likely to receive statins than women even after adjustment (OR 1.33, 95% confidence interval 1.18 to 1.49), among revascularised patients men were less likely than women to receive a statin after adjustment for other factors (OR 0.60, 95% confidence interval 0.48 to 0.76).
There was a wide variation in prescribing patterns between practices (fig 3) that lessened only slightly when age adjusted rates were used instead (data not shown). In 1998, the prescribing rates among those aged 35–85 ranged from 12–51% (interquartile range 25–33%), but in 2000 it was 23–69% (interquartile range 40–52%). In 1998 statin prescribing rates were unrelated to practice size (p = 0.63), being 29% in the 12 practices with under 3000 and 27% in the 8 practices with over 12 000 patients. Nor was statin prescribing associated with degree of urbanisation (9 inner city practices average 28%, 107 urban practices 27%, and 26 rural practices 27%; p = 0.79)

{kind=link}
{kind=link}
{kind=link}
Statin use among patients aged 35–84 years in whom IHD is diagnosed by practice in 1998 (n = 142) and 2000 (n = 115).
To investigate the age trend further we examined statin prescribing among patients with IHD but without any diagnosis of stroke, mental disorder, cancer, or heart failure. At all ages the percentage of these “healthy” patients prescribed statins was only slightly higher than for all patients and the same age gradient was apparent, ranging from 45% (90 of 202) at age 35–44, through 54% (611 of 1139) at age 45–54, 45% (1307 of 2870) at age 55–64, 34% (1680 of 4949) at age 65–74, 12% (402 of 3427) at age 75–84, and 2% (14 of 880) over age 85 years. Further restriction based on numbers of drugs prescribed also made little difference to the trend (data not presented).
Analyses of factors influencing prescribing in 2000 and 2001 provided very similar findings to those for 1998 but with wider confidence intervals (data not presented). In particular, there was no evidence that the age differences were diminishing with prescribing rates in 2001, being 66.5% (175 of 263) at 35–44, through 68.1% (988 of 1450) at age 45–54, 68.4% (2823 of 4130) at 55–64, 61.0% (4314 of 7075) at 65–74, 33.8% (2294 to 6797) at 75–84, and 5.3% (125 of 2382) over 85 years.
Validation of DIN against GPRD in 1998
Region adjusted prevalence rates of treated IHD in DIN were 7.29% for men and 5.37% for women, compared with GPRD published rates of 7.27% for men and 5.42 for women.13
In 1998 the percentage of patients aged ≥ 35 with IHD prescribed statins in DIN (31.4% of men and 20.0% of women) was very similar to the figures that can be derived from GPRD data (29% of men and 19% of women).13
DISCUSSION
IHD rates obtained from DIN are very similar to GPRD published rates, as are statin prescription rates, providing external validation of the trends in IHD and statin prevalence obtained from DIN. No data from GPRD have been published since 1998.
Lipid lowering drug prescription for patients with IHD has grown greatly since 1994 and continues to increase. Statins account for almost all of this growth. Despite this, many patients who may benefit from this treatment still do not receive it.
The trend in statin daily doses had been towards the higher doses more likely to produce the 20–25% reductions in total cholesterol concentration suggested by guidelines3 but many patients remain on lower doses. Many such patients were on low to medium doses of the less potent statins and probably would have benefited from a higher dose or a change to a more potent statin. These data fit with the recent study by Whincup and colleagues.6
Examining the secular trends in our data (table w1) it is apparent that the increase in prescribing of statins for secondary prevention of IHD has been steady with no obvious impact of the national guidelines issued in 199715 and 1998.16 Moreover, the secular increase is similar in all age groups and separately for those with angina, those with MI, and those undergoing surgery (table w2), though differentials by age and type of IHD are apparent in all years.
In implementation of any new guidance it is inevitable that some practices lead, while others lag behind. However, some years after dissemination of evidence regarding the effectiveness of statins, there remains wide variation between general practices in their prescription of statins for IHD. Only limited exploration of practice variation was possible with no evidence that either practice size or degree of urbanisation was related. In fact, practice variation is pronounced for almost any process measure in primary care. Attempts to explain this variation have met with only limited success. Thus, a study of practice variation in prescribing costs found that easily recorded practice factors such as age and sex of general practitioners and other practice characteristics such as computerisation and staff structure explained little.17 It seems likely that to understand practice (and individual doctor) variation a qualitatively different type of study that will collect data on attitudes and responses of individual doctors will be necessary.18 At the same time, where targets have been introduced into primary care with clear incentives for reaching them, practice variation has greatly reduced. Such an example is cervical cytology screening. It is too early to assess the impact of the National Service Framework for coronary heart disease (CHD) on reducing practice variation in statin prescribing.
An important strength of the present study is that practice differences were controlled for when assessing the role of other factors in statin prescribing. Of the other factors that may influence the decision to prescribe a statin, the type of IHD and the age of the patient appear to be most important. It may be that doctors regard IHD in younger people as more serious than in older people. However, since 1999 there has been clear trial evidence that patients aged 65–74 benefit as much as younger patients in relative terms, while the absolute risk reduction is probably greater.19 The logical presumption was that similar benefits would be seen at older ages. This has recently been confirmed by the MRC/BHF heart protection study,20 which has shown clear benefit in those aged 70–80 years at randomisation. Unfortunately, “agist” patient selection in the earlier published trials is reinforced by the National Service Framework for CHD, which does not specifically mention the need for statin treatment over age 75,3 and the National Service Framework for older people, which simply refers one to the framework for CHD.21
It may also be that doctors perceive coronary artery procedures as being more significant than angina. However, the higher statin prescribing rate among patients with MI and coronary artery bypass graft more probably reflects treatment being initiated in a secondary care setting. As the purpose of lipid lowering drugs in IHD is secondary prevention, it is clearly just as important that patients with angina receive lipid lowering drugs as revascularised patients.
Lack of a regional pattern for statin treatment is in keeping with other data on the lack of variation in treatment and control of hypertension22 and can be seen as a strength of a universally available National Health Service. In an earlier report based on the Health Survey for England8 we examined a broad range of socioeconomic factors and found no clear association, though manual workers were slightly more likely to be taking statins for secondary prevention of CHD. The weak association with social status as assessed by the ACORN score in the present study is consistent with the earlier report and shows the advantage of a large sample size. Taken together it seems unlikely that social factors have an important role in determining who receives statins. The slightly lower rate for smokers confirms an earlier report,8 is in keeping with smokers being less likely to have their blood pressure treated or controlled,22 and may be explained by smokers being less likely to visit their general practitioner.
Our observations appear to elucidate the finding of Hippisley-Cox and colleagues7 that women are less likely to receive lipid lowering drugs than men. Our data may also explain some of their other observed sex inequalities in IHD secondary prevention. In our study women with IHD were much less likely to have had revascularisation and were on average considerably older. However, among patients who were revascularised, women were more likely than men to be taking a statin. It has been noted that women with IHD are less likely to be investigated and to receive revascularisation23 but the reasons for this are not known. Our data confirm and extend the observations of Reid and colleagues8 and suggest that the reasons for the sex differences in IHD secondary prevention measures may be more subtle than sex prejudice.24,25
Our study has the strength that all patients registered with a practice were included. Thus, non-response bias is not an issue and the large numbers of patients and practices provide ample statistical power and generaliseability. The potential weakness lies in selection of the practices. For example, it may be that statin prescribing in DIN practices is higher because of their interest in research. However, a recent paper26 provides some reassurance that research practices do not differ much in patient outcome and in this instance our main findings on patient characteristics were robust to controlling for practice and consistent with our recent analysis of Health Survey for England data.8
Our observations show that clinical practice in the area of lipid lowering has improved steadily over the past five years but that there is room for further improvement in a number of areas. In particular the low rates of prescribing among patients with angina only and in those over age 65 appear illogical. While the National Service Framework will probably lead to improvements in prescribing for angina patients, the elderly may continue to miss out on the benefits of statins unless clearer guidance is given.
Acknowledgments
We are grateful to Steve Caine of CompuFile Limited for his technical assistance with DIN and for much helpful support. We acknowledge with gratitude the general practitioners who provide data for DIN and the DIN board for their continued support. SdeW and IMC are funded by The Wellcome Trust.
REFERENCES
Supplementary materials
Footnotes
-
↵* Also the Department of Public Health Sciences
-
Conflicts of interest: NR is a director of CompuFile Ltd, which markets data to pharmaceutical companies.
Linked Articles
- Miscellanea