Article Text

Abstract
Objective: To assess health related quality of life of patients with congestive heart failure; to compare their quality of life with the previously characterised general population and in those with other chronic diseases; and to correlate the different aspects of quality of life with relevant somatic variables.
Setting: University hospital.
Patients and design: A German version of the generic quality of life measure (SF-36) containing eight dimensions was administered to 205 patients with congestive heart failure and systolic dysfunction. Cardiopulmonary evaluation included assessment of New York Heart Association (NYHA) functional class, left ventricular ejection fraction, peak oxygen uptake, and the distance covered during a standardised six minute walk test.
Results: Quality of life significantly decreased with NYHA functional class (linear trend: p < 0.0001). In NYHA class III, the scores of five of the eight quality of life domains were reduced to around one third of those in the general population. The pattern of reduction was different in patients with chronic hepatitis C and major depression, and similar in patients on chronic haemodialysis. Multiple regression analysis showed that only the NYHA functional class was consistently and closely associated with all quality of life scales. The six minute walk test and peak oxygen uptake added to the explanation of the variance in only one of the eight quality of life domains (physical functioning). Left ventricular ejection fraction, duration of disease, and age showed no clear association with quality of life.
Conclusions: In congestive heart failure, quality of life decreases as NYHA functional class worsens. Though NYHA functional class was the most dominant predictor among the somatic variables studied, the major determinants of reduced quality of life remain unknown.
- quality of life
- congestive heart failure
- cardiopulmonary capacity
- NYHA, New York Heart Association
- SF-36, 36 item short form health survey
Statistics from Altmetric.com
Traditional aims in the treatment of congestive heart failure are to relieve symptoms and to improve the prognosis. Another major goal of health care is to maximise function in everyday life and to achieve the highest level of quality of life within the specific limits imposed by the disease. Quality of life is a relatively new scientific measure to evaluate effectiveness of treatment strategies and the course of a disease.1–3 In congestive heart failure, several disease specific instruments—such as the Minnesota living with heart failure questionnaire4—have proved useful in clinical studies.5–11 Disadvantages of these specific measures are that they are difficult to compare across diseases and with controls in the general population. Because they are designed to measure specific aspects of a certain disease, unforeseen side effects of treatment might go undetected (for a detailed review see Guyatt12). Recently, quality of life was shown to be decreased in patients with congestive heart failure in comparison with the general population,13, 14 using the medical outcome study 36 item short form health survey (SF-36), a validated, reliable, and multidimensional generic measure of quality of life.15, 16 However, the few studies which have investigated the relation between quality of life and clinical variables (reflecting the severity of disease) achieved inconclusive results.17–19 Our major aims in the present study were therefore as follows: to assess the extent of the impairment of quality of life in patients with congestive heart failure in comparison with the general population; to compare specific aspects of alterations in quality of life in congestive heart failure with those in other chronic diseases; and to examine the extent to which health related quality of life is explained by various clinical indices, namely New York Heart Association (NYHA) functional class, peak oxygen uptake, the distance covered during a six minute walk test, and the left ventricular ejection fraction.
METHODS
Consecutive patients with stable congestive heart failure (NYHA class I–III) who were referred to the department of cardiology at the University of Heidelberg were assessed to determine their eligibility to participate in the study. The inclusion criterion was a left ventricular ejection fraction below 45%, as determined by radionuclide ventriculography. Patients in NYHA functional class IV were excluded, as were those who had neurological, orthopaedic, peripheral vascular, or severe pulmonary diseases which could impair the successful completion of submaximal or maximal exercise tests. Patients who were not able to speak fluent German were also excluded.
The study was approved by the institutional ethics committee and all patients gave their written informed consent before enrolment.
Standard medical treatment (for example, with angiotensin converting enzyme inhibitors, digoxin, and diuretics) was individually optimised, based on symptoms and renal function, at least six weeks before exercise testing.
In all patients, the NYHA functional class was determined by an independent investigator before assessment of peak oxygen uptake, the six minute walk test, and measurement of left ventricular ejection fraction, and before the SF-36 was administered. All variables were collected within a 48 hour period.
Of the 239 patients who met the predetermined study criteria, 23 refused to participate or discontinued their participation, and 11 failed to complete the SF-36. Complete datasets of 205 patients were thus available for statistical analysis.
Baseline assessment
Each patient's history, clinical status, sociodemographic variables, and the aetiology and duration of the heart failure were assessed. Equilibrium radionuclide ventriculography was performed with a multicrystal gamma camera (Orbiter; Siemens, Erlangen, Germany) in the left anterior oblique view to determine the left ventricular ejection fraction (for details see Zugck20). Cardiopulmonary exercise testing was used to determine the functional capacity of the subjects. Equipment included a metabolic cart (Oxycon Alpha; Jaeger, Würzburg, Germany), with an interfaced supine positioned bicycle ergometer (Ergoline; Jaeger). Peak oxygen uptake was defined as the maximum oxygen consumption measured during the last 30 seconds of symptom limited exercise (for details, see Zugck20). Submaximal exercise capacity was evaluated with the six minute walk test21 within 24 hours, and at least four hours before cardiopulmonary exercise (for details, see Zugck20).
Quality of life assessment
Patients' self assessment of health related quality of life was measured by the German version of the SF-36.22, 23 Evaluation of the SF-36 was done by an investigator who was blinded to the somatic variables. In brief, the SF-36 is a generic health survey designed to assess aspects of health that are not disease, treatment, or age specific. The SF-36 is a generic multidimensional instrument consisting of eight multi-item components representing physical functioning (PF; the extent to which health limits physical activities, such as self care, walking, climbing stairs), role functioning physical (RP; the extent to which physical health interferes with work or other daily activities); bodily pain (BP; the intensity of pain and the effect of pain on normal work, both inside and outside the home); general health perceptions (GH; personal evaluations of current health, health outlook, and resistance to illness); vitality (VT; feeling full of energy rather than tired and worn out); social functioning (SF; the extent to which physical health or emotional problems interfere with normal social activities); role functioning emotional (RE; the extent to which emotional problems interfere with work or daily activities); and mental health (MH; general mental health including depression, anxiety, behavioural-emotional control, and general positive affect). SF-36 scores were converted to a scale of 0 to 100, a higher score indicating a better quality of life.
Comparison groups
The data on the congestive heart failure sample were compared with data on the general population23 and with those in patients with other chronic diseases, namely chronic hepatitis C infection,24 chronic haemodialysis,25 and major depression.26
Statistical analysis
For independent group comparisons, we used t statistics with Satterthwaite correction for variance inhomogeneity. Stratifying the current congestive heart failure sample according to NYHA functional classes I, II, and III led to designated groups a, b, and c. The total heart failure sample served as designated group d. The designated groups a, b, c, and d were compared with the healthy reference group (one sided t tests) and with three selected disease comparison groups (two sided t tests). In addition, the designated groups a, b, and c were compared with each other (one sided tests). Because comparisons with the disease groups were performed for each NYHA level and the total heart failure sample across eight scales, the conservative Bonferroni correction of probability values was performed (that is, the nominal α niveau was adjusted at 0.05/32 = 0.00156).
As a measure of association, Spearman rank correlation coefficients were computed between NYHA functional class, peak oxygen uptake, six minute walk test, left ventricular ejection fraction, duration of congestive heart failure, age, and the scores of the SF-36 scales.
To assess possible influences of functional variables on quality of life, patients were divided into subgroups by the following commonly used cut off values20: peak oxygen uptake > or ≤ 14 ml/min/kg; six minute walk test > or ≤ 450 m; left ventricular ejection fraction > or ≤ 20%. This approach was chosen because the explicit testing of median splits of the current sample showed similar results—that is, peak oxygen uptake 14.6 ml/min/kg, six minute walk test 485 m, and left ventricular ejection fraction 21%.
Multiple regression analysis was performed to determine the variance of dependent variables (the eight SF-36 scales) explained by independent variables (NYHA functional class, peak oxygen uptake, six minute walk test, left ventricular ejection fraction, duration of congestive heart failure, and age). The forward selection algorithm was used to determine the incremental contribution of each predictor in explaining variance in the quality of life. The limit for significant incremental explanation of variance was set at 5%.
RESULTS
Demographic data and functional variables in all the patients with congestive heart failure are summarised in table 1.
Characteristics of 205 patients with congestive heart failure
Most of the patients were male and retired or unemployed, despite the fact that their mean age was rather low, with 88.8% of the patients being younger than 65 years of age (range 19–74 years). The majority of the patients (88.2%) were in NYHA functional class II or III, and almost all were being treated with an angiotensin converting enzyme (ACE) inhibitor and a diuretic. The advanced stage of disease was also reflected by the fact that 46% of the patients had a peak oxygen uptake of ≤ 14 ml/min/kg, 38% a six minute walk test of ≤ 450 m, and 49% a left ventricular ejection fraction of ≤ 20%.
Comparison with a normal population
The total congestive heart failure sample was characterised by significantly reduced scores in all aspects of quality of life compared with a healthy reference group (fig 1; table 2). As illustrated in fig 2A, there was a gradual decline in SF-36 scores compared with the normal population (reference group) from NYHA class I to class III. Within NYHA class I, the most significant decreases were observed in the scales which primarily refer to somatic wellbeing and functioning. In higher NYHA classes, significant decreases in the scales measuring emotional wellbeing and functioning were also found (fig 2A). Patients in NYHA class III had roughly one third of the scores of the healthy population in the following short form scales: physical functioning, role functioning physical, bodily pain, general health, vitality, and role functioning emotional. NYHA class III patients reached a minimum mean SF-36 score in physical role functioning of only 10.7%, compared with 96.9% in the healthy population (fig 2A, table 2).
Comparison of SF-36 scales in heart failure patients in different functional classes, and between heart failure patients, patients with other diseases, and the general population
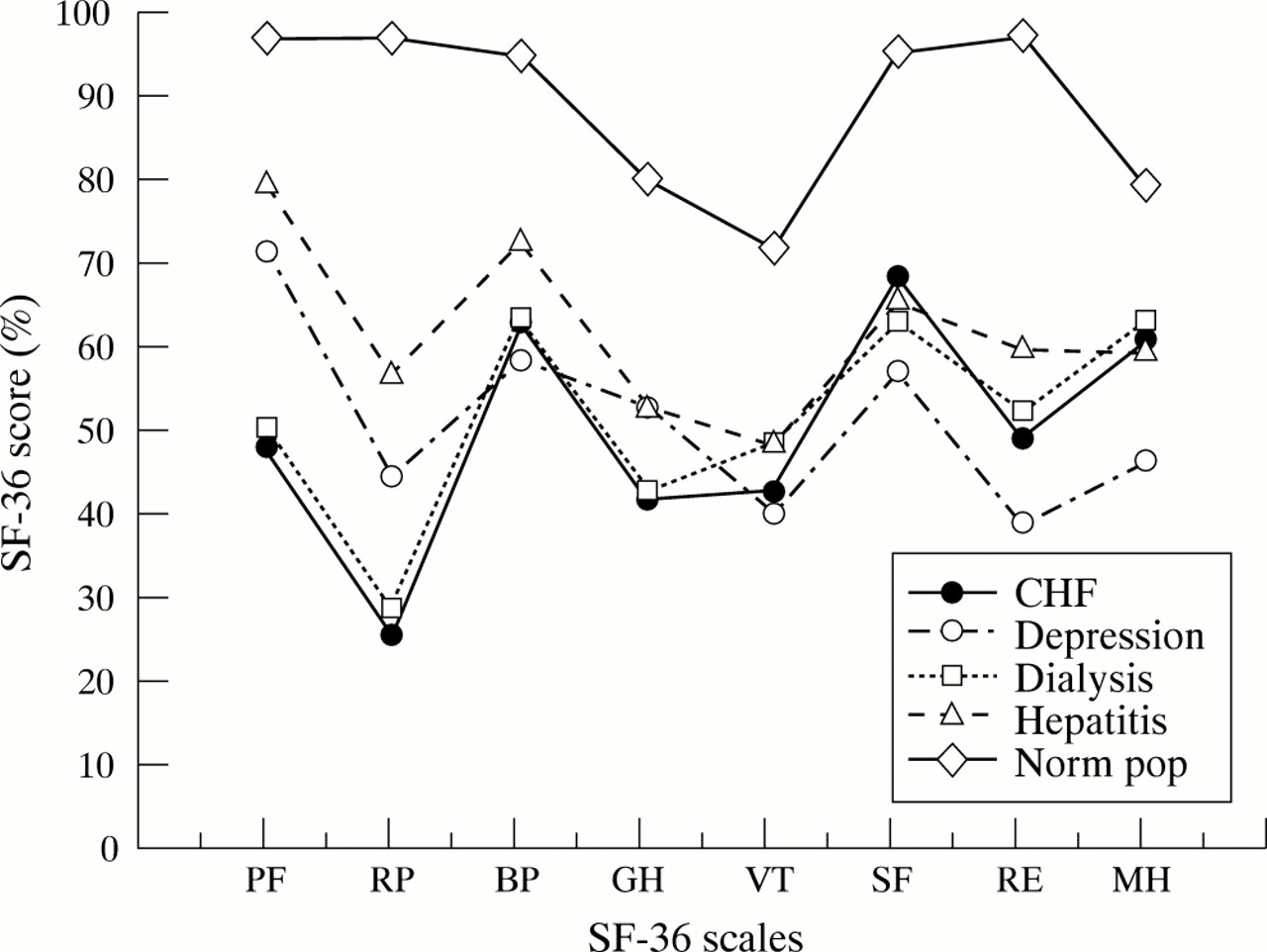
Comparison of total heart failure (CHF) sample with other diseases and with the normal population. SF-36 scores of the total CHF sample (n = 205; that is, not stratified by NYHA classification) compared with selected disease groups: patients on chronic haemodialysis (n = 120), patients with hepatitis C (n = 70), and patients with major depression (n = 502).23–25 The values for a normal population (Norm pop; n = 906) are also shown.22 The eight scales of the SF-36 short form health survey (SF-36) instrument are physical functioning (PF), role limitations due to physical limitations (RP), bodily pain (BP), general health perceptions (GH), vitality (VT), social functioning (SF), role limitations caused by emotional problems (RE), and mental health (MH).

{kind=link}
{kind=link}
SF-36 scores for patients with congestive heart failure (CHF) stratified into prognostically relevant subgroups according to somatic indices. (A) Stratification of the patients by New York Heart Association functional class (NYHA I, n = 24; NYHA II, n = 98; NYHA III, n = 83). (B) Patients split at a peak oxygen uptake of 14 ml/kg/min (≤ 14 ml/kg/min, n = 95; > 14 ml/kg/min, n = 110). (C) Patients split at a walking distance of 450 m covered during a six minute walk test (≤ 450 m: n =79; > 405 m, n = 126). (D) Patients split at a left ventricular ejection fraction (LVEF) of 20% (≤ 20%, n = 100; > 20%, n = 105). The respective values of a normal population (Norm pop, n = 906) are shown for comparison.22 The eight scales of the 36 item short form health survey (SF-36) instrument are physical functioning (PF), role limitations due to physical limitations (RP), bodily pain (BP), general health perceptions (GH), vitality (VT), social functioning (SF), role limitations due to emotional problems (RE), and mental health (MH). Peak Vo2, peak oxygen uptake; 6`WT, six minute walk test.
Comparison with chronic haemodialysis and with chronic hepatitis C
No significant differences were observed between the patients on chronic haemodialysis and the total heart failure sample (table 2). As shown in fig 1, the patients with congestive heart failure showed the same pattern of reduced quality of life as patients on chronic haemodialysis. In contrast, patients with chronic hepatitis C had higher scores in physical functioning, role functioning physical, and general health than the heart failure population (table 2). Thus the pattern of reduced quality of life in patients with chronic hepatitis C was significantly different from that in the heart failure sample (fig 1).
Comparison with major depression
In comparison with patients with major depression from the medical outcome study,26, 27 the total congestive heart failure sample was characterised by significantly worse physical health and better mental health (table 2). However, patients with more advanced congestive heart failure (NYHA class III) had similar scores to patients with major depression on the mental health scales (table 2).
Relation between peak oxygen uptake, six minute walk test, left ventricular ejection fraction, and quality of life
Subgroup analysis after splitting the total congestive heart failure sample at the prespecified values for the relevant prognostic indices (that is, at a peak oxygen uptake of 14 ml/min/kg and at a distance covered during a six minute walk test of 450 m) resulted in significant differences in all quality of life scales (figs 2B and 2C). In contrast, the degree of systolic dysfunction had no impact on the quality of life (fig 2D).
Spearman rank correlation coefficients between the SF-36 scales, functional variables, duration of congestive heart failure, and age are summarised in table 3. High degrees of correlation were found between the physical functioning dimension and NYHA functional class (r = −0.63), six minute walk test (r = 0.56), and peak oxygen uptake (r = 0.47). NYHA functional class and the six minute walk test correlated significantly with all short form dimensions. However, only some modestly significant correlations were obtained between the other functional variables and the SF-36 scales (correlation coefficients of between 0.23 and 0.47). None of the correlations between left ventricular ejection fraction and any of the SF 36 scales reached significance. The duration of disease and age had only very little impact on the SF-36 scales (table 3).
Univariate (rank correlations, r) and multivariate relations (multiple regression forward selection, R2) between SF-36 domains and other variables (n=205)
A series of stepwise forward multiple regressions was computed to explain the variance of each SF-36 scale by the independent variables NYHA functional class, peak oxygen uptake, six minute walk test, left ventricular ejection fraction, duration of disease, and age. Variability in short form scale physical functioning was explained by NYHA functional class (40%) and to a much lower degree by the six minute walk test (11%). In all other SF-36 scales, only between 10% and 28% of the variance could be explained by NYHA functional class, while none of the other variables contributed significantly (table 3).
DISCUSSION
Previous studies have shown an impairment in the quality of life in patients with congestive heart failure.13, 14 Our aim in the present study was to make a more detailed analysis of the relation between quality of life, the severity of the disease, and objective functional variables. Quality of life was assessed with a well validated questionnaire, the SF-36.15, 16 For determining maximal and submaximal functional capacity, standard methods were employed. In order to ensure accuracy, all data were collected within a 48 hour period in each patient.
Comparison with the general population
Compared with the healthy general population, the congestive heart failure sample showed a global reduction in quality of life in all the SF-36 scales. All indices of quality of life decreased with NYHA functional class, the most pronounced loss of quality of life being observed in the domains of physical functioning, role function physical, and role function emotional. In apparently asymptomatic patients with left ventricular dysfunction, independently classified as NYHA functional class I, the SF-36 revealed mild but significant decreases in the scales representing somatic aspects and vitality. In NYHA classes II and III all aspects of quality of life were dramatically reduced, reflecting the severe impact of congestive heart failure on daily life, even though the patients were in a compensated stage and in an ambulatory setting.
Comparison of the present study sample with a sample of patients with congestive heart failure of the medical outcome study26 revealed a similar pattern of impairment. However, as the latter did not include objective functional variables such as the six minute walk test and peak oxygen uptake, a comparison between the two samples can only be limited.
Comparison with other chronic diseases
A previous sample of patients on chronic haemodialysis25 showed nearly the same profile as the overall congestive heart failure sample in our present study. Thus it could be argued that all chronic disease conditions have a similar impact on quality of life. However, patients with chronic hepatitis C24 were characterised by quite a different pattern. In scales referring more to physical health, patients with chronic hepatitis C resembled patients with congestive heart failure in NYHA class I. However, in scales referring to mental health, hepatitis C patients were more comparable to NYHA class II patients.
As expected, patients with major depression were in a better physical condition than patients with congestive heart failure. Most interestingly, the patients with congestive heart failure in NYHA class III had a similar impairment of quality of life in the mental health domains as patients with major depression, in addition to their already dramatically reduced physical health. These data are in accord with the findings of some recent studies showing that a large proportion of patients with congestive heart failure suffer from depression.28–30 Thus the quality of life in patients in NYHA class III is reduced not only physically but also mentally.
One could speculate that these results reflect the effects of congestive heart failure on the central nervous system. Changes in central neurohumoral regulation systems or diminished central perfusion might impair cognitive capacity and trigger a latent vulnerability to depressive disorders.31
Relation of NYHA class, peak oxygen uptake, six minute walk test, left ventricular ejection fraction, and quality of life
In addition to NYHA functional class, more objective indices of functional capacity—such as peak oxygen uptake and the six minute walk test—also showed some relation to the quality of life. This contrasts with the report by Steptoe and colleagues,18 who found no univariate association between exercise capacity and quality of life in patients with mild to moderate congestive heart failure (predominantly in NYHA classes I and II); however, our present study included a broader spectrum of patients with congestive heart failure, with a large proportion in NYHA class III. Cardiopulmonary exercise testing and the six minute walk test represent different aspects of functional capacity, as only the latter—a submaximal exercise test—reflects the work load of daily activities.21 However, in accordance with the close relation between both these exercise tests,20 all SF-36 scales were related similarly to peak oxygen uptake and to the six minute walk test. In contrast, the left ventricular ejection fraction was not significantly correlated with any of the short form scales. Furthermore, there was no difference in health related quality of life in patients subgrouped according to their ejection fraction. This finding confirms the lack of relation between left ventricular ejection fraction and disease specific quality of life observed in other studies.32, 33
The findings of our present study may also explain why β blocker treatment in congestive heart failure has no consistent effect on the quality of life, despite a pronounced improvement in left ventricular ejection fraction (for review, see Carson34), whereas the increase in peak oxygen uptake achieved by exercise training is associated with an improvement in quality of life.35
In general, the variance in the short form scales that can be explained by factors such as NYHA functional class, peak oxygen uptake, six minute walk test, left ventricular ejection fraction, age, and the duration of disease was small. Only the variance of physical functioning was determined to a considerable degree (51%) by NYHA functional class and the six minute walk test. This confirms the validity of the physical functioning scale. In the other scales NYHA functional class and the six minute walk test also contributed consistently to the explained variance, although the effect was small (10–28%). On the one hand, the SF-36 seemed to differentiate clearly between different grades of severity of disease, as measured by the NYHA functional classification, the six minute walk test, and peak oxygen uptake; on the other hand, most of the variability in quality of life remained unexplained by the established indicators of the severity of congestive heart failure. This seems consistent with the findings of Wilson and colleagues,36 who showed little or no relation between perceived exercise intolerance—as measured by the Minnesota living with heart failure questionnaire—and objective measures of circulatory or ventilatory dysfunction.
These results raise the question as to which predictors besides the most obvious prognostic somatic variables influence the quality of life in congestive heart failure. According to Steptoe and colleagues,18 psychological adjustment may be a major determinant of quality of life. The influence of other variables on quality of life—such as neurohumoral factors and cytokines, which are known to be increased in congestive heart failure20, 37—is presently unclear. It is also possible that the daily hassles of the disease cause chronic stress. Depending on the degree of underlying vulnerability, this could lead to a feeling of hopelessness followed by depression and reduced quality of life.38, 39
Limitations of the study
This study was performed at a tertiary referral centre. Thus the sample of patients with congestive heart failure does not represent the typical heart failure population seen by a general practitioner. Most of the latter would have a smaller impairment of left ventricular ejection fraction, a higher prevalence of coronary artery disease, and be older.40 Thus the prevalence of severe congestive heart failure in our hospital is likely to be higher than in community based hospitals. This should not have affected our results as we stratified all our analyses by different levels of disease severity.
Our study was too small to allow an assessment of the potential effects of sex and drug treatment on quality of life domains.
Another limitation might be the cross sectional design of the study. However, the main thrust of our study was the correlation between quality of life and somatic indices assessed at a particular point in time. Nevertheless, it would be highly desirable to document longitudinal changes in quality of life in patients with congestive heart failure, along with objective indicators of disease severity, to separate disease specific from non-specific changes in quality of life and to study cause–effect relations, especially in the domain of emotional impairment.
The comparison between our patients with congestive heart failure and patients with other diseases was limited to published reports on patients with liver, kidney, and mental diseases. However, a comparison of our sample with heart failure patients from the medical outcome study26 showed that impairment in quality of life seems to follow a similar pattern in patients with the same diseases in different countries.
Conclusions
Our findings indicate that quality of life is greatly impaired in congestive heart failure. All SF-36 scales decreased with NYHA functional class. In addition, patients with a more severe impairment of functional capacity—as assessed by the six minute walk test and peak oxygen uptake—had in general significantly lower SF-36 values. However, functional indices only partly explained the impairment in quality of life (by a maximum of 51% in one scale). Left ventricular ejection fraction and quality of life appear to be completely dissociated in these patients. Thus other potential determinants of quality of life should be explored.
From a clinical perspective, we conclude that quality of life ought to be specifically assessed to provide better monitoring of patients with congestive heart failure, as it cannot be extrapolated from routine clinical variables. The treatment of non-physical aspects of chronic disease should be considered as part of the management of congestive heart failure, in order to reduce anxiety, depression, and disturbances of social function. The routine use of the SF-36 might help to identify patients who need further help to improve their quality of life.
Acknowledgments
This study was supported by grants from the faculty for clinical medicine of the University of Heidelberg (projects 32/95 and 158/97).