Article Text

Abstract
Clinical targets are relatively easy to set but can be extremely difficult to implement. It is important to have organisational targets, in addition to clinical targets. The National Service Framework (NSF) for coronary heart disease sets national standards, defines service models, and establishes performance indicators for clinicians to meet. The new National Health Service ethos, in which front line staff are being empowered to develop innovative services tailored to local needs, is helping health professionals in primary care to deliver better care and improved “patient pathways” as promised in the NSF. However, there is still a need for additional resources in order to build capacity and provide support to the health care staff who are delivering the service.
- clinical targets
- coronary heart disease
- National Service Framework
- CHD, coronary heart disease
- NSF, National Service Framework
- NHS, National Health Service
- PCT, primary care trust
Statistics from Altmetric.com
- CHD, coronary heart disease
- NSF, National Service Framework
- NHS, National Health Service
- PCT, primary care trust

It is sometimes argued that the current undue emphasis on targets such as waiting times has led to poor morale among National Health Service (NHS) staff and has distorted health service delivery. However, few would disagree that the public has a right to expect an appropriate service, delivered in an appropriate setting by staff with appropriate skills.
In the UK, targets for cardiovascular disease are generally based on the work of expert groups. The British Hypertension Society has produced guidelines on the management of hypertension,1 and recommendations on the prevention of coronary heart disease (CHD) in clinical practice have been produced jointly by the British Cardiac Society, British Hyperlipidaemia Association, the British Hypertension Society, and the British Diabetic Association.2 Subsequently the Department of Health has produced National Service Frameworks, setting out targets based upon the work of these expert groups. These targets are based on the evidence and will evolve as new evidence accumulates. They may, therefore, change over the next few years. The level of risk at which to intervene may change. There may be new thresholds and targets for total cholesterol and low density lipoprotein cholesterol. When calculating risk, it should be important to consider life years gained as well as absolute risk. When deciding at which level of risk to intervene, financial issues are clearly important but it is capacity that is the main problem at present.
Clinical targets are easier to set than to implement. Hobbs and Erhardt have reported a European study3 looking at barriers to the implementation of guidelines. The most common barriers were found to be lack of time and lack of money (fig 1). Apathy/lack of motivation was a much less commonly reported factor.
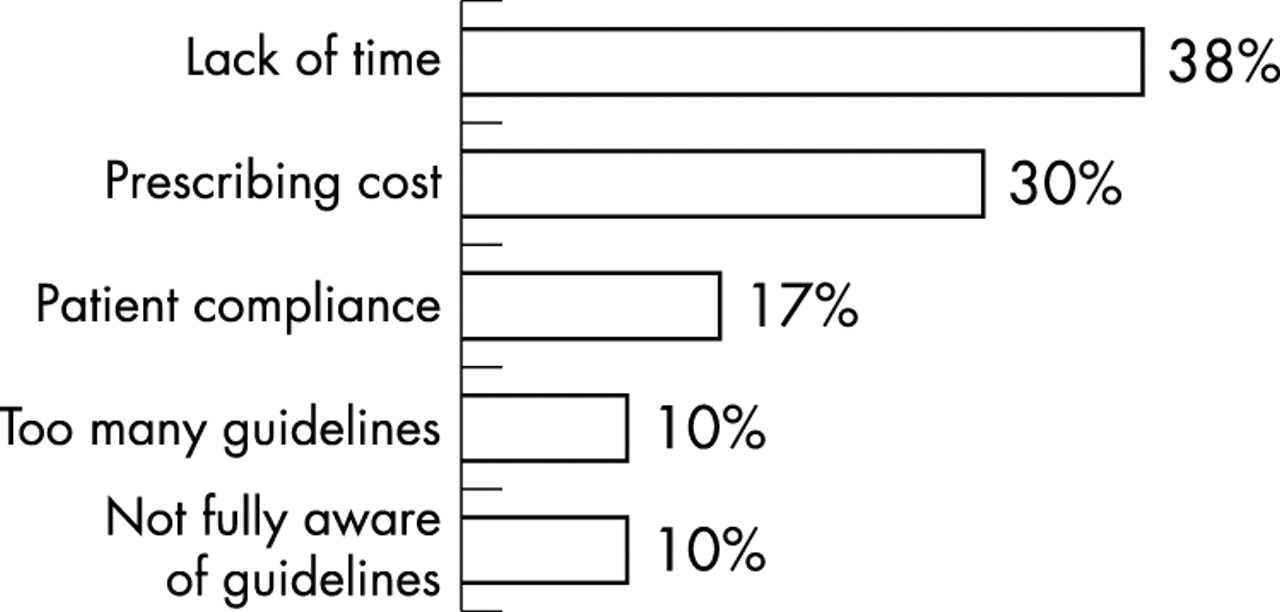
Barriers preventing implementation of guidelines. Adapted from Hobbs and Erhardt,3 with permission.
NATIONAL SERVICE FRAMEWORK FOR CHD
The National Service Framework (NSF) for CHD4 takes a practical, evidence based and flexible approach to tackling CHD. It sets national standards (clinical and organisational), defines service models, and establishes performance indicators. We have to meet the standards and targets but are given flexibility to consider local circumstances when developing new services.
The NSF covers the range of CHD from population based primary prevention, which is starting to gain momentum across the UK, through to cardiac rehabilitation. It has already made a difference in certain clinical areas. For example, organisational change within hospitals has led to a steady improvement in door-to-needle times for thrombolysis. There has also been a pronounced reduction in waiting times for coronary artery bypass graft surgery. When the NSF was first published it seemed inevitable that increased demand would lead to an exponential rise in the time that people waited for their procedure. The government put a substantial amount of money and effort into reducing these waiting times, and no patient now waits over 12 months. Similarly, waiting times for percutaneous coronary intervention have fallen. These findings show that service delivery can be improved, but it does take considerable effort and resources.
In primary care, the main initial effort has been in secondary prevention. The Primary Care Collaborative, which now covers some 400 practices and 4.5 million people, has been involved in improving access and secondary prevention and has achieved impressive results. Secondary prevention has improved greatly and this has been achieved with organisational change allied to limited funding. Most of the practices in the collaborative now have CHD registers. In some of the first wave primary care collaborative practices the CHD death rate has fallen by up to 40%, although this has not been validated. Some £15 million was available (from the Treasury Capital Modernisation Fund) for primary care through the collaborative and this has been used for equipment, such as ECG machines, echocardiography machines, defibrillators, and blood pressure monitors.
Statin ingredient costs can be taken as a marker of activity in cardiovascular disease prevention and, as shown in fig 2, there has been a pronounced increase in use of these drugs. Assuming that prescribing is targeted at people at highest risk, this indicates that practice is improving, even within the limited resources available.

As indicated by quarterly ingredient costs, the use of statins has increased notably since publication of the NSF.
The NSF also sets organisational milestones for secondary prevention in primary care and these have now largely been met. For example, most practices now have chronic disease registers, work as a multidisciplinary team and, critically, are now starting to measure their performance.
NHS PLAN
Most doctors, despite current poor morale in both primary and secondary care, are willing to change and are capable of change. But they do not have the capacity. The government’s approach to enable change is the NHS Plan.5 Key components of this are:
-
behaviour change, as well as structural change and record investment
-
faster and fairer—a national service delivered locally
-
more staff with better conditions working in new ways
-
good performance—autonomy; poor performance—intervention
-
learning culture—sharing best practice.
The NHS Plan makes sense. If it works, it will mean that we learn from each other, there will be more staff, the service will be designed and delivered locally, and there will be more resources. Internal research conducted by the Department of Health soon after the NHS Plan was published sought to find out what health service employees thought about the programme. Nurses were generally positive, welcoming more power going to the community, while doctors were more sceptical of the Plan. Staff were also asked how long they thought it would be before the NHS Plan would start to make a major difference. About 10% of nurses thought that change would occur within two years, and over 40% within three to five years. By contrast, no general practitioners thought it would make any difference in less than two years, and 50% were not optimistic that improvement would be seen within the next 10 years. Certainly the whole of the NHS cannot be transformed in the short term, but meaningful change can occur quickly when appropriate support is given.
How might that be achieved? The government’s consultation document Shifting the balance of power,6 which is part of the implementation of the NHS Plan, emphasises the need for a less “hands on” approach from the centre. It puts patients and staff at the heart of the NHS, with the empowerment of front line staff to develop innovative services, and the empowerment of patients. It also emphasises the need for practical arrangements to be determined locally. Primary care trusts (PCTs) are the cornerstone of this and there is considerable enthusiasm to make it work. If resources are made available to primary care then we will start to make a difference.
The new ethos involves a coordinated approach, with health professionals working together within networks of care (fig 3). The aim is to improve the “patient pathway” to deliver better care. There are many different models of care and the appropriate care must be provided in the appropriate setting. Some care currently provided in the secondary sector might not be appropriate to that setting so it is important to look at the care pathway, to build capacity and expertise in primary care, and to develop intermediate care. Diabetes care is a good example of how this might work. We should build capacity within individual practices but should look to share special expertise on a locality basis.

The new NHS ethos: networks of care. DGHs, district general hospitals, LITs, local implementation teams; PCOs, primary care organisations.
Organisational targets are also important when PCTs are devising their plans. The “strategic signposts” that have been identified are:
-
reducing health inequalities
-
improving the patient experience
-
improving services and outcomes
-
improving access
-
building capacity and resources
-
strategic governance (with accountability to the Department of Health, local authority and the people we serve).
What these organisational targets mean is that we have to ensure that people who need care can access it, we have to try and improve the way the patient feels about their experience at the hands of the NHS, and we have to reduce health inequalities.
AN EXAMPLE OF PROGRESS IN CARDIOVASCULAR PREVENTIVE CARE
Durham Dales PCT provides one example of how progress can be made in cardiovascular prevention. Durham Dales is a former mining community with a high disease burden. On average, 47% more people die prematurely in Durham Dales from heart disease every year than the national average.7 In its plan for implementing the NSF for CHD,4 Durham Dales PCT decided to employ specialist nurses (directly funded by the PCT) to coordinate, facilitate, and run CHD and heart failure clinics in all 12 practices. The nurses work to locally agreed guidelines and protocols. For example, they have an angina protocol, CHD guidelines for nurse led clinics to provide structured follow up, a lipid management protocol with an email service to a chemical pathologist, and a statin titration protocol.
The PCT funded CHD nurses are responsible for running the clinic. In some practices with poor capacity the CHD nurses actually provide the patient care while in others they put in time and resources to empower the staff who are already in the practice. They also use a standard ischaemic heart disease template so that every time a patient is seen their data are put into the computer so that regular audits can be carried out. The aims and objectives of the CHD nurse led clinics are to: assess and monitor symptoms and individual risk factors; provide education and lifestyle advice; encourage compliance to medication and to lifestyle changes; and review patients three, six, or 12 monthly. Audit data are collected quarterly using Miquest (a computer software program for data extraction) and there are quarterly meetings with the general practitioners.
Figure 4 shows an example of the outcomes that have been achieved. Eighty four per cent of patients have had their cholesterol recorded in the past year and 62% of patients are meeting their cholesterol target. However, the data also show the difficulty of maintaining improvement because over the last six months the number of patients at target level fell (from 71% to 62%), probably as a result of patient non-compliance with their prescribed medication. Continued follow up is therefore essential.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Durham Dales: number of patients with cholesterol recorded.
The number of patients with ischaemic heart disease who had their blood pressure recorded in the past year is 91%. Of these, 67% are reaching the British Hypertension Society audit target (< 150/90 mm Hg). The average across the UK is probably 30%. Also, around 90% of eligible patients are taking aspirin or other antiplatelet agents for secondary prevention. Overall, there are very high levels of secondary prevention and this success has been achieved because the service is organised, systematic, and structured.
Interestingly, although validity is not proven, since starting the secondary prevention programme the number of people having a myocardial infarction over the previous 12 months fell gradually, from 182 in the second quarter of 2001 to 137 in the second quarter of 2002. Of the people who have had an infarct, nearly 90% of them were on appropriate secondary prevention.
A patient survey was carried out in Durham Dales to assess what users felt about the service. It was found that 62.8% of patients reported having a better understanding of their condition and 43% had changed their eating habits since attending the clinic. Only 0.3% were not aware how to contact the CHD nurse if they wanted help and 3.5% said that they had not received adequate information on exercise. Most people were happy with the service and thought that their management and their understanding of the disease had improved.
Learning points
-
Clinical targets are necessary in cardiovascular medicine but when they are set a certain degree of pragmatism is needed. Targets that are evidence based but unrealistic are unlikely to be implemented
-
It will be possible to deliver better cardiovascular care but the only way to do this is to have targets, build capacity, and support service delivery
CONCLUSION
Clinical targets are important but it is up to the PCTs, as the representatives of the NHS in the community, to decide which of these targets they are in a position to deliver. We have to get the resources to build capacity. There is enthusiasm within primary care to move forward, but resources at present are inadequate.
DISCUSSION
Professor Martin Cowie: I was fascinated by your slide that showed doctors and other health care professionals at opposing ends of the spectrum of views about the NHS Plan. Why do you think clinicians have a more pessimistic view about change?
Dr Davis: Physicians have had the “benefit” of experiencing many NHS changes since 1990 and it appears to many of us that the changes have produced little benefit to our patients. Maybe experience has taught us to be cynical.
Question: As a GP interested in primary prevention, I think that perhaps this is a political and public health problem. On a population basis, look at the things that are against us and against our patients, particularly those in social classes 4 and 5: it’s not easy to cycle, there is still a smoking culture, and at the supermarket checkout if you look at somebody who is obese and what is in their trolley, you can see why they are obese. This is what we are fighting against.
Dr Davis: I agree absolutely. Individuals, parents, schools and the food industry do have to take responsibility. But changes are taking place. There are many initiatives that are starting to reduce inequalities in our communities. There are the Health Action Zones and projects such as Sure Start. Multi-agency effort is being made to try and change things but it is a long term project.
Question: I think many of us are frustrated because we have the ability to make a large difference to patients’ lives by delivering treatments but we don’t have the facilities or the resources or the organisations, so I think your issue of organisation is absolutely correct. As you pointed out, the big differences that will be made in health care are going to be through delivering the care effectively.
Dr Davis: Certainly there are too few health care professionals of all types. However, in Leeds we have audited our secondary prevention performance and found that some practices deliver good secondary prevention and yet they have either the same or less resource, in terms of nursing time, etc, than other practices that don’t do as well. So morale, motivation, capacity, expertise and organisational capability are all important.
Question: Few of us believe there is enough investment in health care in this country. There are not enough trained professionals, and therefore we can never deliver the sort of health care that we hope to until we address this issue.
Dr Davis: There will be more healthcare professionals joining the system but it is going to take some time and we have to make a start now. We have to use what resources we have got, perhaps in a more efficient way, and realise that the NSF is a 10 year project.