Article Text

Abstract
Objective To compare ticagrelor and prasugrel with clopidogrel for recurrent fatal and non-fatal myocardial infarction (reMI) in real-life conditions.
Methods Case-referent study using the Pharmacoepidemiological General Research eXtension (PGRx)-acute coronary syndrome (ACS) registry. Cases were patients with reMI from a cohort with index ACS or external to the cohort (same sites). Referents from the cohort, without recurrent event, were matched on index ACS type and date, age and sex with reMI cases. Multivariate conditional logistic regression assessed the OR (95% CI) for reMI associated with ticagrelor and prasugrel vs clopidogrel, adjusted for aspirin use and cardiovascular risk factors.
Results 1047 cases and 2234 matched referents were included. Compared with clopidogrel, ticagrelor and prasugrel were associated with respective ORs of 0.65 (95% CI 0.52 to 0.81) and 0.71 (95% CI 0.53 to 0.96) for reMI occurrence. ORs for ticagrelor and prasugrel vs clopidogrel were: 0.50 (95% CI 0.38 to 0.67) and 0.66 (95% CI 0.45 to 0.95), 0.39 (95% CI 0.24 to 0.62) and 0.44 (95% CI 0.26 to 0.75), 0.63 (95% CI 0.43 to 0.92) and 1.20 (95% CI 0.69 to 2.07), 1.11 (95% CI 0.72 to 1.72) and 0.82 (95% CI 0.44 to 1.54) when index ACS was a first MI, a first ST-elevated MI (STEMI), a first non-STEMI and a recurrent ACS, respectively, and 0.63 (95% CI 0.45 to 0.87) and 0.77 (95% CI 0.41 to 1.45) for patients aged ≥70 years.
Conclusions This real-world study showed a significant reduction of reMI with new antiplatelets compared with clopidogrel, ticagrelor being associated with a greater decrease of risk notably for first, either STEMI or non-STEMI. The larger magnitude of effect may be attributed to potential residual confounding or higher effectiveness compared with efficacy reported in trials (EMA Post Authorisation Study Registry Number EUPAS5905).
Statistics from Altmetric.com
Introduction
A key component in the management of acute coronary syndrome (ACS), antiplatelet therapy is effective in reducing the risk of acute ischaemic events.1 2 Platelet activation and aggregation is inhibited by cyclooxygenase inhibitors (aspirin), glycoprotein IIb/IIIa antagonists and P2Y12 antagonists (clopidogrel, prasugrel and ticagrelor), the latter two classes administered with aspirin.3–5 Recently, a number of studies concluded that, while carrying increased bleeding risk,6–8 ticagrelor and prasugrel are superior to clopidogrel in reducing major cardiovascular events. However, their effect under real-life conditions remains underexplored. Following a request by the French health authorities, this study aimed to determine if using ticagrelor or prasugrel after an ACS (unstable angina (UA), myocardial infarction (MI)) was associated with a lower risk of recurrent MI (reMI: new non-fatal MI or cardiac death) compared with clopidogrel use in real-life conditions.
Methods
The Antiplatelet agents and Recurrent Myocardial Infarction Study (AReMIS) case-referent study used the Pharmacoepidemiological General Research eXtension (PGRx) registry of ACS assembled by French cardiologists since 2007 as described elsewhere.9–12 The study period was 1 June 2013 (to allow 1 year after the marketing date for ticagrelor, the last antiplatelet agent (APA) licensed in France) to recruitment completion in 12 March 2016.
Study population
Composed of (i) a cohort of patients with an index ACS and (ii) reMI case-patients from the cohort or recruited externally to the cohort but in the same cardiology sites. Cohort patients not experiencing a reMI were defined as referents. Using this latter cohort, referents were selected for each case by individual matching.
To avoid selection bias, patients were consecutively recruited after prospective/retrospective identification by centres blind to the study objectives.
Cases and referents met similar eligibility criteria: (1) gender; (2) aged ≥18 years; (3) living in France; (4) index ACS during the study period, regardless of its rank (n=1, 2,…, n).
Case definition and ascertainment
Cases were patients with a reMI occurring after the index ACS, defined according to the ESC Committee for Practice Guidelines as13: (1) new spontaneous MI; (2) cardiac death due to MI lacking biomarkers; (3) stent thrombosis; (4) cardiac-related death or (5) UA with myocardial revascularisation (percutaneous coronary intervention (PCI) with/without stent or coronary artery bypass grafting (CABG)) and intensive care unit hospitalisation. When concerns of uncertainty were raised for cases as to their eligibility, an expert cardiologist (NDa) blinded to the exposure status was requested to independently review the cases.
Referents and matching
Referents were patients meeting the eligibility criteria above, but with no reMI at the time of matching. An average of two referents were matched to each case by: (1) date of index ACS (range: delay (±10%) between index ACS of case and corresponding reMI); (2) age ±1 year, and if unfeasible, year by year up until ±5 years, both within each of the strata aged ≤69 and ≥70 years separately; (3) sex; (4) type of index ACS (according to four types of index ACS: first UA, first ST-elevated MI (STEMI), first non-STEMI (NSTEMI), ACS with previous history of ACS prior to index ACS) and (5) type of exposure data source. Referents who became cases at a later date were retained as cases in the analysis (n=99), some of which were still used as matched referents over the period preceding the recurrence (n=49, out of 99).14 15 Referents were used as matched referents for one single case in order to avoid bias on relative risk estimates.16
Sample size estimation
The target sample size was established at 1250 cases and 2500 referents in order to obtain at least 80% power to detect significant ORs below 0.9 (main analysis) based on the assumptions that 1) one-third of the referents would be prescribed ticagrelor, one-third prasugrel or no-P2Y12 antagonist treatment and one-third clopidogrel and 2) no effect modification or influence on reMI risk by other P2Y12 antagonist use would occur, so that two-thirds of the sample size would be available for the comparison of each new P2Y12 antagonist versus clopidogrel. Expected 95% CI estimates were (0.677 to 0.945) (0.268 width), and (0.762 to 1.063) (0.310 width) for ORs of 0.8 and 0.9, respectively.
Time windows for defining APA exposure
The exposure of principal interest was defined as APA use within 30 days of the index ACS between cases and matched referents. The information on exposure was obtained from one of the following three sources (percentages below are mutually exclusive) as per the corresponding matching criterion:
Hospital treatment reports for drugs prescribed following the index ACS (86.8%);
Prescriptions issued by the patient’s treating physician or dispensation by her/his regular pharmacist (11.9%);
Patient interviews (1.3%).
A sensitivity analysis addressed drugs used immediately before the reMI among APA users. A patient was defined as exposed if he/she was prescribed an APA at least once within the 30 days’ time window prior to the reMI.
Potential confounders
Confounding by indication is based on the fact that APAs are prescribed differentially, according to health status and prognosis. To take it into account, the following wide range of measures was taken:
a stringent matching on age, type of index ACS, index date and exposure source;
and adjustment on factors defined a priori, including aspirin use, age, anticoagulant exposure, ACS preceding index ACS (number), hypertension (confirmed/use of antihypertensive drugs), diabetes (confirmed/antidiabetics intake), hyperlipidaemia (confirmed/lipid-lowering drugs intake), body mass index (BMI) and severe comorbidities (Alzheimer’s disease, Parkinson’s disease, rheumatoid arthritis, spondylitis, chronic obstructive pulmonary disease, viral hepatitis, schizophrenia, psychotic disorder, bipolar affective disorder, drug abuse (opiate dependency and addictions), multiple sclerosis, Crohn’s disease, ulcerative colitis, cirrhosis, renal failure and cancers).
Statistical analyses
Analyses relied on conditional logistic regression using case/matched referent status as the dependent variable. The principal exposure variable included the following mutually exclusive categories: clopidogrel, ticagrelor, prasugrel and no-P2Y12 antagonists users within 30 days of index ACS, corresponding to intention-to-treat (ITT) analysis. Ticlopidine (n=2) was grouped with clopidogrel.
Analysis of recent exposure was performed among antiplatelet users only, according to the following mutually exclusive categories: clopidogrel, ticagrelor, prasugrel and switchers, prescribed within 30 days prior reMI diagnosis.
A post hoc analysis examined the association between the risk of reMI and, ticagrelor and prasugrel compared with clopidogrel, each maintained between index ACS and reMI or matching date.
Crude and adjusted matched ORs, with 95% CIs were calculated for ticagrelor, prasugrel and no-P2Y12 antagonists use as individually compared with clopidogrel.
Ethics statement
The PGRx registries comply with principles set out by the Declaration of Helsinki, local regulatory requirements and the International Conference on Harmonisation–Good Pharmacoepidemiology Practice guidelines. Informed consent was obtained from all patients interviewed to establish risk factors and drug use between index ACS and reMI for cases or the matching date for referents. Confidentiality and anonymity of all patients recruited via PGRx registries have been maintained. Only physicians were compensated for inviting and recruiting patients.
Data collection and quality control
Data collected at inclusion included patient characteristics, cardiac and vascular medical history, comorbidities, symptoms, ECG results, type/date of index ACS and all drugs prescribed at index ACS discharge. Additionally, for reMI cases were collected symptoms, ECG, cardiac enzymes tests, type/date of reMI, vital status, date and cause of death and all treatments taken by the patient prior to reMI.
Data were collected using electronic case report forms (eCRF). Scientific oversight, conduct of operations and data management were the sponsor’s responsibility (PGRx). Quality control was part of systematic screening procedures for retrospective cases identification and data collection and concerned two-third of cases used in the study (the rest being prospectively included), for whom eCRFs were monitored against source documentation. This process implied anonymous data collection unless patient consent was obtained. Eligible patients were systematically posted information about the study and asked if they would: a) consent to participate, accepting to undergo the interview; b) not consent to participate but not objecting to the use of anonymous data for the study; c) fully object to the collection of medical data. Prospective patients’ recruitment was randomly audited during the recruitment period to ensure exhaustive inclusion of patients. The database includes an electronic audit trail for all data modifications, and critical variables were subjected to additional audits. Data for this study were extracted from the PGRx database on 11 May 2016.
Results
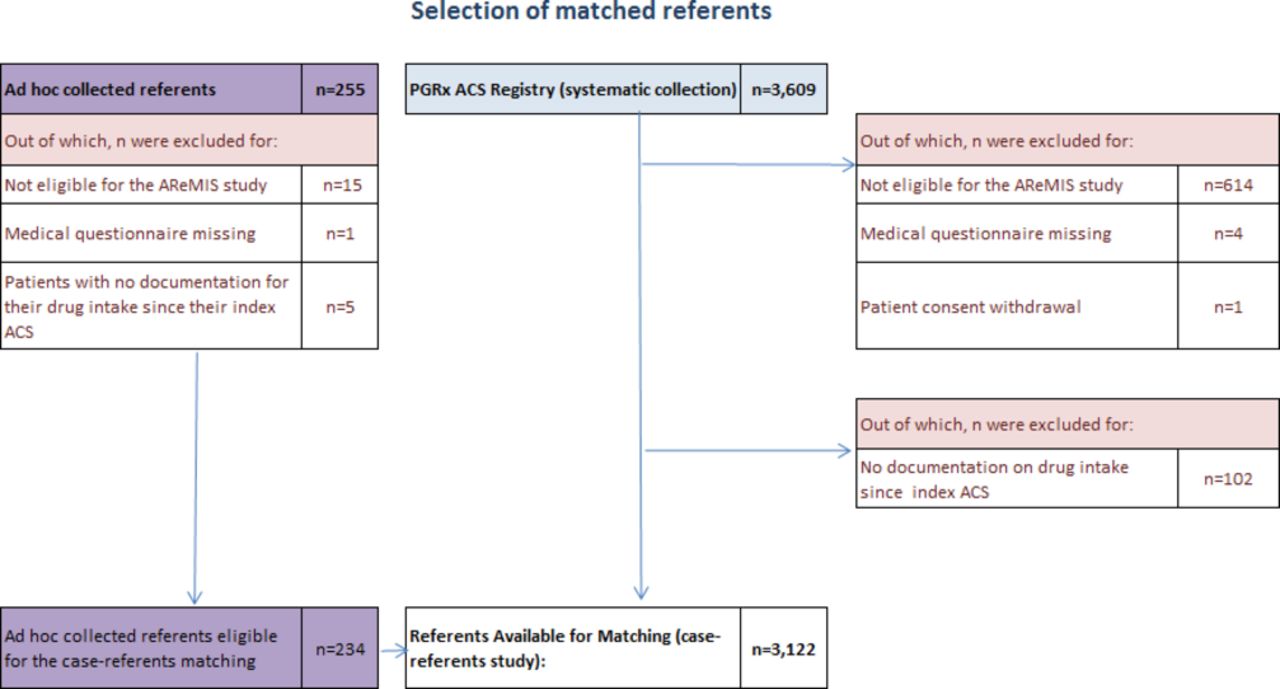
Overall, 275 cardiology centres and 26 general practices recruited a total of 1425 patients identified as reMI, of whom 1243 were found to be fully eligible as they met the definition of cases (figure 1). Of 3864 patients identified as potential referents, 3122 were fully eligible (figure 2).

Selection of cases. ACS, acute coronary syndrome; PGRx, Pharmacoepidemiological General Research eXtension; reMI, recurrent MI.

Selection of matched referents. ACS, acute coronary syndrome; AReMIS, Antiplatelet agents and Recurrent Myocardial Infarction Study; PGRx, Pharmacoepidemiological General Research eXtension.
The 3122 referents were characterised by APA use at the time of the index ACS in order to identify potential sources of confounding, especially by indication (table 1). Patients using clopidogrel were older (70.7 years, SD 12.5) than those taking ticagrelor or prasugrel (61.5, SD 12.3 and 57.8, SD 10.4), and more often females (33.3% vs 22.9% and 14.9%). Clear differences were also observed for the type of index ACS across the four categories of exposure, with clopidogrel users presenting more often with UA (13.8%) or ACS antecedents (21.7%) than ticagrelor (5.1% and 10.1%, respectively) or prasugrel users (4.4% and 9.7%, respectively), the latter two including more patients with first MI (respectively 84.8% and 86.0% vs 64.5% for clopidogrel). Clopidogrel users had also more often diabetes as well as CV and severe comorbidities. They were less often aspirin users and more often anticoagulant users. Some of these differences were expected as prasugrel is indicated in patients younger than 75 years subjected to PCI. No-P2Y12 antagonist users were more exposed to anticoagulant drugs than ticagrelor and prasugrel users but less exposed compared with clopidogrel users. Moreover, no-P2Y12 antagonist users underwent CABG in a much higher proportion than users (15.4% for no-P2Y12 antagonists users compared with 3.3%, 1.0% and 0.2% for clopidogrel, ticagrelor and prasugrel, respectively).
Description of risk factors at the index ACS in the 3122 fully eligible referents population according to APA use immediately postindex ACS
Table 2 provides a description of cases and matched referents. Cases were predominantly males (71%) with a mean age of 70.6 years. Just over half the cases were experiencing recurrence after a first MI and 32% had more than one previous ACS. Nearly all patients (>94%) had hypertension and hyperlipidaemia.
CV risk factors in cases of reMI and their matched referents (total population)
On implementing the extended and stringent matching criteria, 1047 cases were fully matched to 2234 matched referents (table 2).
Adjusting for potential confounders and risk factors reduced the risk of reMI by 35% among patients exposed to ticagrelor within 30 days of their index ACS, compared with those exposed to clopidogrel (OR 0.65; 95% CI 0.52 to 0.81; table 3). For patients exposed to prasugrel, the associated risk reduction was 29% (OR 0.71; 95% CI 0.53 to 0.96). Patients not prescribed a P2Y12 antagonist at discharge had a risk of recurrence identical to the reference group (table 3).
Association between reMI (non-fatal MI and cardiac deaths) and ITT exposure to APAs—cases and fully matched referents to type of index ACS
Applying less stringent matching on the type of index ACS (UA or MI, irrespective of ST-elevation or number of previous ACS) to increase the sample size, yielded superimposable results: significant risk reductions of 33% and 27% for ticagrelor and prasugrel, respectively, indicating that the model controls potential confounding induced by a partial matching on type of index ACS.
Stratified analyses
As the most critical confounder, stratification by age was performed below and above 69 years. The OR estimates for ticagrelor remained essentially unchanged (OR 0.63; 95% CI 0.45 to 0.87 for ≥70 years and OR 0.71; 95% CI 0.51 to 0.99 for their younger counterparts) (table 4). The risk reductions for prasugrel were not significant for either age-group.
Association between reMI and ITT exposure to APAs, stratified by age; cases and fully matched referents on type of index ACS
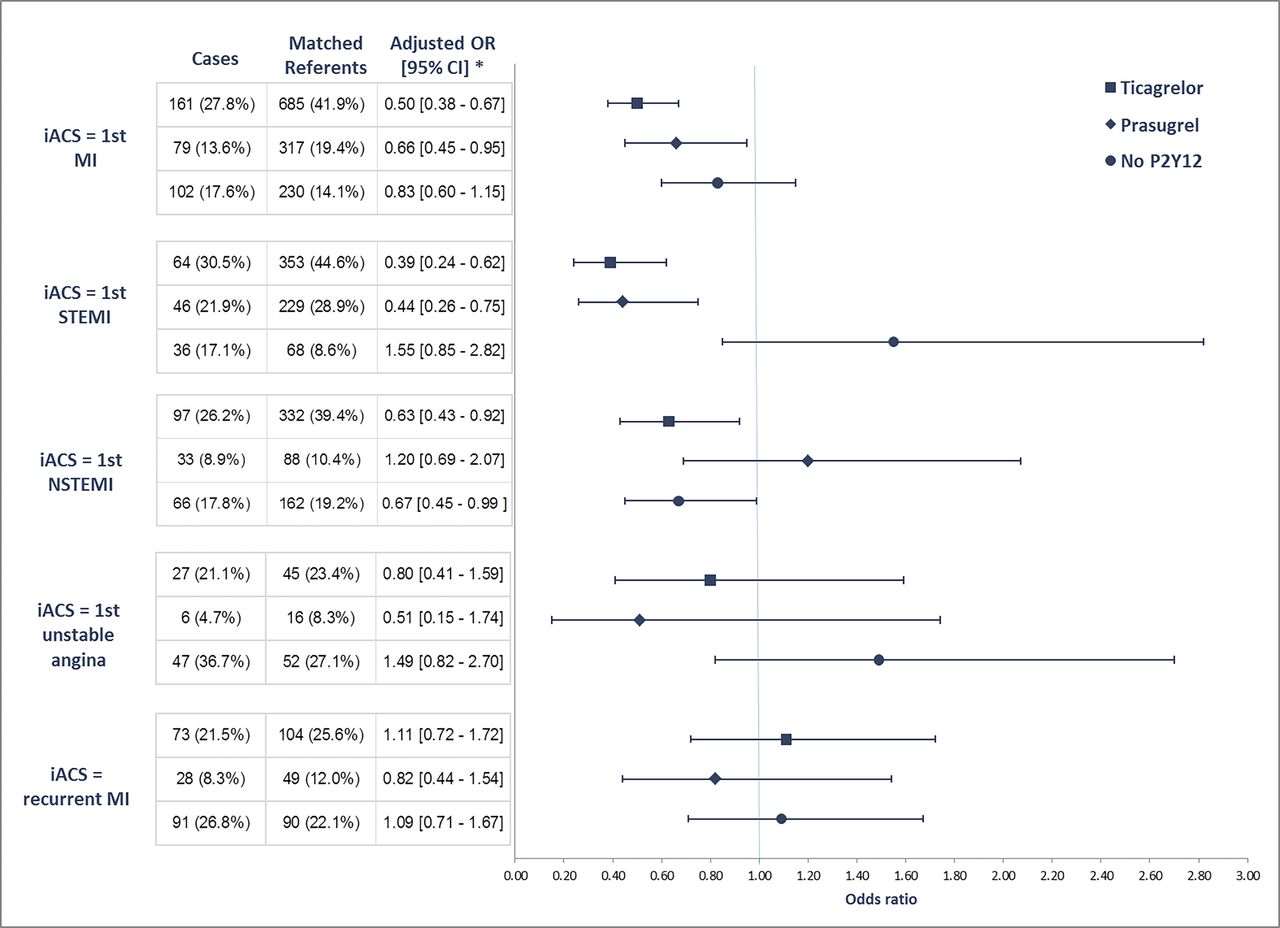
In view of the different distributions of the four categories of exposure according to types of index ACS (table 1), a likelihood ratio test to assess interaction between index ACS and category of APA exposure found this one to be significant (P<0.001). As a result, the analysis was matched in a stringent way.
OR estimates obtained among all patients (main model) showed a risk reduction in ticagrelor and prasugrel users compared with the reference group (figure 3), held only for patients with a first MI (including those with a first STEMI) as their index ACS. Among the latter, risk reduction for ticagrelor (OR 0.39; 95% CI 0.24 to 0.62) and prasugrel (OR 0.44; 95% CI 0.26 to 0.75) was highest among patients with a first STEMI; the risk reduction was less pronounced for those exposed to ticagrelor (OR 0.63; 95% CI 0.43 to 0.92) with no significant risk difference shown for prasugrel. Risk reduction for patients with a first UA as their index ACS taking ticagrelor was less than that of those taking prasugrel, but neither was significant (OR 0.80; 95% CI 0.41 to 1.59 vs OR 0.51; 95% CI 0.15 to 1.74).
{kind=link}
{kind=link}
{kind=link}
Association between reMI and ITT exposure to APAs by index ACS. ACS, acute coronary syndrome; APA, antiplatelet agent; iACS, index ACS; ITT, intention-to-treat; reMI, recurrent myocardial infarction; STEMI, ST-elevation MI.
Sensitivity analysis
A series of sensitivity analyses were performed using the main model to explore the robustness and stability of the results. Varying the time window of exposure to APAs, comparing the effect of maintaining the same medicine over time, restricting the analysis to patients exposed to both an antihypertensive and a lipid-lowering drug between the index ACS and the reMI date, excluding patients treated with anticoagulants, returned consistent results to those obtained in the principal ITT analysis (table 5).
Sensitivity analysis (a) by window of exposure (30 days before event date, and when the same medicine is maintained over time, only in users of APA), (b) restricting the analysis to patients exposed to both antihypertensive and lipid-lowering drugs between the index ACS and the reMI date and (c) excluding patients treated with an anticoagulant
Discussion
This large case-referent study addresses the real-life impact of new APAs in cardiology settings. It revealed a highly significant protective effect of ITT use of new APAs, more pronounced with ticagrelor after an ACS on the recurrence of non-fatal MI and cardiac death as compared with clopidogrel.
Findings are in line with those reported in controlled trials, which were not affected by confounding by indication. Therefore, the observation that new APAs, and notably ticagrelor, protect against reMI is highly plausible. Results in no-P2Y12 antagonist users appear to reflect those in clopidogrel users. A possible explanation is the proportion of no-P2Y12 antagonist users undergoing CABG surgery as their index ACS treatment compared with clopidogrel users (almost fivefold more).
The discussion lies on the magnitude of the effect observed for ticagrelor and prasugrel, which appears even larger in real-life use than that achieved in the trials the Study of Platelet Inhibition and Patient Outcomes (PLATO) and the Trial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition with Prasugrel–Thrombolysis in Myocardial Infarction (TRITON–TIMI 38).14 15 Potential residual confounding may explain the larger effect. However, differences in the populations analysed in both studies may explain also the difference in effect magnitude found. The trials were conducted under strictly controlled conditions. As such, the population in which the drug is ultimately licensed for use and that of the original trial may differ.14 Additionally, as more patients in the ticagrelor arm of PLATO discontinued treatment than in the clopidogrel arm, non-compliance should favour a type II error (failing to detect an effect), which is not the case here; however, this could explain the difference in the effect magnitude (ie, translated into higher effectiveness in real life than the efficacy assessed in trials). Such observations are not infrequent, contrary to common beliefs, when compliance to treatment is good. In a similar study conducted in PGRx, it was demonstrated that adherence to chronic cardiovascular treatment is excellent in France, notably in patients with MI.12 Another explanation to such larger real-life effect may relate to the fact that drugs and regimens are tailored to patients, while in trials these are usually fixed. This is the case of our study, where ticagrelor and prasugrel were mainly prescribed to patients (84.8% and 86%, respectively) with MI for whom the risk-reducing effects appear higher. Indeed, interaction analysis between index ACS categories and different APA use showed to be highly significant. Actually, understanding an ‘indication bias’ for aetiological research may translate into a positive impact from a public health viewpoint, as clinicians prescribe drugs to patients with higher expected benefit.
Real-world evidence studies have since been conducted. A study using the The Swedish Web-system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapies (SWEDEHEART)- Myocardial infarction (MI) (SWEDEHEART-MI)registry on 45 073 patients of whom about one-fourth were discharged on ticagrelor, the balance on clopidogrel, showed a cumulative probability of the combined outcome of death, MI and stroke at 24 months for patients in the ticagrelor cohort was half that of the clopidogrel cohort (11.7% (95% CI 10.6 to 12.8) vs 22.3% (95% CI 21.8 to 22.7)).17 Furthermore, a recent study investigated the effect of prasugrel and ticagrelor on all-cause mortality and stent thrombosis in a large single-centre, all-comers registry to find that both prasugrel and ticagrelor were associated with reduced mortality compared with clopidogrel in patients with STEMI and that ticagrelor also significantly reduced the rate of stent thrombosis which is consistent with our results.18 Our findings are also consistent with studies providing platelet function measurement data, most of these concluding that, compared with prasugrel, ticagrelor was associated with significantly greater P2Y12 inhibition with both achieving a significantly greater inhibition than clopidogrel during maintenance therapy.19 20
Study limitations
Significant differences in the distributions of individual P2Y12 antagonist usage were observed for age, type of index ACS, history of ACS events and aspirin use, which may represent significant confounding factors. Controlling for these factors through stringent matching and modelling may not have entirely controlled for residual confounding due to unmeasured unknown variables associated with more ‘subjective’ factors explaining physicians’ choice of prescription.
Study strengths
Besides the robust results, this study is unique in that it derives from the systematic identification and recruitment of cases and its case-referent design for the selection of matched referents, outside of any study hypothesis, thus minimising any potential selection bias. Furthermore, it relied on in-depth clinical and drug utilisation descriptions, objective sources of exposure information and stringent matching of referents to cases with a high level of comparability of case-referents series.
The study was conducted in more than 300 clinical centres, of which at least 90% were cardiology centres and 9% general practices, distributed across France and representative of different settings (university/general hospitals, private clinics, and ambulatory practices). The observed proportions of use of the different APAs closely reflect the sales of these products in France (data not shown).
Conclusion
In this real-world case-referent study using clinical data, ticagrelor and prasugrel were associated with a significant relative-risk reduction of reMI compared with clopidogrel, ticagrelor being associated with a greater decrease of risk than prasugrel notably for first MI, regardless of being STEMI or non-STEMI. This finding is consistent with clinical trials. The larger magnitude of the observed effect compared with clinical trials, may be attributed to potential residual confounding and/or higher effectiveness compared with reported trial efficacy (EUPAS5905).
Key questions
What is already known about this subject?
Evidence from clinical trials has shown new antiplatelet agents (APAs), ticagrelor and prasugrel, to be superior to clopidogrel in preventing major cardiovascular events; however, real-life use and effect of APAs is lacking.
What does this study add?
This first comparative effectiveness study using clinical data shows that, in real-life, the risk of recurrent myocardial infarction (MI) (non-fatal MI and cardiac death) is significantly lower in patients taking ticagrelor or prasugrel than in those taking clopidogrel, the magnitude of which was larger than the observed effect reported in clinical trials: 0.65 (95% CI 0.52 to 0.81) and 0.71 (95% CI 0.53 to 0.96) for ticagrelor and prasugrel vs 0.84 (95% CI 0.77 to 0.92) and 0.81 (95% CI 0.73 to 0.90), respectively, from corresponding pivotal trials.
How might this impact on clinical practice?
New-generation APAs should be considered when initiating or prescribing an APA in patients with acute coronary syndrome (ACS). Wide adoption of prasugrel and ticagrelor for ACS has the potential to decrease ischaemic events, including spontaneous MI.
Supplementary file 1
References
Footnotes
Contributors LG-B and LA drafted the protocol and the statistical analysis plan and conducted the analyses. LG-B drafted the manuscript. LG-B supervised all aspects of the study including document screening, selection, reconciliations, data collection, extraction and management. All authors made substantial contributions to conception or design of the work, reviewed the manuscript for important intellectual content, approved the final manuscript and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The PGRx data registry is owned by Centre for Risk Research Inc., an independent research organisation, to which a subscription can be purchased for observational studies. AstraZeneca (AZ) subscribed data from PGRx data registry specifically for the AReMIS study. The conception and design of the study as well as the data collection, management and analysis were conducted independently of AZ, under the supervision of a Scientific Committee.
Competing interests LG-B is currently employed by PGRx, a company susceptible of collaborating with virtually all the pharmaceutical companies worldwide. NDa declares having received financial support from Abbott France, Amgen SAS, AstraZeneca, Bayer Healthcare SAS, Boehringer Ingelheim France, Bristol-Myers Squibb, GlaxoSmithKline France, Lilly France SAS, MSD France, Novo Nordisk, Pierre Fabre, Re-Imagine Health Agency, Sanofi-Aventis France and Servier during the conduct of the study. JD declares having received personal fees for participating in Scientific Boards from AstraZeneca, Bayer and MSD. BF reports personal fees from AstraZeneca during the conduct of the study. AF, OM, FL, FG and NDe declare no conflict of interest. YC declares having received financial support for participating in Scientific Boards and consulting for Bayer, Boehringer, Novartis, Pfizer and Servier outside the submitted work. LB declares having received financial support in the form of grants and/or personal fees from AstraZeneca during the conduct of the study and also outside the submitted work. EP declares having received fees for lectures and/or consulting from Amgen, AstraZeneca, Bayer, BMS, Daiichi-Sankyo, Lilly, MSD, The Medicine Company, Sanofi and Servier. JB declares having received financial support from Association pour le Développement de l’Enseignement et des Recherches auprès des universités des centres de recherches et des entreprises d’Aquitaine, AstraZeneca, Servier and LASER during the conduct of the study. LA is chairman and stock owner in Analytica LASER, a consultancy susceptible of collaborating with virtually all the pharmaceutical companies worldwide. PGRx has no commercial interests in any of the products studied. Members of the PGRx network have no interest in any drugs or other factors studied using data collected using PGRx.
Patient consent Not required.
Ethics approval Ethics Review Committee of Paris-Ile de France III (Comité de Protection des Personnes Ile de France III) and the French Data Protection Authority (Commission Nationale de l’Informatique et des Libertés).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are available on request under certain conditions.
Collaborators PGRx-Acute Coronary Syndrome (ACS) Study Group Reda Aarras (Cabinet Privé, Beausoleil,), Nacera Abbou (Hôpital Stell, Rueil Malmaison); Kamel Abdennbi (Cabinet Privé, Paris), Ramzi Abi Akar (Georges Pompidou European Hospital, Paris), Corine Aboa Eboule (Centre Hospitalier de Semur-en-Auxois), Michel Adda (Cabinet Privé, Nice), Fifa Agbessi (Cabinet Privé, Lille), Bruno Agout (Cabinet Privé, Montoire Sur Le Loir), Saïd Ahres (Hopitaux Civls de Colmar), Linda Aissou (HU-Paris Seine Saint Denis, APHP, Bobigny), Franck Albert (Le Les Hôpitaux de Chartres, Le Coudray), Joachim Alexandre(Centre Hospitalier Universitaire de Caen), Alexandre Alies (Cabinet Privé, Montelimar), Thierry Allaouchiche (Cabinet Privé, Salon De Provence), Jean-Marc Amans (Cabinet Privé, Metz, Walid Amara (Groupe hospitalier intercommunal Le Raincy, Montfermeil), Ahmed Amiar (Groupe Hospitalier de Seclin Carvin), Gladys Amiel Oster (Cabinet Privé, Aubervilliers), Ahmed Amlaiky (Cabinet Privé, Mulhouse), Marc Amzallag (Cabinet Privé, Paris), Stephane Andrieu (Centre Hospitalier d’Avignon), Jean Marie Annic (Cabinet Privé, Neuville-sur-Saône), Sébastien Ansaldi (Cabinet Privé, Bastia), Cyprian Anton (Centre hospitalier de villeneuve, Villeneuve-sur-Lot), Luc Ardouin (Cabinet Privé, Fosses), Sebastien Armero (Hopital Européen Marseille), Abderrahmane Assaf (Cabinet Privé, Bapaume), Pierre Attali (Les Hôpitaux Universitaires de Strasbourg), Gilles Audebert(Cabinet Privé, La Seyne Sur Mer), Jean-Luc Auffray (Hôpital cardiologique, CHR Lille), Pierre-Antoine Ayrivie (Cabinet Privé, Beziers), Jean-Claude Azambourg (Cabinet Privé, Elbeuf), Olivier Azzano (Cabinet Privé, Cluses), Margarita Baert (Centre Hospitalier d’Albi), Jean-Philippe Baguet (CHU Grenoble Alpes, Grenoble), Souleyman Bai Sepou (Centre Hospitalier Verdun Saint-Mihiel, Verdun), Xavier Balaire (CHU Caen), Laurent Bali (Centre Hospitalier de Cannes), Jonathan Banayan (CH Tours, Chambray-Lès-Tours), Yves Banus (Clinique, Nantes), Charles Baranés (Cabinet Privé, Paris), Michel Barboteu (Clinique, Evecquemont), Franck Barbou (Hôpital Militaire, Paris), Alain Bardoux (Cabinet Privé, Maubeuge), Nicolas Baron (Hôpital Versailles, Le Chesnay), Maruan Barri (CH Longjumeau), Olivier (CH Avignon), Abdelkader Belhassane (Centre Hospitalier Cambrai), Jean Paul Bellefleur (Cabinet Privé, Saint-André-les-Vergers), Olivier Belliard (Clinique, Neuilly Sur Seine), Claudia Bemba (Centre Hospitalier du Centre Bretagne, Noyal Pontivy), Laurence Ben Cheikh M Hamed (Cabinet Privé, Longeville-en-Barrois), Tewfik Benchaa (CH Aix en Provence), Bouziane Benhalima (Cabinet Privé, Le Bourget), Lamjed Bensaad (Centre Hospitalier Stell, Rueil Malmaison), Jacques Berland (Clinique, Rouen), Yves Bermond (Cabinet Privé, Vannes), Jean Baptiste Berneau (Centre Hospitalier de la Côte Basque, Bayonne), Patrick Bert-Marcaz (Centre Hospitalier de Mâcon), David Bertora (Centre Hospitalier de Nice), Arnaud Bertrand (Cabinet Privé, Sigean), Sylvain Beurtheret (Hôpital Saint Joseph, Marseille), Yves Biron (Clinique, Rennes), Pierre Bizieux (Cabinet Privé, Marmande), Elodie Blicq (Centre Hospitalier de Versailles, Le Chesnay), Benoit Blondin (Cabinet Privé, Audun-le-Roman), Gerard Bocquillon (Cabinet Privé, Camblain-l’Abbé), Vera Bogdanova (Clinique, Paris), Emmanuel Boige (Cabinet Privé, La Teste-de-Buch), Marie-Thérèse Boire (Cabinet Privé, Ollioules), Jacques Bonnet (Hôpital Haut Leveque, CHU, Pessac), Thierry Bontemps (Cabinet Privé, Limoges), Sebastien Bosle (Centre Hospitalier de Brive), Khaled Karim Bouchlaghem (Cabinet Privé, Marseille), Georges Bouharb (Cabinet Privé, Montpellier), Fatima Boukhsibi (Centre Hospitalier Stell, Rueil Malmaison), Claire Bouleti (HU-Paris Nord site Bichat, APHP, Paris), Valerie Bourdin (Cabinet Privé, Azerailles), Guillaume Breard (Centre Hospitalier Blois), Myriam Brunehaut (Cabinet Privé, Clermont), Claude Brunschwig (Cabinet Privé, Cannes), Martine Cadoret (Cabinet Privé, Sablé-sur-Sarthe), Bruno Camenen (Cabinet Privé, St Herblain), Guillaume Canu (Centre Hospitalier de Bourg-en-Bresse), Claudine Carville (Cabinet Privé, Antony), Frederic Casassus (CHU Hopitaux de Bordeaux, Hôpital Haut-Leveque, Pessac), Rozenn Castera (Cabinet Privé, Bassussarry), Pierre Causse (Cabinet Privé, Saint Etienne), Philippe Cayron (Cabinet Privé, Montpellier), Isabelle Centa (Cabinet Privé, Le Kremlin-Bicêtre), Alexandre Chabrun (Cabinet Privé, Poitiers), Abdeslem Chalani (Centre Hospitalier de Narbonne), Stephane Champagne (Centre Hospitalier Universitaire Henri Mondor, Creteil), Philippe Chapon (Centre Hospitalier de Valence), Warren Chasseriaud (Hôpital Haut Leveque, CHU, Pessac), Nassim Chebahi (Hôpital prive Le Bois, Lille), Nicolas Chedru (Cabinet Privé, St Nazaire), Saida Cheggour El Bouazzaoui (Centre Hospitalier d’Avignon), Philippe Chemin (Cabinet Privé, Bordeaux), Nouredine Chemmam (Centre Hospitalier de l’Ouest Vosgien, Neufchateau), Kamal Chennouf (Clinique, Brou-Sur-Chantereine), Sami Cheriaa (CH Meaux), Paul Chiri (Cabinet Privé, Marseille), Claire Chisseray-Pramotton (Cabinet Privé, Nante), Guy Chivoret (Cabinet Privé, Toul), Frederic Chometon (Cabinet Privé, Firminy), Rene Codjia (CH GHPSO Creil, Creil), Philippe Commeau (Clinique, Ollioules), André Corbin (Cabinet Privé, Dinan), Yves Cottin (CHU Dijon, Dijon), Ulun Crimizade (Les Hôpitaux Universitaires de Strasbourg), Bernard Crousillat (Centre Hospitalier General Salon de Provence), Julie Curjol-Soto (Cabinet Privé, Bouc-Bel-Air), Adib Dabboura (Cabinet Privé, Villefranche-sur-Saône), Alphonse Dacunto (Cabinet Privé, St Fons), Nicolas Danchin (Hôpital européen Georges-Pompidou, Paris)Bernard Darmon (Cabinet Privé, Colomars), Patrick Dary (Cabinet Privé, Saint-Yrieix-la-Perche), Olivier Dascotte (Cabinet Privé, Saint-André-lez-Lille), Guillaume De Geeter (Cabinet Privé, Anzin), Axel De Labriolle (Cabinet Privé, Montauban), Roland De Ladreit (Cabinet Privé, Saint-Germain-au-Mont-d’Or), Olivier De Sauniere (Hôpital de Roanne), Jean Louis Deaux (Cabinet Privé, Condom), Matthieu Debonne (Cabinet Privé, Marcq En Baroeul), Eric Decoulx (CH Tourcoing), Georges Delamare (Cabinet Privé, Blois), Nicolas Delarche (Centre hospitalier François Mitterrand, Pau), Bernard Delfour (Cabinet Privé, Greasque), Dominique Delsart (Cabinet Privé, Bersee), Mathieu Deltreuil (Centre Hospitalier Jacques Boutard, Saint-Yrieix-la-Perche), Philippe Dematteo (Cabinet Privé, Valognes), Chems Eddine Deramchi (Cabinet Privé, Montevrain), Mohamed Derbali (Centre Hospitalier de Châteauroux), Jacques Derycke(Cabinet Privé, Saint-Laurent-de-la-Salanque), Josyane Devico Palacci (Cabinet Privé, Marseille), Olivier Dibon (Centre Hospitalier Régional d’Orléans), Katy Didier Petit (Centre Hospitalier Intercommunal de la Haute Saône, Vesoul), Romain Didier(Centre Hospitalier Universitaire de Brest), Abdelkader Djebabra (Cabinet Privé, Venissieux), Charly Djeumen Wandji (Centre Hospitalier Lucien Hussel, Vienne), Bernard Doucet (Cabinet Privé, Chambery), Christophe Dromnelle (Cabinet Privé, Chamalieres), Philippe Duc (Cabinet Privé, Fontenay-sous-Bois), Valerie Duchatelle (Hôpital Paris Saint Joseph, Paris), Audrey Duchemin (CH Tourcoing), Agathe Dumont (Cabinet Privé, Dammartin-en-Goële), Daniel Dumortier (Cabinet Privé, Lille), Pierre Dumoulin (Cabinet Privé, Courbevoie), Sylvie Dunica (Cabinet Privé, Paris), Arnauld Dupoizat (Cabinet Privé, Toulouse), Catherine Dupont Biscaye (Cabinet Privé, Preignac), Patrick Dupouy (Clinique, Melun), Philippe Durandet (Cabinet Privé, La Rochelle), Pierre Duron (Cabinet Privé, Chaville), Laurent Dutoit (Centre hospitalier Henri Mondor, Aurillac), Fawaz El Damen (Hôpital Albert Schweitzer. Colmar), Fouad El Ghelbazouri (Cabinet Privé, Montargis), Abdellatif El Hallak (Clinique, Evecquemont), Adnan El Jabali (Centre Hospitalier de Bagnols-Sur-Ceze), Rami El Mahmoud (Hôpital Ambroise-Paré, Boulogne-Billancourt), Meyer Elbaz (Centre Hospitalier Universitaire de Toulouse), Mariam Elkohen (Clinique, Villeneuve D’Ascq), Frederic Gad Elmkies (Cabinet Privé, Compiegne), Pascale Enguehard (Cabinet Privé, Coutances), Alfonso Epicureo (Cabinet Privé, Carvin), Michele Escande Orthlieb (Clinique, Marseille), Ghazaleh Esna (Cabinet Privé, Rambouillet), Jean-François Falquier (Cabinet Privé, Bergerac), Jean Louis Farges (Cabinet Privé, Bethune), Abderrazah Farza (Cabinet Privé, Fontainebleau), Fouad Fattah (Centre Hospitalier René Dubos, Pontoise), Maurice Fauvel (Cabinet Privé, Colomiers), Jihad Fawaz (Cabinet Privé, Talence), Maxime Fayard (Centre Hospitalier Chalon-Sur-Saône), Zohir Fekhar (Cabinet Privé, Narbonne), Israel Feldmann (Cabinet Privé, Haguenau), Emile Ferrari (Centre Hospitalier, Nice), Gérard Fhal (Cabinet Privé, Marseille), Pierre Fichter (Cabinet Privé, Marseille), Laurent Fischbein (Cabinet Privé, Bourg Les Valence), Pascale Flinois (Cabinet Privé, Rognac), Stéphane Fol (Cabinet Privé, La Roche sur Foron), Eric Forest (Cabinet Privé, Vannes), Christian Fournier (Cabinet Privé, Sabres), Pierre Frances (Cabinet Privé, Banyuls sur Mer), Eric François (Cabinet Privé, Aire sur la Lys), Jean-Marc Frey (Cabinet Privé, Sète), Reynald Friedmann (Cabinet Privé, Montpellier), Alain Furber (Centre Hospitalier, Angers), Karim Gacem (Centre Hospitalier, Cholet), Pierre-Henry Gacon (Centre Hospitalier Dijon), Olivier Gaillard (Cabinet Privé, Annonay), Thierry Garban (Cabinet Privé, Carquefou), Eric Garbarz (Centre Hospitalier, Clichy), Waddah Garman (Cabinet Privé, Paris), Jean-Pierre Garnier Crussard (Cabinet Privé, Orange), Olivier Gartenlaub (Cabinet Privé, Maisons-Alfort), Tatiana Gavrilina (Centre Hospitalier, Chambéry), Audrey Gehanne (Cabinet Privé, Vannes), Michel Gehanne (Cabinet Privé, Vannes), Michel Geneves (Cabinet Privé, Paris), Jean-Louis Georges (Centre Hospitalier, Le Chesnay), Fahmi Ghanem (Centre Hospitalier, Châteauroux), Nachwan Ghanem (Centre Hospitalier, Eaubonne), Catherine Gigandet (Cabinet Privé, Mérignac), Jean-Marie Gil (Hôpital des Armées, Marseille), Mathieu Gillet (Cabinet Privé, Nantes), Aude Girard-Girod (Cabinet Privé, Thonon les Bains), Jean-Pierre Giuliani (Cabinet Privé, Toulon), Chandrah Goburdhun (Centre Hospitalier, Tulle), Antonio Gongora (Clinique, Lievin), Marc Goralski (Centre Hospitalier, La Source), Hervé Gourio (Cabinet Privé, Douarnenez), Stéphane Greciano (Centre Hospitalier, Colmar), Michel Gudin De Vallerin (Cabinet Privé, Paris), Hajar Lahbabi Guennioui (Centre Hospitalier, Tourcoing), Pierre Guéranger (Centre Hospitalier, Villefranche de Rouergue), Anne-Lise Gugenheim (Centre Hospitalier, Corbie), Philippe Guillot (Cabinet Privé, Sète), Jean-Paul Guillot (Centre Hospitalier, Bayeux), Véronique Haddad (Clinique, Aubagne), Djamel Hamani (Clinique, Paris), Karim Hasni (Centre Hospitalier Intercommunal, Toulon), Eric Helms (Cabinet Privé, Saint-Priest), Richard Hersh (Cabinet Privé, Longwy), Sébastien Hess (Centre Hospitalier Universitaire, Strasbourg), Bernard Hijazi (Cabinet Privé, Nîmes), Agnès Holeman (Cabinet Privé, Clichy), Charlotte Honore (Clinique, Rouen), Daniel Horovitz (Cabinet Privé, Savigny sur Orge), Franck Houeze (Centre Hospitalier, Charleville-Mézières), Jean-Sébastien Hulot (Hôpital Pitié-Salpêtrière, Paris) Frédéric Hurson (Cabinet Privé, St-Maur-des-Fosses), Messaoud Idir (Centre Hospitalier, Périgueux), Karim Ikhlef (Centre Hospitalier, Belfort), Adi Issa (Centre Hospitalier, Bourges), Olivier Jaboureck (Centre Hospitalier, Bourges), Gildas Jacob (Cabinet Privé, Saint-Brieuc), Saed Jazayeri (Centre Hospitalier Universitaire, Dijon), Christophe Jego (Centre Hospitalier, Maubeuge), Philippe Jessen (Clinique, Aubervilliers), Marc Jobbe Duval (Cabinet Privé, Neuilly sur Seine), Thierry Joseph (Centre Hospitalier Intercommunal, Quimper), Jean-Philippe Joubert (Cabinet Privé, Orange), Patrick Jourdain (Centre Hospitalier, Pontoise), Rémy Juste (Cabinet Privé, Lagny sur Marne), Thomboj Theostyphyl Kabsel (Centre Hospitalier, Le Puy en Velay), Yasser Kalaaji (Centre Hospitalier, Gonesse), Gaetan Karrillon (Centre Hospitalier, Eaubonne), Didier Kassehin (Centre Hospitalier Intercommunal, Poissy), Sébastien Kerebel (Hôpital des Armées, Toulon), Ryad Khallaayoune (Centre Hospitalier Intercommunal, Marmande), Idriss Kioueh (Centre Hospitalier, Semur en Auxois), Alain Kojfer (Cabinet Privé, Hénin-Beaumont), Bassel Koujan (Centre Hospitalier, Châteauroux), Mouhammad Mazen Kouzez (Centre Hospitalier, Vichy), Jérome Kozak (Cabinet Privé, Marcq en Baroeul), Hélène Kremer (Centre Hospitalier Universitaire, Strasbourg), Fabien Labombarda (Centre Hospitalier Universitaire, Caen), Cécile Lacote Roiron (Centre Hospitalier Universitaire, Bron), Alain Lacroix (Cabinet Privé, Brive), Christian Lagiewka (Clinique, Aubervilliers), Emmanuel Lamaze (Cabinet Privé, Bussang), Bruno Lambert (Cabinet Privé, Pleumeur-Gautier), Eric Lamy (Cabinet Privé, Caen), Ingrid Landragin Martin (Cabinet Privé, Angoulême), Pascal Lauvergnat (Cabinet Privé, Auray), Tahar Lazizi, Centre Hospitalier, Laval), Pierre Le Franc (Cabinet Privé, Rouen), Jean-Michel Le Hir (Cabinet Privé, Marseille), Laurent Leborgne (Centre Hospitalier Universitaire, Salouel), Florence Leclercq (Centre Hospitalier Régional Universitaire, Montpellier), Guillaume Lecoq (Clinique, Caen), Didier Lefevre (Cabinet Privé, Castres), Yves Lemiere (Cabinet Privé, Conflants Ste Honorine), Gérard Lesage (Cabinet Privé, Plancher les Mines), Pierre-François Lesault (Clinique, Le Havre), Nicolas Lhoest (Clinique, Strasbourg), Yann Lize (Cabinet Privé, Challans), Pierre Llaty (Cabinet Privé, Poitiers), Judith Loeb Mansour (Cabinet Privé, Argences), Jean-Louis Long (Cabinet Privé, Vichy), Philippe Longere (Cabinet Privé, Draguignan), Christian Lorentz (Cabinet Privé, Belfort), Jean-Christophe Louchart (Cabinet Privé, Bethune), Jules Louembe (Hôpital des Armées, Clamart), Arezki Lounis (Centre Hospitalier Intercommunal, Montfermeil), Olivier Lozinguez (Clinique, Noisy le Grand), Anne Luycx Bore (Cabinet Privé, Compiègne), Jean-Louis Lysakowski (Cabinet Privé, Lyon), Daniel Bey (Centre Hospitalier du Centre-Bretagne, Noyal Pontivy), Pascal Mabire (Cabinet Privé, Fleury sur Orne), Amine Madi (Centre Hospitalier, Vénissieux), Patricia Magnus (Cabinet Privé, Thann), Benaouda Mahdjoub (Cabinet Privé, Bressuire), Muhyjealdeen (Centre Hospitalier, Soissons), Hamid Makki (Cabinet Privé, Châtillon sur Seine), Henri Malaterre (Cabinet Privé, Marseille), Gregory Malbranque (Cabinet Privé, Hénin-Beaumont), Bernard Manne (Cabinet Privé, Le Blanc Mesnil), Michel Mansour (Centre Hospitalier, Belfort), Jacques Mantoux (Cabinet Privé, Limoux), Denis Manzi (Cabinet Privé, Chate), Stéphanie Manzo Silberman (Hôpital Lariboisière, Paris), Arnaud Marchand (Cabinet Privé, Aix en Othe), Mounir Maroun (Cabinet Privé, Givet), Michel Marsaux (Cabinet Privé, Conflants-Ste-Honorine), Michael Martelet (Centre Hospitalier, Langres), Olivier Martin (Cabinet Privé, Nice), Victor Mateus (Centre Hospitalier, Laval), Serge Mazouz (Cabinet Privé, Chelles), Daniel M’bey (Centre Hospitalier, Noyal Pontivy), Karine Mear (Centre Hospitalier, Bourges), Fatiha Mehlal (Centre Hospitalier, Saumur), Dominique Mellin (Cabinet Privé, L’isle sur la Sorgue), Bruno Meme (Cabinet Privé, La Riche), Paul Menu (Centre Hospitalier Universitaire, Poitiers), François-Xavier Meriaux (Cabinet Privé, Fougères), Zoubir Mesli (Cabinet Privé, Montpellier), Nathan Messas (Centre Hospitalier Universitaire, Strasbourg), Charlotte Mestrallet Rivet (Centre Hospitalier Intercommunal, Rumilly), Marie Metivier (Cabinet Privé, Paris), Thibaud Meurice (Cabinet Privé, Lille), Jonathan Meurice, Centre Hospitalier Universitaire, Lille), Philippe Meurin (Clinique, Villeneuve Saint-Denis), Stéphane Mielot (Cabinet Privé, Marseille), Christopher Mielot (Cabinet Privé, Plan de Cuques), Alexandre Mischie (Centre Hospitalier Intercommunal, Chateaubernard), Marcin Mlotek (Cabinet Privé, Saint-Etienne), Patrick Montant (Cabinet Privé, Cluses), Daniel Montaut (Cabinet Privé, Negrepelisse), Olivier Morel (Centre Hospitalier Universitaire, Strasbourg), Claudine Morillon (Cabinet Privé, Vannes), Pierre-Julien Moro (Clinique, Marseille), Saleh Mortada (Centre Hospitalier, Forbach), Yann Morvan (Cabinet Privé, Joigny), Lakri Mouaci (Cabinet Privé, Beauvais), Joseph Mouallemm (Centre Hospitalier, Langres), Maan Moulla (Centre Hospitalier, Soissons), Jean-Philippe Mouret (Centre Hospitalier, Marseille), Samer Mousi (Centre Hospitalier, Niort), Gérard Muller (Centre Hospitalier, Ste Feyre), Jean-Joseph Muller (Cabinet Privé, Strasbourg), Melchior Munet (Cabinet Privé, Decines Charpieu), Lyassine Nait Saidi (Centre Hospitalier Intercommunal, Toulon), Olivier Nallet (Centre Hospitalier Intercommunal, Montfermeil), Marc Nejman (Cabinet Privé, La Villedieu), Le Anh Tuan Nguyen (Centre Hospitalier, Niort), Van Hung Nguyen (Centre Hospitalier, Aurillac), Dorian Nitu (Centre Hospitalier, Eaubonne), Elisabeth Nyom (Centre Hospitalier, Laon), Alice Ohanessian (Centre Hospitalier, Briis sous Forges), Codin Olariu (Cabinet Privé, Moulins), Bernard Olivieri (Cabinet Privé, Juan les Pins), Azeddine Ouguoujil (Cabinet Privé, Gennevilliers), Michel Ovize (Centre Hospitalier Universitaire, Bron), Didier Pacaud (Centre Hospitalier, Sens), Franck Paganelli (Centre Hospitalier Universitaire, Marseille), Mathieu Pankert (Centre Hospitalier, Marseille), Francesco Paparoni (Centre Hospitalier, Seclin), Kumaressen Pareathumby (Cabinet Privé, Prades), Serge Pariente (Cabinet Privé, Paris), Philippe Paule (Hôpital des Armées, Brest), Julie Peroz (Hôpital Américain, Neuilly sur Seine), Eric Pichon (Cabinet Privé, Vesoul), Alain Pinzani (Cabinet Privé, Sète), Christophe Piot (Clinique, Montpellier), Renaud Piquemal (Cabinet Privé, Thionville), Eric Plantrou (Cabinet Privé, Pont de l’Arche), Alain Pleskof (Cabinet Privé, Chelles), Grégoire Poletti (Centre Hospitalier Régional Universitaire, Nîmes), Jean-Marc Ponzio (Cabinet Privé, Nîmes), Iulia Popescu (Centre Hospitalier Intercommunal, Chantepie), François Poulain (Cabinet Privé, Paris), Bruno Pouzet (Clinique, Le Chesnay), Raphael Poyet (Hôpital des Armées, Toulon), Etienne Puymirat (Hôpital Européen Georges Pompidou, Paris), Gonzalo Quaino (Centre Hospitalier, Chambéry), Virginie Rachenne-Barthomeuf (Cabinet Privé, Bourgoin-Jallieu), Benjamin Ramanamamonjy (Clinique, Tarbes), Mamy Randriamora (Centre Hospitalier, Arras), Patrice Raymond (Cabinet Privé, Asnie), Pierre Reins (Cabinet Privé, Schiltigheim), Caroline Richalet (Cabinet Privé, Echirolles), Christian Roche (Cabinet Privé, Saint-Etienne), Nicolas Charles Roche (Hôpital des Armées, St-Mande), Jérome Roncalli (Centre Hospitalier Universitaire, Toulouse), Roger Rosario (Hôpital Saint-Joseph, Marseille), Chantal Rosati Gretere (Cabinet Privé, Montrouge), Guillaume Rosey (Cabinet Privé, Toulouse), Vincent Roule (Centre Hospitalier Universitaire, Caen), Philippe Rouquette (Cabinet Privé, Mauguio), Olivier Rousseau (Cabinet Privé, Saint-Etienne), Dorine Rousseau (Cabinet Privé, Neuville en Ferrain), Christophe Roussel (Centre Hospitalier Intercommunal, Fréjus), Simon Saad (Centre Hospitalier, Chateaubriant), Rim Saad Blidi (Centre Hospitalier, Eaubonne), Maurice Saade (Cabinet Privé, Hesdin), Rémi Sabatier (Centre Hospitalier Universitaire, Caen), François Saint-Pierre (Centre Hospitalier Intercommunal, Arles), Adrien Salem (Cabinet Privé, Marseille), Emmanuel Salengro (Centre Hospitalier Intercommunal, Villeneuve St-Georges), Eric Saloux (Centre Hospitalier Universitaire, Caen), Ali Reza Samadi (Centre Hospitalier Intercommunal, Villeneuve St-Georges), Alain Sandalian (Cabinet Privé, Marseille), Marc Sander (Cabinet Privé, Saint-Germain-en-Laye), Alexandru Sarbu Pop (Centre Hospitalier, Charleville-Mézières), Virginie Sarrau (Cabinet Privé, Gennevilliers), Bachir Sayegh (Centre Hospitalier, Colmar), Armand Sbaiti (Cabinet Privé, Montpellier), Antony Scemama (Clinique ,Suresnes), Patrick Schlageter (Cabinet Privé, Marckolsheim), Gregory Schoukroun (Cabinet Privé, Cornebarrieu), Philippe Schraub (Cabinet Privé, Ajaccio) Olivier Selton (Cabinet Privé, Toul), Jamal Seoud (Cabinet Privé, Creil), Sylvain Sifaoui (Cabinet Privé, Cannes), Laurent Simonnet (Cabinet Privé, Obernai), Cristina Sirbu (Centre Hospitalier Universitaire, Vandoeuvre les Nancy), Joelle Sissmann (Cabinet Privé, Paris), Charles Sokic (Cabinet Privé, Bischwiller), Renaud Solanet (Cabinet Privé, Roubaix), Jean-Pierre Soulard (Cabinet Privé, Cholet), Jean Souyri (Cabinet Privé, Valentine), Philippe Gabriel Steg (Hôpital Bichat, Paris), Stéphane Tabet (Cabinet Privé, Enghien les Bains), Jean-Yves Tabet (Clinique, Villeneuve Saint-Denis), Samira Taihi (Centre Hospitalier, Bar le Duc), Marc Takla (Centre Hospitalier Intercommunal, Epinal), Sunhok Tan (Cabinet Privé, Arles), Roger Tanguy (Cabinet Privé, Plouzane), Philippe Tanielian (Cabinet Privé, Marseille), Frédéric Targosz (Centre Hospitalier, Perpignan), Jean Tartar (Cabinet Privé, St Pol sur Mer), Jacques Teboul (Clinique, Saint-Laurent-du-Var), Mohamed Terbah (Hôpital de la Source, Orléans), Sébastien Terrazzoni (Clinique, Antony), Pascal Tessier (Cabinet Privé, Saint-Raphael), Catherine Thiebaut (Cabinet Privé, Saint-Mandrier-sur-Mer), Denix Tixier (Cabinet Privé, Clamart), Pascal Toban (Clinique, Tours), Kossi Lolonyo Tonyiga (Centre Hospitalier, Rueil-Malmaison), Philippe Trehou (Cabinet Privé, Guise), Olivier Tricot (Centre Hospitalier, Dunkerque), Charlotte Trouillet (Centre Hospitalier, La Rochelle), Xavier Troussier (Clinique, Massy), Basile Tsoumbou (Centre Hospitalier, Chateaubriant), Albert Mudiambi Tuambilangana (Centre Hospitalier, Cherbourg Octeville), Philippe Uge (Cabinet Privé, Bordeaux), Clément Unal (Cabinet Privé, Vaison la Romaine), Denis Uzan (Cabinet Privé, Aulnay sous Bois), Franck Valero (Cabinet Privé, Anzin), Richard Valla (Cabinet Privé, Digne), Frédéric Vallet (Centre Hospitalier, Niort), Yann Valy (Centre Hospitalier, La Rochelle), Bruno Vaquette (Centre Hospitalier, La Rochelle), Olivier Varenne (Hôpital Cochin, Paris), Eric Verbrugge (Centre Hospitalier, Boulogne sur Mer), Marc Villaceque (Cabinet Privé, Nîmes), Fabrice Vine (Cabinet Privé, Paris), Thibaud Violet (Cabinet Privé, Annecy), Bruno Vittecoq (Cabinet Privé, Saint-Michel-sur-Orge), Bernard Charlot Wafo (Centre Hospitalier, Briis sous Forges), Rana Wanly (Centre Hospitalier, Vienne), Michel Wazana (Cabinet Privé, Strasbourg), Michel Weingrod (Cabinet Privé, Plaisir), Steve Werquin (Centre Hospitalier, Dunkerque), Xavier Wuydin (Cabinet Privé, Cappelle en Pévèle), Cossi Virgile Yadouleton (Centre Hospitalier, Brive la Gaillarde), Wael Yafi (Centre Hospitalier, Mulhouse), Gilles Zemmour (Centre Hospitalier, Cannes).