Article Text

Abstract
Objective Although the factors associated with short-term survival from out-of-hospital cardiac arrest (OHCA) are well established, relatively little is known about the factors that influence long-term survival. In this study, we describe the 15-year survival outcomes of OHCA survivors and examine the influence of peri-arrest factors and 12-month outcomes on long-term survival.
Methods Survivors of OHCA between 2000 and 2014 identified from the Victorian Ambulance Cardiac Arrest Registry were linked with state-wide death records. Kaplan-Meier survival curves and Cox regression models were used to estimate long-term survival outcomes.
Results A total of 3449 patients were included with a mean survival duration of 11.9 (95% CI 11.7 to 12.1) years. The 1-year survival rate was 92.2% (95% CI 91.3% to 93.1%), while the 5, 10 and 15-year survival rates were 81.4% (95% CI 79.9% to 82.8%), 70.1% (95% CI 67.9% to 72.1%) and 62.3% (95% CI 58.9% to 65.5%), respectively. The standardised mortality rate of OHCA survivors was 5.6 times that of the standard Australian population in the first-year postarrest, but approached that of the standard population 5 years postarrest. Few peri-arrest factors were independently associated with long-term survival after discharge. Rather, transport to a percutaneous coronary intervention-capable hospital and discharge home from hospital were associated with longevity. Returning to work and favourable physical/functional recovery were associated with improved survival after 12 months.
Conclusions OHCA survivors experience relatively favourable long-term survival after discharge from hospital. While peri-arrest factors had little influence on long-term survival after hospital discharge, favourable recovery postdischarge was associated with improved long-term outcomes.
- Cardiac arrhythmias and resuscitation science
- Cardiac arrest
- Epidemiology
- Quality and outcomes of care
Statistics from Altmetric.com
Introduction
Out-of-hospital cardiac arrest (OHCA) is a significant public health problem, with a global average survival to hospital discharge rate of 7%.1 A number of factors have been demonstrated to improve short-term prognosis. Early initiation of cardiopulmonary resuscitation (CPR) and defibrillation by either advanced or lay rescuers have been demonstrated to improve a patient’s chance of return of spontaneous circulation and survival to hospital discharge.2 3 In addition, other arrest and emergency response factors, such as response time, witness status, location and initial arrest rhythm, have also been associated with short-term survival both locally and internationally.4 5
Conversely, relatively little is known about the long-term survival of patients with OHCA, or the factors that influence their longevity after hospital discharge. A recent report found that the majority of OHCA survivors were alive 12 months postarrest with favourable functional and neurological outcomes, and that only witness status and the rhythm of arrest are associated with improved prognosis.6 Acute hospital interventions including percutaneous coronary intervention (PCI) and therapeutic hypothermia have been associated with improved long-term survival, as have arrests of cardiac aetiology.7 8 In contrast, increasing age, a history of myocardial infarction, cigarette smoking and poorer neurological recovery at hospital discharge have been associated with an increased mortality rate postdischarge.9–12
However, evidence surrounding the association between arrest and emergency response factors and long-term survival after OHCA is limited, and the factors which may improve long-term outcomes have not been well established. Additionally, the importance of 12-month health-related quality of life (HR-QOL) outcomes as descriptors of long-term survival is yet to be determined. In this report, we describe the long-term survival of patients discharged from hospital following OHCA, and assess the influence of peri-arrest factors on long-term survival. We hypothesised that peri-arrest factors which are associated with short-term survival may also influence patient longevity. In addition, we evaluate the association between HR-QOL measures recorded 12 months postarrest and longer-term survival, and compare the mortality rates of OHCA survivors at each year of follow-up with those of the Australian standard population.
Methods
Study design
We conducted a registry-based follow-up study of OHCA survivors by linking two state-wide registries in Australia: the Victorian Ambulance Cardiac Arrest Registry (VACAR) and the Victorian Registry of Births, Deaths and Marriages (the death registry). Between 1 January 2000 and 31 December 2014, we identified all OHCA survivors to hospital discharge from the VACAR, and linked baseline arrest data to death records. The primary outcome measure was length of survival after OHCA. The collection and use of VACAR data was approved by the Victorian Government Department of Health Human Research Ethics Committee as a quality assurance project, and access to hospital data is approved by all participating institutions.
Setting
The state of Victoria, Australia, has a population of approximately 5.9 million people and covers more than 227 000 km2. Ambulance Victoria (AV) is the single provider of emergency medical services (EMS) in the state. Advanced life support and mobile intensive care ambulance paramedics co-respond to cardiac arrest events. Basic life support trained first responders, including fire fighters and Community Emergency Response Teams, are also dispatched to suspected OHCAs in select areas through the state-wide dispatch authority. The AV clinical practice guidelines are aligned with the recommendations of the Australian Resuscitation Council (http://www.resus.org.au). Patients resuscitated from OHCA are transported to the closest emergency department. A regionalised system of care for patients with OHCA has not been established.
Data sources
The VACAR is a state-wide OHCA clinical quality registry and is described in detail elsewhere.13 Patient and case details are collected for all OHCAs attended by EMS in Victoria. Data capture is facilitated by paramedic completion of electronic patient care records on conclusion of each case.14 A broad data search criteria identifies potential OHCA events, and confirmed cases are entered into the registry in alignment with Utstein requirements. Where electronic records are not available, searches of paper patient care records are conducted.15
Hospital discharge status is obtained for transported patients. Dates of death are recorded for all deaths occurring during admission. In this study, patients with OHCA who survived to hospital discharge were linked to the death registry to ascertain the date of death. Patients who were not linked with a death record were assumed to be alive, and were censored at the date of linkage (17 September 2015).
HR-QOL data were extracted from the VACAR for patients whose arrest occurred between January 2010 and June 2014. Since 2011, the VACAR has collected HR-QOL and functional status of 12-month survivors. The data capture process and HR-QOL outcomes have been previously described.6 Briefly, a list of survivors to hospital discharge is provided to the death registry to establish the date of death of patients who die within the 12-month period. Patients who are not linked are assumed to be alive, and are invited to participate in telephone interviews. Participants (patients or proxies) answer the 12 Item Short Form Health Survey (SF-12), EuroQol-5D (EQ-5D) and Glasgow Outcome Scale-Extended (GOSE), plus questions related to work status. The SF-12 is completed by patients rather than proxy responders. Responses from the SF-12 are also used to derive the SF-6D, a single health state value ranging from 0.345 to 1.00.16 The VACAR maintains a 12-month follow-up rate of approximately 81%.
Statistical analyses
Baseline characteristics are presented as frequencies and proportions for categorical variables, and median (IQR) or mean (SD) for continuous variables, as appropriate for the distribution of the data. Kaplan-Meier survival curves were constructed, and the mean (95% CI) survival durations were calculated, for the entire study population, and by baseline and arrest characteristics. Follow-up years were calculated from the date of OHCA to the date of death or censoring, as appropriate. Survival durations were compared across initial arrest rhythms using the log-rank test. Unadjusted Cox proportional hazards regression models were constructed to obtain estimates of the influence of arrest factors on long-term survival. To satisfy the proportional hazards assumption, these models stratified the baseline hazard by initial arrest rhythm. Stratification assigns a unique baseline hazard to each initial arrest rhythm, while the coefficient associated with each covariate remains constant across all rhythms. Age and gender-specific death rates from the Australian Bureau of Statistics Life tables17 were used to calculate standardised mortality ratios (SMR) for each year of follow-up.
A multivariable Cox proportional hazards regression analysis was conducted to understand the independent association between baseline and arrest characteristics and long-term mortality. This model also stratified the baseline hazard by initial arrest rhythm to satisfy the proportional hazards assumption. The following covariates were included: age at the time of arrest, gender, arrest aetiology, witness and bystander CPR status, EMS response time, arrest location, metropolitan/rural region and transport to a PCI-capable hospital. Adjusted survival curves were constructed for each initial arrest rhythm to visualise the differences in survival outcomes.
To assess the association between survival and 12-month HR-QOL measures, unadjusted and adjusted Cox regressions were used. For these analyses, only patients who were alive 12 months postarrest were included, and follow-up years were calculated from 12 months postarrest rather than the date of OHCA. GOSE categories ‘Vegetative state’ (n=4 patients) and ‘Lower severe disability’ (n=82 patients) were combined due to the infrequency of their observation. To prevent overfitting models, adjusted HRs were obtained by selectively excluding the above-mentioned covariates until only those that showed evidence of an association with long-term survival remained. As a result, models were adjusted for age only. In addition, to satisfy the proportional hazards assumption, the models with SF-12 mental component summary (MCS), physical component summary (PCS) and SF-6D included were stratified by age group, and the former model was also stratified by the MCS itself (grouped by quartiles). Due to the distribution of the EQ-5D variable (39.7% of respondents achieved a score of 1), an additional dichotomous variable, indicating whether the patient achieved a score of 1, was included with the EQ-5D score.
The goodness of fit of all models was assessed using Cox-Snell residuals. All analyses were conducted using Stata Statistical Software: Release 14 (College Station, Texas, USA: StataCorp LP). p Values from a two-sided test <0.05 were considered statistically significant.
Results
Baseline characteristics
A total of 3618 patients were discharged from hospital during the study period, equating to 10.9% of patients with OHCA who received a resuscitation attempt (online Supplementary Figure S1). Patients with a missing name or date of birth (n=169) were excluded from analyses as this missing information prevented their linkage with the death registry. This left 3449 patients for analysis. The mean age was 60.3 (SD 17.5) years, and 74.7% were male (table 1). Most patients arrested due to a presumed cardiac cause (86.5%), and the first recorded arrest rhythm was shockable in 77.0%. In total, 83.7% of survivors were discharged directly home from hospital. Patients who were excluded from analyses did not differ from the study population in terms of baseline characteristics.
Supplementary file
Baseline characteristics of out-of-hospital cardiac arrest survivors to hospital discharge
Unadjusted long-term survival estimates
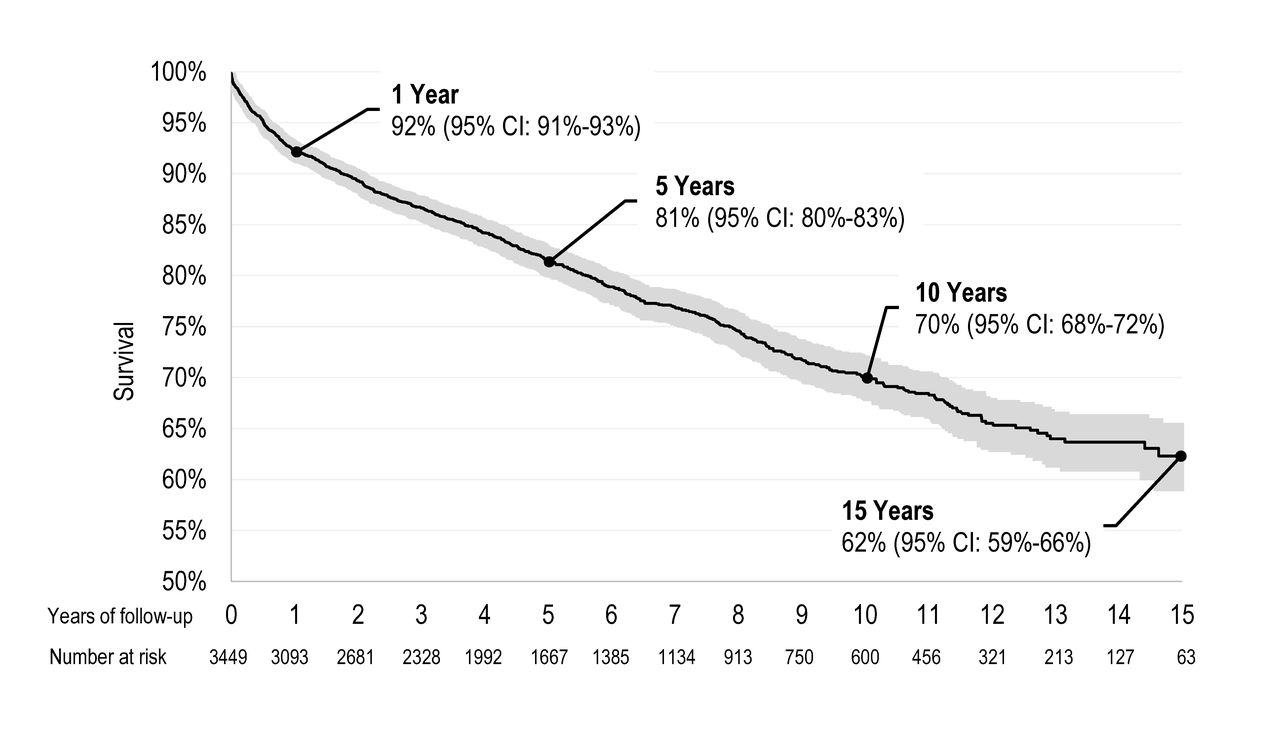
Figure 1 provides the Kaplan-Meier estimates of long-term survival for the study population. The 1-year survival rate was 92.2% (95% CI 91.3% to 93.1%), while the 5, 10 and 15-year survival rates were 81.4% (95% CI 79.9% to 82.8%), 70.1% (95% CI 67.9% to 72.1%) and 62.3% (95% CI 58.9% to 65.5%), respectively. The mean survival duration was 11.9 (95% CI 11.7 to 12.1) years (online supplementary table S1).

Kaplan-Meier survival estimates of out-of-hospital cardiac arrest survivors to hospital discharge.
According to unadjusted analyses (although with baseline hazard stratified by initial arrest rhythm), improved long-term survival was associated with younger age, shorter EMS response time, arresting due to overdose or poisoning or in a public location, transport to a PCI-capable hospital and discharge home from hospital (table 2). Kaplan-Meier curves across subgroups of baseline characteristics are provided in online supplementary figure S2. A shockable arrest rhythm was associated with an improved survival duration (p<0.001). The 10-year survival rate was 72.6% (95% CI 70.0% to 75.0%) for patients with a shockable arrest rhythm, 57.7% (95% CI 52.2% to 62.8%) for pulseless electrical activity (PEA) and 68.4% (95% CI 61.4% to 74.3%) for asystole. Patients arresting in an aged care facility/supported accommodation had the lowest survival rate across all subgroups analysed, with a 10-year survival rate of 28.1% and a mean survival duration of 5.9 (95% CI 4.5 to 7.3) years.
Cox regression analyses of long-term mortality
Age and gender SMRs
Yearly SMRs of patients with OHCA are presented in figure 2 across follow-up years. The SMR for the overall population was 1.9 (95% CI 1.7 to 2.0). Within the first year of follow-up, the rate of death in OHCA survivors was 5.6 (95% CI 4.9 to 6.3) times that of the standard population. After 5 years, the risk of death was similar to that of the standard population.

{kind=link}
{kind=link}
Yearly standardised mortality ratios (95% CI) of out-of-hospital cardiac arrest survivors to hospital discharge in relation to the standard Australian population. Year 12 includes years 13, 14 and 15.
Adjusted long-term survival estimates
According to multivariable analyses, the hazard of death increased by 59% (95% CI 37%–84%, p<0.001) for each 10-year increase in age (table 2). Gender and EMS response time were not significantly associated with mortality. However, the hazard of death for patients arresting in an aged care facility/supported accommodation was 2.3 (95% CI 1.7 to 3.1, p<0.001) times that of patients arresting in a private residence, while arresting in public location was associated with improved long-term outcome (HR=0.8, 95% CI 0.66 to 1.0, p=0.046). Being witnessed to arrest and/or receiving bystander CPR was not associated with an improvement in long-term survival; however, transport to a PCI-capable hospital and discharge directly home from hospital were associated long-term survival improvements.
Given that our model was stratified by initial arrest rhythm, adjusted survival curves are presented in online supplementary figure S3 according to initial arrest rhythm. For the typical bystander witnessed arrest, the probability of 5, 10 and 15-year survival for shockable arrests were 83.1%, 70.8%, and 60.6%, respectively. For patients whose initial arrest rhythm was PEA, the 5, 10 and 15-year survival rates were 68.7%, 59.8% and 58.6%, respectively, while for asystole they were 68.5%, 63.8% and 59.0%, respectively.
Impact of 12-month HR-QOL on survival
A description of 12-month HR-QOL outcomes is provided in online supplementary table S2, and the mean (95% CI) survival duration after 12 months is presented in online supplementary table S3. According to unadjusted analyses, survival after 12 months was associated with returning to work, higher SF-6D and SF-12 PCS scores, and higher EQ-5D scores (table 3). After adjusting for age, the hazard for death of patients who returned to work after arrest was 0.21 (95% CI 0.05 to 0.84, p=0.028) times that of patients who had not returned to work. Additionally, the hazard of patients reporting an upper severe disability according to the GOSE was 3.1 (95% CI 1.3 to 7.6, p=0.013) times that of patients who reported an upper good recovery. The hazard for death after 12 months also decreased by 3% for each one point increase in SF-12 PCS score (p=0.046). While patients with an EQ-5D score of 1 had reduced mortality compared with patients with other scores, there was little evidence that more subtle shifts in EQ-5D impacted on survival.
Associations of 12-month outcomes with long-term mortality
Discussion
The purpose of this study was to assess 15-year survival outcomes in patients with OHCA surviving to hospital discharge. Our large study suggests that patients with OHCA experience relatively high survival after hospital discharge, with 10 and 15-year survival rates of 70.1% and 62.3%, respectively. While a shockable arrest rhythm was associated with favourable outcomes, other factors commonly associated with short-term survival both locally and internationally, such as witness status, bystander CPR and EMS response time,5 13 did not influence long-term survival after hospital discharge. Instead, transport to a PCI-capable hospital and discharge directly home from hospital were associated with improved long-term survival outcomes, and returning to work after discharge was associated with improved survival after 12 months.
The 5-year survival rate in our study (81.4%) is higher than previous OHCA studies which report rates between 43% and 77%.7 9 12 18 However, our cohort consists of a greater proportion of patients arresting due to a presumed cardiac aetiology and into an initial shockable rhythm, both of which have been associated with improved long-term survival.8 For instance, our 5-year survival rate is similar to a small Norwegian study in which the proportion of patients with a presumed cardiac aetiology or initial shockable arrest rhythm were comparable (91% and 80%, respectively).19 Additionally, our 5-year survival rate of OHCA survivors arresting due to a presumed cardiac aetiology (82.2%) is higher than the 3-year survival rate of patients discharged from hospital following isolated coronary artery bypass graft surgery (76.7%),20 and much higher than the 5-year survival rate of patients discharged with acute heart failure (21.5%).21
However, the rate of death after hospital discharge in our population was greater than the Australian standard population in the first 5 years postarrest. In particular, in the first-year postdischarge, the rate of death of OHCA survivors was 5.6 times that of the standard population. Previous studies have also reported high mortality rates in the first-year postarrest, with one small study reporting an SMR of 4.6 times that of an age and gender matched population.19 22 Although high mortality rates may be explained by the discharge of palliated patients or the increased risk of death associated with neurological impairment, these results also highlight the importance of postarrest care, rehabilitation and quality of life.
For example, our results suggest that 12-month recovery may be a better descriptor of long-term survival postdischarge than peri-arrest factors, and it is therefore plausible that longevity may be influenced by early hospital-based interventions and medical follow-up. Previous studies have associated PCI7 23 and therapeutic hypothermia7 with reduced long-term mortality. In our study, transport to a PCI-capable hospital was associated with longevity. However, given that many patients with OHCA in Victoria do not undergo early PCI, the association between receiving hospital and reduced mortality may be reflective of other factors. For instance, in patients with acute coronary syndromes, the prescription of secondary prevention medications, lifestyle advice and referral to rehabilitation are reported to differ across hospitals,24 25 and are likely to be associated with long-term survival.26 It is therefore possible that long-term survival could be further improved through the implementation of a regionalised approach to cardiac arrest care in Victoria, in which specialised postarrest treatment and follow-up is provided to patients with OHCA.27 28
Additionally, returning to work postarrest, which has previously been described as a reliable proxy for favourable neurological and functional recovery,29 was associated with improved survival after 12 months in our study. Previous studies have also associated lower cerebral performance category and activities of daily living scores at hospital discharge with favourable long-term survival.11 12 Although the majority of OHCA survivors report favourable HR-QOL outcomes postarrest,6 further improvements in long-term survival may be achieved through focussed rehabilitation initiatives in the first 5 years postarrest when the risk of mortality is greatest. For example, previous research has suggested that 12-month HR-QOL post-OHCA can be improved with administration of psychosocial therapy and provision of self-management strategies such as problem solving skills and action plans.30
Our study is limited by its retrospective nature. In addition, while transport to a PCI-capable hospital is monitored by VACAR, we are unable to report whether patients actually underwent emergency PCI or the distance to the nearest PCI-capable hospital. Similarly, we are unable to report other hospital-related factors such as temperature management, protocols for withdrawal of care, prescription of prevention medications or models for discharge direction. It is possible that early withdrawal of care may give rise to a cohort of survivors biased towards long-term survival. Our 12-month HR-QOL data were captured in only a subgroup of patients arresting between 2010 and June 2014. These analyses are therefore restricted to 12-month survivors with a maximum follow-up duration of 4.75 years. Furthermore, as the VACAR collects HR-QOL at 12 months postarrest only, we are unable to describe the long-term HR-QOL and prognosis of survivors, or the influence of HR-QOL at other time points in the patient’s recovery on long-term survival. Finally, it is possible that patients may have died outside the state of Victoria, and their death may therefore not have been captured by the Victorian death registry.
Conclusion
Our study suggests that the majority of OHCA survivors survive beyond 12 months, with 10 and 15-year survival rates of 70.1% and 62.3%, respectively. However, the mortality rate of OHCA survivors in the first 5 years post-arrest was greater than the Australian standard population. While a shockable arrest rhythm was associated with more favourable outcomes, other peri-arrest factors did not influence long-term survival after hospital discharge. Instead, we found evidence to suggest that discharge directly home from hospital and favourable 12-month recovery were better descriptors of longevity. However, further investigation of the in-hospital and postarrest factors which influence long-term survival is warranted.
Key questions
What is already known on this subject?
Evidence surrounding the association between arrest and emergency response factors and long-term survival following out-of-hospital cardiac arrest (OHCA) is comparatively limited when compared with that surrounding short-term survival. In addition, the importance of 12-month health-related quality-of-life outcomes as descriptors of longer-term survival after 12 months is yet to be determined.
What might this study add?
In OHCA survivors to hospital discharge, the 1-year survival rate was 92.2%, while 70.1% and 62.3% survived to 10 and 15 years, respectively. In the first-year postarrest, the standardised mortality rate of OHCA survivors was 5.6 times that of the standard population. Discharge directly home from hospital and favourable 12-month recovery were associated with longevity.
How might this impact on clinical practice?
This study provides evidence that OHCA survivors can live a long-life postarrest. Investigation of in-hospital clinical practices and postarrest rehabilitation initiatives that optimise a patient’s recovery is needed given the association between favourable recovery and long-term survival.
Acknowledgments
We would like to acknowledge the Victorian Ambulance Cardiac Arrest Registry team members (Marijana Lijovic, Vanessa Barnes, Resmi Nair, Marian Lodder, Davina Vaughan and Kerri Anastasoupolos) for their continued maintenance of the registry.
References
Footnotes
Contributors EA was responsible for data extraction, analysis and writing the manuscript. RW provided statistical oversight. All authors contributed to and reviewed the final manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.