Article Text

Abstract
Objective This prospective study aimed to determine to what extent clinical symptoms and neurohumoral activation are improved in patients with severe aortic valve stenosis after transcatheter aortic valve implantation (TAVI) with the CoreValve prosthesis.
Methods From June 2008 to June 2009 consecutive patients with symptomatic severe aortic valve stenosis (area<1 cm2), age≥75 years with a logistic EuroSCORE ≥15% or age>60 years plus additional specified risk factors were evaluated for TAVI. Examinations of study patients were performed before and 30 days after TAVI and comprised assessment of quality of life (Minnesota living with heart failure questionnaire, [MLHFQ]) 6-minute walk test, measurement of B-type natriuretic peptide and echocardiography. Aortic valve prosthesis was inserted retrograde using a femoral arterial or a subclavian artery approach.
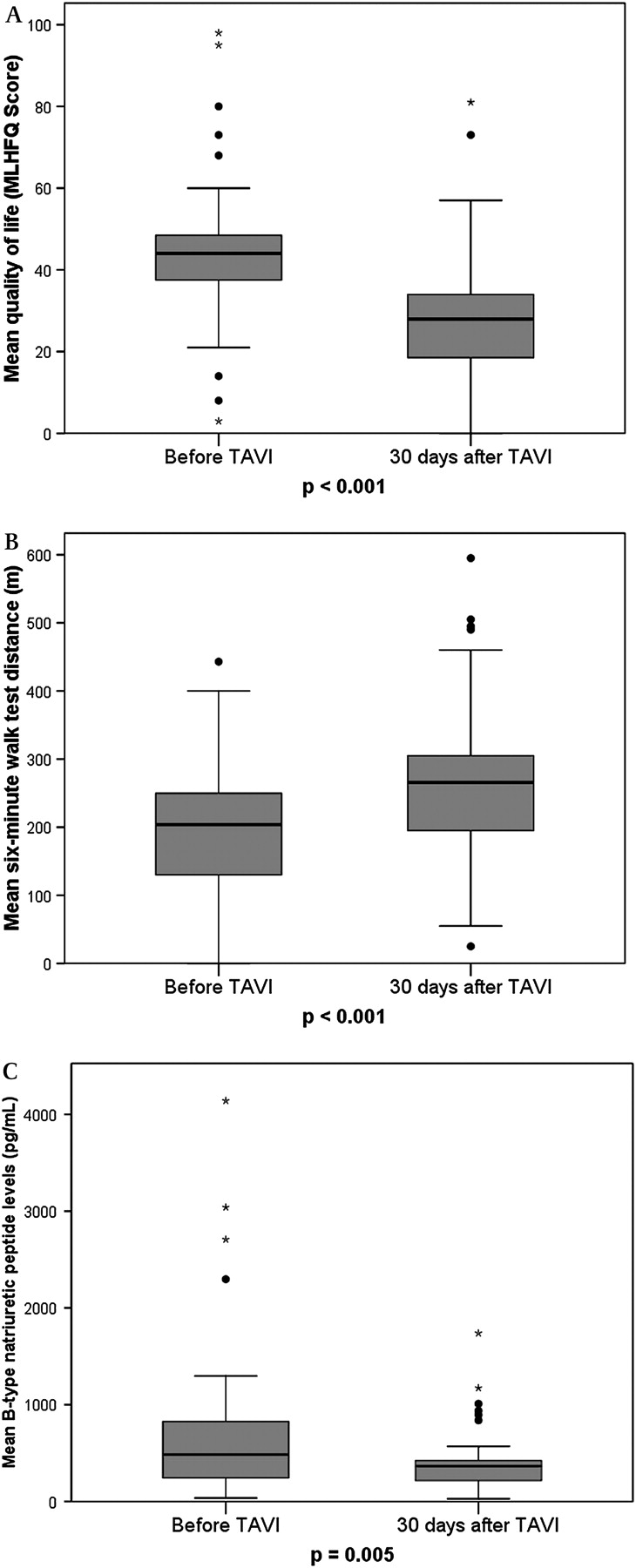
Results In 44 consecutive patients (mean age 79.1±7 years, 50% women, mean left ventricular ejection fraction 55.8±8.5%) TAVI was successfully performed. Follow-up 30 days after TAVI showed a significantly improved quality of life (baseline 44±19.1 vs 28±17.5 MLHFQ Score, p<0.001) and an enhanced distance in the 6-minute walk test (baseline 204±103 vs 266±123 m, p<0.001). B-type natriuretic peptide levels were reduced (baseline 725±837 vs 423±320 pg/ml, p=0.005).
Conclusions Our preliminary results show a significant clinical benefit and a reduction of neurohormonal activation in patients with severe and symptomatic aortic valve stenosis early after TAVI.
- Transcatheter aortic valve implantation
- quality of life
- 6-minute walk test
- B-type natriuretic peptide
- percutaneous valve therapy
- clinical trials
- aortic valve disease
Statistics from Altmetric.com
- Transcatheter aortic valve implantation
- quality of life
- 6-minute walk test
- B-type natriuretic peptide
- percutaneous valve therapy
- clinical trials
- aortic valve disease
Introduction
Aortic valve stenosis is the most common valvular heart disease in industrialised countries. Incidence increases with age and its prevalence rises because of an ageing population.1
During the course of disease, aortic valve stenosis leads to a pressure overload of the left ventricle. Consecutively, increased myocardial wall stress induces concentric myocardial hypertrophy2 and stimulates the release of neurohormones such as B-type natriuretic peptide.3
In severe aortic valve stenosis signs of heart failure may occur such as shortness of breath, angina and syncope. After onset of symptoms, mortality rates increase dramatically.4
The only reasonable treatment of symptomatic aortic valve stenosis is aortic valve replacement.1 However, nearly 30% of patients with severe and symptomatic aortic valve stenosis are not accepted for surgical treatment because of co-morbidities and their high surgical risk.5
Recently, transcatheter aortic valve implantation (TAVI) has been used as an alternative technique for treatment of aortic valve stenosis in patients with an excessive surgical risk.6–8 Moreover, 30-day mortality rates were significantly lower than predicted by established risk algorithms for surgical aortic valve replacement. Additionally, improvement of NYHA functional class early after TAVI has been demonstrated.6–8
However, little is known about other effects of TAVI on clinical symptoms in patients with heart failure due to severe aortic valve stenosis.
Established parameters in treatment of patients with heart failure are assessment of quality of life by means of the Minnesota living with heart failure questionnaire (MLHFQ),9 10 the 6-minute walk test11 and the measurement of B-type natriuretic peptide.12
This prospective study aimed to determine the short-term effects of TAVI on valvular heart failure caused by severe aortic valve stenosis. We hypothesised that shortly after the procedure, TAVI leads to reduced neurohormonal activation, improved clinical symptoms and enhanced functional capacity.
Methods
Patients
From June 2008 to June 2009, consecutive patients with severe and symptomatic aortic valves stenosis (aortic valve area ≤1 cm2) were referred to our department for evaluation of transcatheter aortic valve implantation (TAVI). Risk of surgical aortic valve replacement was estimated with the logistic EuroSCORE.13
The indication for TAVI required the following conditions: (1) symptomatic, severe and native aortic valve stenosis, (2) aortic annular dimensions between 20 mm and 27 mm and an ascending aortic diameter of <45 mm, (3) age≥75 years with a logistic EuroSCORE ≥15% or age>60 years plus at least one additional specified risk factor. Specified risk factors were liver cirrhosis, respiratory failure, pulmonary hypertension, previous cardiac surgery, right ventricular failure and porcelain aorta.8 14
Exclusion criteria for TAVI were: (1) sepsis or active endocarditis, (2) hypersensitivity or contraindication to acetylsalicylic acid or clopidogrel, (3) bleeding diathesis or coagulopathy, (4) recent (<3 months) myocardial infarction or cerebrovascular event, (5) left ventricular or atrial thrombus, (6) previous aortic valve replacement, (7) progressive other disease with expectancy of life <1 year.8
All patients with the indication for TAVI without any exclusion criterion were included in our investigation (n=59). The protocol was approved by the local ethics committee. All patients gave written informed consent before participation.
Quality of life, 6-minute walk test and B-type natriuretic peptide
Clinical investigations of patients were performed within 7 days before TAVI and 30 days after TAVI.
The MLHFQ was designed to measure the effects of heart failure and treatments for heart failure on the individual's physical, emotional, social and mental dimensions of quality of life.9 10 Patients completed in an adaptation of MLHFQ for German-speaking patients. Summation of the responses yielded the total MLHFQ score for each patient. The test ranges between 0 and 110, whereas higher score indicates a poorer quality of life.
The 6-minute walk test was performed according to the guidelines of the American Thoracic Society.11 Patients were instructed to walk quickly for a period of 6 minutes or until dyspnoea or muscular fatigue appeared. The walking course was 30 metres in length. Total walking distance was recorded.
Plasma B-type natriuretic peptide levels (normal value <130 pg/ml) were measured on the same day as clinical investigations. The blood samples were collected in EDTA-containing tubes. After immediate centrifugation, B-type natriuretic peptide was measured using a chemoluminescent immunoassay kit (Biosite Triage, San Diego, CA, USA).
Echocardiography
Echocardiographic studies were performed in all patients within 7 days before TAVI. Follow-up examination was done 30 days after implantation.
Transthoracic echocardiography was performed according to the guidelines of the American Society of Echocardiography15 using a digital ultrasound scanner (Vivid 7, General Electrics, Horton, Norway).
Left ventricular ejection fraction was measured by Simpson method from four-chamber and two-chamber views, by M-mode using the Quinones formula from the parasternal views and by the semiquantitative two-dimensional visual estimate method from different echocardiographic views. Left ventricular ejection fraction values were averaged for each patient.
In the apical five-chamber view peak and mean pressure gradients across the aortic valve were calculated by using the Bernoulli equation. Aortic valve area was measured by means of the continuity equation.
Invasive measurements and transcatheter aortic valve implantation
In 59 patients TAVI was indicated. Five patients died of acute heart failure or sudden death before the intervention.
TAVI was performed in the remaining 54 patients. The aortic valve prosthesis (18-F-generation) (Medtronic CoreValve Percutaneous System, Medtronic CV Luxembourg Sarl) was inserted retrograde without haemodynamic support using a femoral arterial approach (n=50)6 8or using a subclavian arterial approach (n=4) as previously described.16
Immediately before and after implantation, invasive measurements were performed. Aortic and left ventricular pressures were recorded by 5F fluid-filled pigtail catheters connected to a pressure transducer. Invasive measurements comprised aortic systolic and diastolic pressure, peak systolic left ventricular pressure and left ventricular end-diastolic pressure. Transaortic peak-to-peak pressure was calculated by subtraction of aortic systolic pressure from left ventricular systolic pressure. Each measurement was averaged over five cardiac cycles.
One patient died during the procedure owing to rupture of the eccentric calcified aortic base. In two patients, an implantation was not possible for technical and anatomical reasons.
After implantation, six patients died of respiratory failure (n=3) or pump failure (n=3). One patient refused the ambulatory follow-up examination after 30 days.
The remaining 44 patients formed the final study cohort (figure 1).
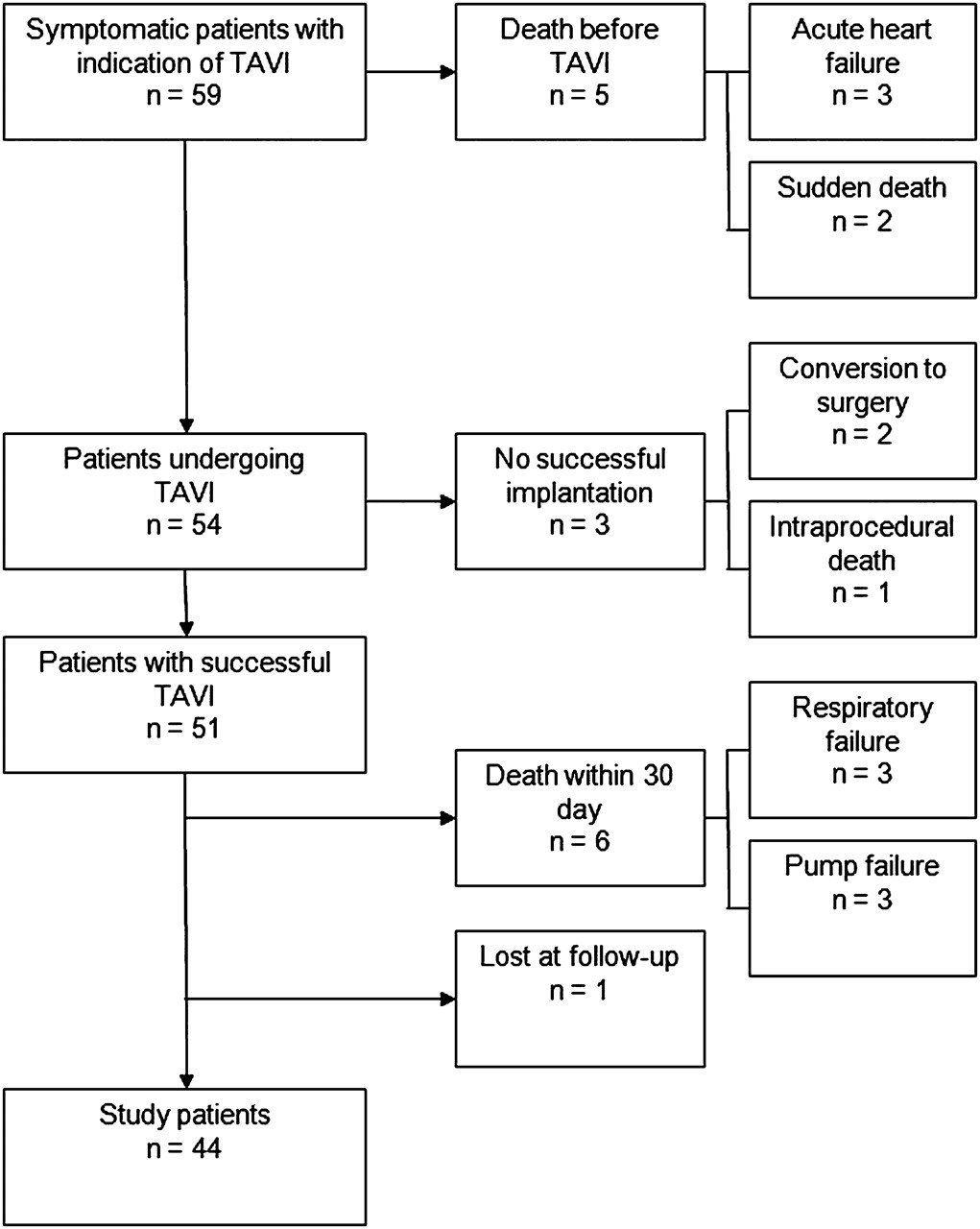
Flow chart presenting all patients with indication for TAVI and the generation of study patients.
Statistical analysis
Numerical values are expressed as mean±SD. Continuous variables were compared between groups using an unpaired t test (for normally distributed variables) or the Mann-Whitney U test (for non-normally distributed variables). χ2 analysis was used to compare categorical variables. Box-and-whisker plots were generated to depict quality of life, 6-minute walk test B-type natriuretic peptide before and 30 days after TAVI. All reported probability values are two-tailed, and p<0.05 was considered statistically significant. Analyses were performed with the SPSS statistical software package (version 17.0).
Results
Patient characteristics
The study patients' baseline characteristics are given in table 1. Mean age was 79.1±7 years. Mean log EuroSCORE was high (18.3±12.4) and co-morbidities were common: 25 patients had coronary artery disease and 15 of them previously survived a myocardial infarction. In 11 patients atrial fibrillation was detected, 17 patients had chronic obstructive lung disease and 24 patients had kidney disease. Kidney disease was defined as a glomerular filtration rate<60 ml/min/1.73 m2 using the abbreviated equation from the Modification of Diet in Renal Disease Study.17
Baseline characteristics of study patients
Changes in haemodynamic parameters immediately after TAVI
Immediately after percutaneous implantation of aortic valve prosthesis, left ventricular peak pressure as well as peak-to-peak pressure decreased, whereas systolic blood pressure increased. Left ventricular end-diastolic pressure slightly decreased (table 2).
Haemodynamic parameters immediately before and after TAVI in study patients
Clinical and echocardiographical characteristics and B-type natriuretic peptide
Before TAVI symptoms of heart failure due to severe aortic valve stenosis occurred in all patients: NYHA class II (n=4), NYHA class III (n=35) and NYHA class IV (n=5). Thirty days after TAVI, NYHA classes improved: NYHA class < II (n=13), NYHA class II (n=24) and NYHA class III (n=7).
Moreover, 30 days after TAVI quality of life showed a significant improvement (figure 2A) and the distance in 6-minute walk test increased (figure 2B). Additionally, B-type natriuretic peptide levels were reduced (figure 2C and table 3).
{kind=link}
{kind=link}
(A) Quality of life (Minnesota living with heart failure questionnaire). (B) Six-minute walk test distance. (C) B-type natriuretic peptide levels in study patients before and 30 days after TAVI (box-and-whisker plot; circles indicate mild outliers, asterisks indicate extreme outliers).
Clinical and echocardiographic characteristics and B-type natriuretic peptide levels in study patients before and 30 days after TAVI
In the echocardiographic examination improvement of haemodynamic properties was observed after TAVI. Aortic valve area increased and aortic valve peak velocity, aortic mean and aortic peak gradient decreased. Concomitant aortic valve regurgitation showed no significant change in degree of severity. However, character of aortic valve regurgitation changed. After TAVI, central aortic regurgitation was seldomly seen (n=2), whereas minor paraprosthetic leaks were common (n=29). Severe aortic regurgitation did not occur after TAVI in our study patients. Concomitant mitral valve regurgitation was not influenced by TAVI. Left ventricular ejection fraction showed a minor but significant enhancement (table 3).
Complications in study patients after TAVI
Acute complications in study patients after TAVI are reported in table 4. A non-fatal pericardial tamponade occurred in one case. One patient had a stroke.
Complications in study patients (n=44)
Vascular surgery (femoral vascular repair) was necessary in six patients. Vascular repair was also needed in four patients in whom a subclavian artery approach was used.
The incidence of new complete heart block or relevant bradycardia associated with new onset of left bundle branch block was high. Therefore, 26 patients received a new permanent pacemaker. Major bleeding or myocardial infarction did not occur in any of the study patients.
Discussion
This prospective study analysed the short-term effects of TAVI in patients with severe aortic valve stenosis on neurohormonal activation and symptoms of valvular heart failure. We employed established parameters which are commonly used to evaluate the efficacy of treatment in patients with heart failure: the MLHFQ,9 10 6-minute walk test 18 19 and measurement of B-type natriuretic peptide.12
The main finding of this study is that TAVI leads to a rapid reduction of neurohormonal activity, an improvement of quality of life and a significantly enhanced functional capacity.
The prevalence of severe and symptomatic aortic valve stenosis increases in ageing population and aortic valve replacement is the only reasonable therapy.1 2 Surgical aortic valve replacement treats symptoms and leads to an improved expectation of life.20 However, in elderly patients co-morbidities are common and owing to their high risk they are often rejected from surgical treatment.5
Recently, TAVI has been implemented in the treatment of high-risk patients with severe aortic valve stenosis.6 Previous studies demonstrated advantageous haemodynamic results early after TAVI.6–8 In our study, these results could be confirmed (tables 2 and 3).
Effects of TAVI on long-term survival are unknown. Several studies demonstrated an improvement of NYHA functional class early after the procedure.6–8 Moreover, one recently published study showed a beneficial effect of TAVI on quality of life, measured by diverse questionnaires21 in 30 patients. Our results are in line with these observations. In our study patients, NYHA functional class decreased significantly after TAVI (table 3). Additionally, quality of life, assessed by means of MLHFQ improved (figure 2A).
The 6-minute walk test is a sub-maximal exercise test and measures the functional capacity.11 Whereas the 6-minute walk test is a common parameter in clinical trials evaluating therapies in chronic heart failure,18 the effects of aortic valve replacement on walking distance are widely unknown. However, even if the results of 6-minute walk test should be interpreted carefully, changes in 6-minute walk test are useful as supportive evidence for symptomatic benefit.19 Our study could demonstrate significant extension of walking distance early after TAVI (figure 2B).
B-type natriuretic peptide is an established parameter for diagnosis, optimisation of treatment and risk stratification in chronic heart failure.22
In aortic valve stenosis, increased myocardial wall stress stimulates the release of B-type natriuretic peptide.3 However, release of this neurohormone also depends on left ventricular ejection fraction and left ventricular end-diastolic pressure.22 Nevertheless, previous studies show the relation between B-type natriuretic peptide levels and the severity of aortic valve stenosis.23 Furthermore, increased B-type natriuretic peptide levels can reflect the onset of clinical symptoms.3 After surgical aortic valve replacement, the increased myocardial wall stress returns to normal and B-type natriuretic peptide levels decrease. It appears that reduction of B-type natriuretic peptide is particularly associated with improvement of clinical symptoms.24
TAVI leads to sudden and almost complete normalisation of pressure-overload of the left ventricle and successively to a reduction of myocardial wall stress. Reduced myocardial wall stress after TAVI was associated with a decrease in B-type natriuretic peptide levels in our study patients (table 3 and figure 2C).
In conjunction with enhanced haemodynamic characteristics, TAVI had favourable effects on neurohormonal activity, quality of life and functional capacity. However, patients' quality of life and functional capacity had improved but were still restricted after TAVI. Moreover, B-type natriuretic peptide levels did not reach normal values.
A possible explanation may be the diverse co-morbidities of patients with indication for TAVI. Particularly, concomitant heart valve disease, chronic lung disease and heart failure had unfavourable influences on B-type natriuretic peptide level, MLHFQ and 6-minute walk test distance.
The results of our study demonstrate the efficacy of TAVI in the treatment of symptoms in severe symptomatic aortic valve stenosis. Furthermore, our data might be helpful in estimating the clinical benefit of patients with planned TAVI. Further studies are necessary to identify patients with expected improvement of symptoms of valvular heart failure.
Limitations
The major limitation of the present study is the small sample size and its monocentric character. However, TAVI is a relatively new procedure and it is realised in few centres only. Therefore, the experience of this procedure is limited and until now only a small number of patients have been treated with TAVI.
Our study population consisted of patients who reached the 30-day follow-up and excluded those patients who died after TAVI. This selection of patients could have an influence on the results of TAVI. Furthermore, it cannot be excluded that a longer sample period might show changes in neurohumoral activity, quality of life and functional capacity. However, this study was designed to evaluate the short-term effect of TAVI. In order to investigate the sustained effect of TAVI, further studies are necessary.
Moreover, our study population was not matched by a control group. A placebo group or a comparison with patients undergoing surgical aortic valve replacement could prove the specific effects of TAVI. Whereas a blinded study does not seem feasible because of ethical concerns, a comparison with surgical treatment would require a broadened indication of TAVI for patients with less severe EuroScores.
Acknowledgments
The authors thank Mrs B Rose for help in organisation and realisation of the study.