Article Text

Abstract
Objective: To determine the effect of education and other measures of socioeconomic status (SES) on risk of acute myocardial infarction (AMI) in patients and controls from countries with diverse economic circumstances (high, middle, and low income countries).
Design: Case-control study.
Setting: 52 countries from all inhabited regions of the world.
Participants: 12242 cases and 14622 controls.
Main outcome measures: First non-fatal AMI.
Results: SES was measured using education, family income, possessions in the household and occupation. Low levels of education (⩽8 years) were more common in cases compared to controls (45.0% and 38.1%; p<0.0001). The odds ratio (OR) for low education adjusted for age, sex and region was 1.56 (95% confidence interval 1.47 to 1.66). After further adjustment for psychosocial, lifestyle, other factors and mutually for other socioeconomic factors, the OR associated with education ⩽8 years was 1.31 (1.20 to 1.44) (p<0.0001). Modifiable lifestyle factors (smoking, exercise, consumption of vegetables and fruits, alcohol and abdominal obesity) explained about half of the socioeconomic gradient. Family income, numbers of possessions and non-professional occupation were only weakly or not at all independently related to AMI. In high-income countries (World Bank Classification), the risk factor adjusted OR associated with low education was 1.61 (1.33 to 1.94), whereas it was substantially lower in low-income and middle-income countries: 1.25 (1.14 to 1.37) (p for interaction 0.045).
Conclusion: Of the SES measures we studied, low education was the marker most consistently associated with increased risk for AMI globally, most markedly in high-income countries.
Statistics from Altmetric.com
In Western countries low socioeconomic status (SES) has been demonstrated to be associated with higher rates of coronary disease.1 2 3 4 5 6 The increase in risk is graded and has been observed for several indicators of socioeconomic position. However, there are at least three limitations to the available information. First, most of the burden of cardiovascular disease is in developing countries; yet, few data are available for the effect of low SES in these populations. Significant variations around the world in the risk of acute myocardial infarction (AMI) associated with level of education have been demonstrated, with the associations between AMI and education varying among regions that are at different levels of socioeconomic development, but these reports are inconsistent.7 8 9 10 11 12 13
Second, SES is a complex construct that represents multiple dimensions; however, studies have generally used a single socioeconomic variable—for instance, education or income.14 This may be a limitation, particularly when considering heterogeneous populations, where the effect of different socioeconomic dimensions could display marked variations. Education is one of the most widely used, having the advantage of being relatively easy to measure, but although education is correlated with income, there is great variation in income at each level of education and, accordingly, these two variables are not interchangeable.14 Therefore, there is a need to simultaneously evaluate multiple measures of SES.
Third, not all studies have evaluated the degree to which other biological or behavioural risk factors may explain the relation between SES and MI risk. The INTERHEART study presents a unique opportunity to overcome some of the limitations identified above. INTERHEART is an international, standardised, case-control study conducted in 52 countries, designed to assess the association of risk factors and AMI across all regions in the world.15 The study measured several risk factors which collectively explained over 90% of the population attributable risk (PAR) for AMI, providing an opportunity to assess the degree to which these risk factors explain the relation between SES and AMI.
The aim of the present analysis is to (1) investigate the potential association of education and other socioeconomic measures on risk of AMI in a multinational population, (2) the extent to which other measured risk factors contribute to explain a tentative relation between education and AMI risk, (3) whether the association between education and AMI varies in different countries based on their economic circumstances.
Methods
Participants
In the INTERHEART study, 12 461 patients with incident cases of AMI from 262 centres in 52 countries representing all geographic regions and 14 637 control subjects free of heart disease were enrolled between February 1999 and March 2003. Centres were requested to recruit consecutive subjects. Patients admitted to the coronary care unit or equivalent cardiology ward of participating centres were screened to identify incident cases of first AMI and enrolled within 24 hours. Details of criteria used for the definition of AMI are provided elsewhere.15 At least one control subject was recruited from each centre and matched to every case subject by age (up to 5 years older or younger) and sex. Eligible control subjects were community based (visitor or relative of a patient from another ward, or an unrelated visitor of a cardiac patient) or hospital based. The ethics committees at each participating centre approved INTERHEART, and participants provided informed consent. For the purpose of the present study we used World Bank classifications for the relevant period 1999 to 2003 (http://web-worldbank.org) to subdivide the 52 countries into high-income, middle-income, and low-income countries (see Heart website for supplementary table 1).
Procedures
Structured questionnaires were administered and physical examinations were carried out in the same way in cases and controls. Information was obtained about demographic factors, SES, and lifestyle factors, including tobacco use, physical activity and dietary patterns with the use of standardised INTERHEART questionnaires. Personal and family patterns of cardiovascular disease (CVD) and risk factors were recorded, and histories of hypertension and diabetes were self-reported. Questions were included about psychosocial conditions to identify depressive mood and psychological stress.16 Weight and height were measured with standardised protocols. Anthropometric measures were obtained in duplicate, by the same examiner, and included height, weight and waist and hip circumferences. Details of blood sampling, storage, transportation and analyses have been published previously.15
The present study is based on 12 242 cases (98.2%) and 14 622 controls (99.9%) with complete data for education. Socioeconomic position was assessed in several ways:
Formal education (predefined options of none, 1–8 years, 9–12 years, trade school or college, university)
Household income defined as predefined country-specific categories (five groups). Ideally, household income would have been assessed as a continuous variable but because this was perceived to be a sensitive issue, the principal investigator from each country defined categories specific for their own country before study initiation
An indication of assets, characterised by objects owned by the household (list of home, car/auto, motorcycle/scooter, bicycle, radio/stereo, television, other land/property, computer, livestock/cattle, other)
Occupation. While detailed responses were recorded, for the purpose of the present analysis, occupation was categorised as general labour, skilled labour, professional and all other. Women were classified according to their own occupation, with homemaker classified among other occupation.
All data were transferred to the Population Health Research Institute, McMaster University and Hamilton Health Sciences, Canada.
Statistical analyses
The statistical methods used in the INTERHEART study have been described.15 Relative risk estimates are reported as odds ratios (ORs) and accompanying 95% CIs using unconditional logistic regression. Generalised linear models (GLM) were used to compute adjusted means and proportions. We used Cochran-Armitage tests for trend and heterogeneity p values were computed based on the test of interaction between each risk factor and the stratifying factor. As previously reported,15 we were not able to find the perfect age and sex matching for about 19% of cases/controls and there was a general agreement for key results among various methods including conditional logistic regression, mixed models and unconditional logistic regression with adjustment for matching criteria. For this reason, we used unconditional logistic regression with adjustment for age and sex instead of conditional logistic regression. The importance of each measure of SES (education, income, assets and occupation) in the prediction of myocardial infarction was assessed in several different ways. In models which adjusted for age, sex and region we investigated the effect on each socioeconomic variable on the risk of AMI. Subsequently, multivariable models were built where, after adjustment for age, sex and region; we separately introduced (a) psychosocial factors (stress, stressful life events, perceived locus of control and depression), (b) biological variables such as apolipoprotein B/apolipoprotein A1 (apoB/apoA1) ratio, hypertension, diabetes, (c) lifestyle factors (smoking, exercise, vegetables and fruits, alcohol consumption, abdominal obesity), (d) all nine factors identified in the INTERHEART study; and, finally, we additionally estimated the OR for each SES variable mutually adjusted for each other. During this process, we explored the interaction between known confounder and risk factors and report as necessary. Fitted models were also assessed using the Hosmer and Lemeshow goodness-of-fit test. In this manner, we sought to establish, first, which of the different set of risk factors explained most of the association between AMI and SES and, second, the independence of each socioeconomic factor. All statistical tests were two-sided. Statistical analyses and graphics were produced with the SAS system version 9.1 and S-Plus version 7.0. PAR were calculated using Interactive Risk Attributable Program version 2.2 (US National Cancer Institute, 2002) and described previously.15
Results
The distribution of risk factors between cases and controls has been reported previously (see Heart website for supplementary table 2); here we focus only on measures related to SES. In the INTERHEART population, the majority, or two-thirds, were derived from middle-income countries, 22% from high-income countries and about 14% from low-income countries (see Heart website for supplementary table 1).
Of the cases, 45.0%, and of the controls, 38.1%, had 8 years of education or less (table 1). Corresponding proportions who were in the lowest two quintiles of their country-specific household income distribution were 52.8% and 49.8%, respectively, and who had two possessions or less, 14.7% and 13.7%. Conversely, 12.7% of cases but 16.5% of controls were in occupations defined as professional.
Frequency for socioeconomic status (SES) variables for cases and controls in the INTERHEART study
Table 2 summarises odds ratios (OR), with 95% confidence intervals, for education, income, possessions and occupation. After adjustment for age, sex and region the OR associated with education 8 years or less, compared with more than 12 years (trade school/college/university) was 1.56 (95% confidence interval 1.47 to 1.66), and for education 9–12 years 1.32 (1.24 to 1.41). Adjustment for, first, psychosocial factors and, second, apoB/apoA1, hypertension, and diabetes did not appreciably change these estimates. However, in a model which adjusted for lifestyle variables (smoking, exercise, daily consumption of vegetables and fruits, alcohol, abdominal obesity) the ORs were reduced to 1.31 (1.23 to 1.40) and 1.19 (1.11 to 1.28), estimates which changed only marginally in a model that included all nine INTERHEART risk factors. Finally, in a model which additionally mutually adjusted for all socioeconomic factors, there was again little change to the estimates for the effect of education, which remained statistically significant (OR 1.31; 95% CI 1.20 to 1.44 for education 8 years or less, and 1.15; 95% CI 1.05 to 1.26 for education 9–12 years).
Odds ratios (and 95% confidence intervals) for acute myocardial infarction (AMI) risk for each of the four methods of measuring socioeconomic status (SES) with six different levels of adjustments
Similar, but lower estimates were obtained for the effect of family income on risk of AMI. With the two highest country-specific fifths of family income as reference, the OR for category 3 compared to the highest income group was 1.17 (1.09 to 1.26), and for category 1 and 2 1.28 (1.21 to 1.37) after adjustment for age, sex and region. These estimates were slightly reduced after adjustment for risk factors, chiefly lifestyle factors. In the final model, adjusted for risk factors, and mutually for other socioeconomic variables the OR for family income in the third quintile was 1.21 (1.10 to 1.32) and for the lowest two quintiles 1.12 (1.03 to 1.23). Having five or more possessions in the family was a protective factor, whereas any type of occupation other than professional was associated with higher risk. However, only weak or non-significant independent effects were evident after adjustment for lifestyle factors, and no significant relation was observed after mutual adjustment for other socioeconomic factors, implying that almost all important information on SES in the present study was contained in education.
The age-adjusted association of education to risk factors in male and female control subjects is shown in table 3. Overall, education demonstrated no, or only minor, associations with apoB/apoA1, blood pressure and self-reported hypertension. Smoking was inversely related to education among men but not women (p for interaction gender—smoking 0.005). All other lifestyle variables—abdominal obesity, consumption of vegetables and fruits, alcohol and exercise—consistently displayed a more adverse pattern in both men and women control subjects with low education, effects that were stronger for women than for men (p for interaction effects <0.0001 to 0.018). Stress at home/work was higher among those with high education, whereas depression was more common among men, but not women, with low education. A high locus of control was consistently, and strongly, associated with high education, in both men and women.
Risk factors by education and gender in control subjects in the INTERHEART study
We defined current smokers as individuals who smoked any tobacco in the previous 12 months and included those who had quit within the past year. Individuals were judged to be physically active if they were regularly involved in moderate exercise (walking, cycling or gardening) or strenuous exercise (jogging, football, and vigorous swimming) for 4 hours or more a week. Regular alcohol use was defined as consumption three or more times a week.
Table 4 shows risk factors by education among controls in high/income, and in low/middle-income countries. Almost all lifestyle variables—smoking, waist-to-hip ratio, consumption of fruit and vegetables and exercise—displayed a more adverse pattern in control subjects with low education, regardless of type of country, with no, or only weak heterogeneity. Regular alcohol consumption was inversely related to education only in low/middle-income countries (p for interaction <0.0001). Severe stress at home/work was higher among those with high education, among controls in low/middle-income countries, but no associations with educational level were found for high-income countries. Conversely, depression was more common in subjects with low education, from both high-income and low/middle-income countries, with a more marked gradient in high-income countries (p for interaction 0.009).
Risk factors by education and type of country in control subjects in the INTERHEART study
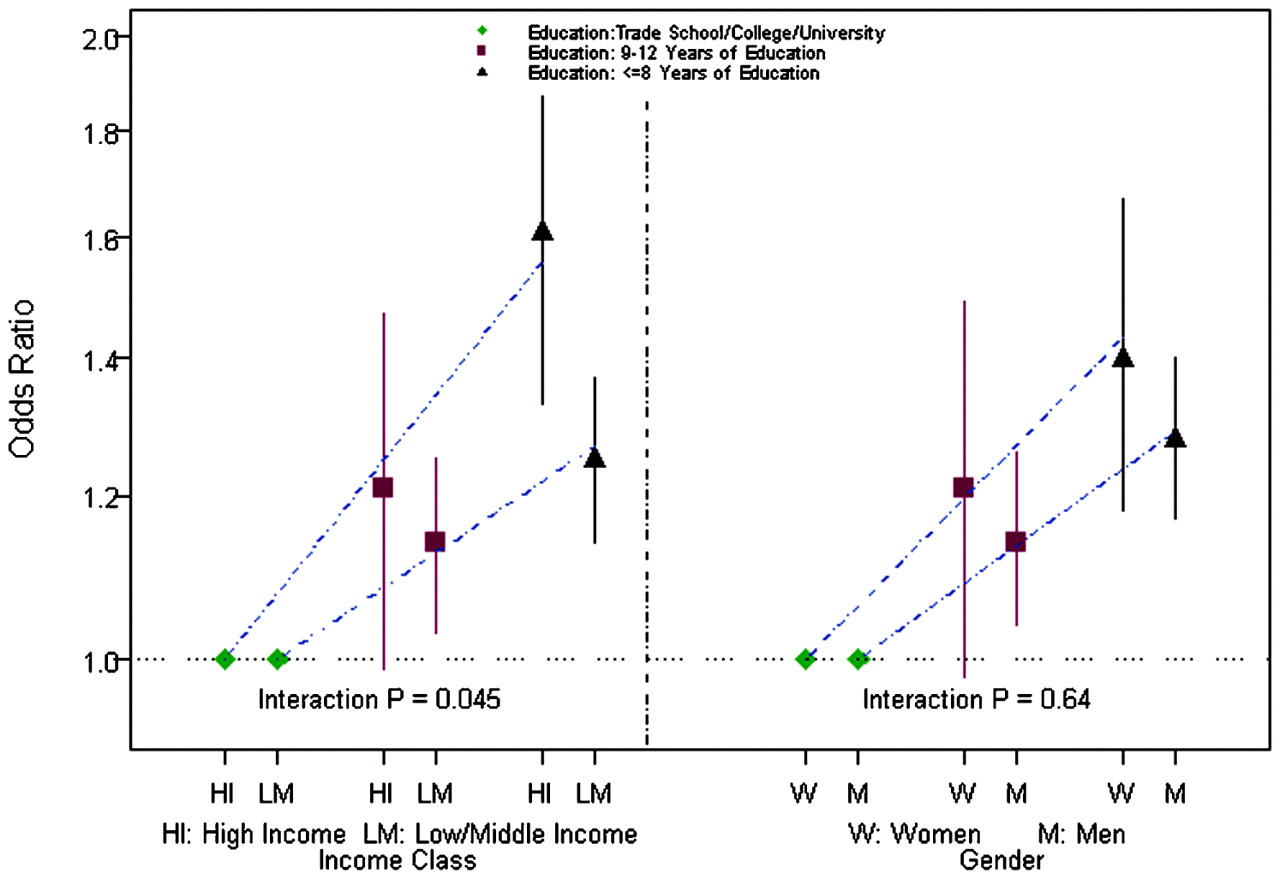
Figure 1 shows the association of education with risk for MI in high-income, versus low-income and middle-income countries, and in men versus women. In models adjusted for age, sex and region, the OR associated with education ⩽8 years, compared to the highest education category, was 1.95 (1.71 to 2.21) in high income, and 1.46 (1.37 to 1.57) in low and middle-income countries (p value for heterogeneity 0.0004). These estimates decreased after further adjustment for risk factors to 1.61 (1.33 to 1.94) in high income and 1.25 (1.14 to 1.37) in low and middle income countries; p for heterogeneity 0.045. The effect of education was stronger in women than in men; age-adjusted and region-adjusted ORs were 2.13 (1.87 to 2.42) for women and 1.43 (1.33 to 1.53) for men; p for heterogeneity <0.0001. However, after further adjustment for risk factors ORs for men and women were not significantly different; p = 0.64.

{kind=link}
Adjusted odds ratios (and 95% confidence intervals), with tests for heterogeneity for risk of acute myocardial infarction for education by (left) type of country and (right) gender.
The fully adjusted ORs associated with low family income (lowest two quintiles vs highest two) was 0.94 (0.75 to 1.18) in low-income, 1.19 (1.07 to 1.32) in middle-income, and 1.07 (0.88 to 1.31) in high-income countries (p for heterogeneity 0.41) (not shown). Similarly, the fully adjusted ORs for five possessions or more, compared to two possessions or fewer were 1.15 (0.90 to 1.47), 1.01 (0.87 to 1.16) and 1.10 (0.85 to 1.42) for low, middle, and high-income countries, respectively; p for heterogeneity 0.71.
In the primary analysis for the INTERHEART study, the PAR associated with nine risk factors, adjusted for age, sex and region was 90.5%. This estimate increased to 92.7% if a composite of education, income, possession, and occupation was entered, reducing the part that was unexplained from 9.5% to 7.3% (that is, by about one-quarter).
Discussion
Of the measures for SES that we studied low education was the marker most consistently associated with increased risk for AMI. About half of the increase in risk associated with low education was due to modifiable lifestyle factors. The effect of education was more marked in high-income countries, compared to low-income and middle-income countries. Income and family possessions exerted only weak, or non-significant, effects when education and other factors were taken into consideration.
There are three unique aspects of INTERHEART. First, this large international study included 52 countries with cases and controls drawn from populations at different economic levels. Second, several measures were available, such as education, income, material possessions and occupation. Third, the study included a large number of cases and controls with extensive data on potentially mediating risk factors and consequently we were able to evaluate the independent impact of SES on MI risk in countries at different levels of economic development.
Of the measures for SES used in the present study, education is the one that is most often used because it is easily obtained and it is also frequently treated as a proxy for SES overall. Which measure best correlates with health outcomes or whether added information is obtained by using several measures simultaneously is not known. We used several measures in the present study and, while they all broadly pointed in the same direction, education best distinguished between cases and controls. It is unclear whether education is inherently the best indicator, or whether education simply integrates many relevant factors including better knowledge and awareness about healthy living. The fact that a substantial fraction of the excess risk associated with low education was explained by modifiable risk factors could indicate that the latter is at least part of the explanation. Given that measures other than education added little, it is unlikely that a composite index of these factors would be significantly superior to education alone as an indicator of SES in most regions of the world.
Income discriminated less exactly than education between cases and controls. Because income was perceived to be sensitive, data on income were only collected as prespecified categories, which will inevitably have resulted in a loss in precision, and an underestimation of the true effect of income. A comparison of the association between deprivation and health between countries would potentially have offered the opportunity to explore whether the effect of deprivation is due to absolute deprivation or relative deprivation. We found, however, no evidence for an interaction effect between type of country and the effect of income, suggesting that relative income levels have consistent effects within and across regions. However, because of the inherent limitations in collecting data on income, these findings must be interpreted with caution.
Findings in the context of the literature
We found a clear variation between the effect of education and countries grouped by their levels of economic development, with a stronger association in the high-income countries than in low-income and middle-income countries. This suggests that, with economic development and increases in the overall level of income of a country, the gradient between the well educated and less educated changes. The findings from the present study underline that associations between AMI and SES are dependent on time and context. Early findings from Western populations observed no associations, or even positive associations,17 18 while inverse associations first were reported based on data from the 1950s and 1960s.19 20 21 22 23
Over the past decades, there has been a growing body of research on socioeconomic inequalities in CVD in Western Europe and the United States, with most studies demonstrating that low SES is a risk factor for coronary disease,1 2 3 4 5 6 however, with significant heterogeneity even within Europe.24 25 By contrast, studies on health disparities affecting the populations of low-income and middle-income countries, where two-thirds of the world’s population reside, are sparse. Higher risks for CVD in groups with higher SES have been reported from Hong Kong, Pakistan and Puerto Rico,7 8 9 whereas in some countries recent socioeconomic gradients resemble those of the West. Also, the inverse association is not consistently observed in developing or transitional countries.12 13
In the present study we found no evidence for higher risk for AMI with increasing SES measured as education in low-income and middle-income countries, but the association was flatter than for high-income countries. There are several potential explanations for this. The most obvious one is that urbanisation and industrialisation already are advanced in the countries that were studied. Our study was confined largely to individuals drawn from urban communities in each country and so the gradients we observed may not necessarily apply to rural regions, especially in low-income countries. Whether the impact of SES on health outcomes varies between urban and rural settings in countries at different economic development levels is currently being studied in the Prospective Urban Rural Epidemiologic study (Yusuf, unpublished data). Further, there may be heterogeneity between SES and health outcomes across different populations within specific countries. For example, the risk for AMI increased with higher income and education in the black African group in the INTERHEART African substudy but the opposite was observed in coloured and white Africans.12
In INTERHEART about half the gradient associated with education could be explained by risk factors, mainly lifestyle factors, and thus amenable to modification. These data suggest that poor diet and lack of exercise lead to markers of the metabolic syndrome, and indicate that the rising burden of obesity-related conditions may disproportionately affect the poor globally. However, a large fraction of the gradient is still unexplained, but whether this represents inadequate estimation of the full impact of lifestyle factors, which are usually measured with some imprecision, is not known. Many studies have reported that socioeconomic differences are only partly accounted for by differences in the distribution of the established risk factors.1 2 3 4 5 6 23 26 Because there are differences in the distribution of risk factors, there has been a debate whether the effect of SES merely reflects these differences, or whether there is an independent effect.27 28 However, as argued by Lynch et al conventional risk factors explain the majority of absolute social inequality in coronart heart disease (CHD) because these risk factors explain the vast majority of CHD cases in the population, even though conventional risk factors do not explain more than part of the socioeconomic gradient.27 In line with this, the PAR only increased from 90.5% to 92.7% when all risk factors were considered.
Dietary and physical activity patterns in the US, Europe, and lower and middle-income countries of the developing world are changing rapidly, with levels of overweight, which is an important factor behind several cardiovascular risk factors, exceeding those of the United States in Mexico, Egypt and South Africa.29 Rapid urbanisation, falling food prices (until recently) and westernisation of diet have contributed to changes in lifestyles and an increase in risk factors, which are rising faster than the historical experience of the West. Countries where the predominant pattern is poverty and high mortality in the young from communicable diseases now represent only a small proportion of the world’s population, indicating that the epidemiological transition is already taking place practically everywhere. Adverse trends in risk factors are now a problem not only for the wealthy.30 Although there is a paucity of data, a review of studies reported between 1989 and 2003 indicates that the burden of obesity tends to shift to lower-income groups as gross national product increases.31 These findings are consistent with the present analyses from the INTERHEART study.
Limitations
There are a few limitations of our study. First, our data cannot be taken as being nationally representative for any country, and so this study should be viewed as an indicator of the potential variations in the relation between SES and MI that can exist in different settings. In addition, years of education does not necessarily mean the same across 52 countries, with different educational structures and opportunities. It is, however, likely that contrasts will be greater in low-income countries. A third potential limitation is whether recall biases could have influenced our results. We believe that this is unlikely because we used measures of SES (for example, education) that should not be affected by different recall by cases and controls, and neither subjects nor staff recording the data had any preconceived notions of what the associations were likely to be in each country. Selecting controls who were either patients or attendants in the same centre means that there is a degree of matching on SES in terms of ability or likelihood of attending that hospital. Another potential limitation is that only surviving cases could be investigated. Overall, there were 433 fatal cases in the study. The case fatality for those in the highest two education categories was just above 2%, whereas among those with 8 years of education or less it was 5%. Therefore, it is likely that the true influence of education on AMI was underestimated in the present study. Additionally, the relatively limited data collected on income may have attenuated the relation of income, compared to education.
What is already known on this topic
In Western countries low socioeconomic status has been demonstrated to be associated with higher rates of coronary disease.
Socioeconomic status is a complex construct that represents multiple dimensions; however, studies have generally used a single socioeconomic variable—for instance, education or income
Few data are available for the effect of low socioeconomic status in populations from the developing countries despite the fact that most of the burden of cardiovascular disease is in these countries.
What this study adds
Low education was the socioeconomic status marker most consistently associated with increased risk for acute myocardial infarction in this study which comprised 52 countries.
About half of the increase in risk associated with low education was due to modifiable lifestyle factors.
The effect of education was more marked in high-income countries, compared to low-income and middle-income countries, probably reflecting different stages in the epidemiological transition.
Conclusion
In the INTERHEART study low education was the socioeconomic status marker most consistently associated with increased risk for AMI. About half of the increase in risk associated with low education was due to modifiable lifestyle factors. The effect of education was more marked in high-income countries, compared to low-income and middle-income countries, probably reflecting different stages in the epidemiological transition. These findings suggest that improving education levels has the potential to partially prevent the rising epidemic of CVD in developing countries, as it could lead to healthier lifestyles. Our study will hopefully stimulate larger and more targeting studies that will explore these associations involving a wider range of both urban and rural communities in countries selected by their overall status of economic development.
Acknowledgments
SY initiated the INTERHEART study and supervised the project, data analysis and writing of the report. AR had main responsibility for writing the report. SI did all data analyses and reviewed and commented on drafts. SVS was involved in the design and, along with SR and CKC, assisted in interpretation and writing the manuscript. KS, MZ, AA and KK coordinated the study in their respective countries and made significant contributions to the manuscript. The authors had full access to and take full responsibility for the integrity of the data. All authors have read and agree to the manuscript as written. AR is the guarantor.
REFERENCES
Footnotes
▸ Additional tables are published online only at http://heart.bmj.com/content/vol95/issue24
Funding SY was supported by a senior scientist award of the CIHR and holds an endowed chair of the Heart and Stroke Foundation of Ontario. CKC is supported through a Cottrell scholarship, Royal Australasian College of Physicians and a Public Health (Sidney Sax) Overseas Fellowship cofunded by NHMRC and NHF of Australia. SVS is supported by the National Institutes of Health Career Development Award (NHLBI 1 K25 HL081275). The INTERHEART study was funded by the Canadian Institute of Health Research, the Heart and Stroke Foundation of Ontario, the International Clinical Epidemiology Network (INCLEN) and through unrestricted grants from several pharmaceutical companies, with major contributions from AstraZeneca, Novartis, Hoechst Marion Roussel (now Aventis), Knoll Pharmaceuticals (now Abbott), Bristol Myers Squibb, King Pharma and Sanofi-Sythelabo, and by various national bodies in different countries: Chile: Universidad de la Frontera, Sociedad Chilena de Cardiologia Filial Sur; Colombia: Colciencias, Ministerio de Salud; Croatia: Croatian Ministry of Science and Technology; Guatemala: Liga Guatemalteca del Corazon; Hungary: Astra Hassle, National Health Science Council, George Gabor Foundation; Iran: Iran Ministry of Health; Italy: Boehringer-Ingelheim; Japan: Sankyo Pharmaceutical Co, Banyu Pharmaceutical Co, Astra Japan; Kuwait: Endowment Fund for Health Development in Kuwait; Pakistan: ATCO Laboratories; Philippines: Philippine Council For Health Research and Development, Pfizer Philippines Foundation, Astra Pharmaceutical, and the Astra Fund for Clinical Research and Continuing Medical Education, Pharmacia and Upjohn; Poland: Foundation PROCLINICA, State Committee for Scientific Research; Singapore: Singapore National Heart Association; South Africa: MRC South Africa, Warner-Parke-Davis Pharmaceuticals, Aventis; Sweden: Swedish Heart and Lung Foundation, the Swedish Council for Working Life and Social Research; Thailand: The Heart Foundation of Thailand, Thailand Research Fund; USA: King Pharma. Role of the study sponsors or funders: in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication: none. Researchers were independent from funders.
Competing interests None.
Ethics approval The protocol was approved by the ethics committee at each of the participating centres and all participants provided written informed consent.
Provenance and Peer review Not commissioned; not externally peer reviewed.