Article Text

Abstract
Diabetes is an increasing problem in sub-Saharan Africa. Type 2 diabetes, the most common form, is becoming more prevalent owing to rising rates of obesity, physical inactivity and urbanisation. Type 1 diabetes exists in two major forms in the region: type 1A or autoimmune and type 1B or ketosis-prone type 2 diabetes. At present there are scanty epidemiological data on either. The current morbidity of diabetes is primarily due to the high rates of microvascular complications, while macrovascular complications, once rare, are becoming more common, particularly in the urban setting. Further, despite the HIV epidemic, the total number of people with diabetes in the region is expected to grow because of changing demography. A concerted multisectoral effort will be critical to ensuring improvement in healthcare delivery for people with diabetes in the region.
Statistics from Altmetric.com
Diabetes, an important component of the non-communicable diseases, is undoubtedly a rising problem globally. Sub-Saharan Africa is not immune to the process, and is experiencing a triple and in many instances, a quadruple burden of disease, as the traditional infectious diseases such as malaria and tuberculosis have been joined by non-communicable diseases in addition to HIV. In certain countries high levels of trauma and violence contribute further to the burden of disease.1 All this occurs in a region in which over 40% of the population live on <US$1/day,2 and in which the epidemiological transition is occurring rapidly, often accompanied by tremendous social and political upheaval. Sub-Saharan Africa, however, is not homogeneous and countries are clearly at different stages of this transition.
Against this backdrop, the current review focuses on the scope of diabetes in the region, the different forms of diabetes and macrovascular complications encountered, and finally, the challenges and barriers to the provision of optimal healthcare for diabetes. The review concentrates on these topics as they relate to the indigenous African population, overwhelmingly the majority of the population throughout sub-Saharan Africa. It is perhaps pertinent to note that a number of authors have proposed that diabetes be used as a tracer for the other burgeoning chronic diseases, because it is well defined, fairly easy to diagnose and common.3
The sources of information were based on a Medline search using key words including: diabetes, Africa, prevalence, healthcare, mortality and healers. The World Health Organization (WHO), International Diabetes Federation (IDF) and World Bank websites were also explored for relevant information.
EPIDEMIOLOGY
Type 2 diabetes is the predominant form of diabetes in sub-Saharan Africa, accounting for over 90% of cases. Type 1A or autoimmune type 1 and type 1B or idiopathic or alternatively ketosis-prone type 2 diabetes constitute the remainder.
Type 2 diabetes
Prevalence
The WHO estimated that there were 135 million people in the world with diabetes in 1995 and that this would rise to 154 million in 2000.4 The most recent IDF Atlas (2006) pointed to an even greater current and future problem by calculating that, at present, diabetes affects 246 million people world wide, with a projected rise to 380 million by 2025. Each report has highlighted the fact that low- and middle-income countries will bear the brunt of the increase and that Africa will contribute significantly to this rise. The IDF Atlas estimated that 10.8 million people have diabetes in sub-Saharan Africa in 2006 and that this would rise to 18.7 million by 2025, an increase of 80%, as such exceeding the predicted worldwide increase of 55%. Indeed, while the HIV epidemic has captured the world’s attention, recent data indicate that the global mortality due to diabetes and HIV are similar.5 Furthermore, whereas the trends for a rise in diabetes prevalence are clear, globally and regionally, there is less certainty for HIV.6
Historically, studies on the epidemiology of diabetes in sub-Saharan Africa have been restricted to a small number of countries, although the WHO STEPwise Chronic Disease Risk Factor Surveillance Programme is beginning to rectify this. Much of the information is not in yet in the public domain, but when available, will provide a much clearer picture of the true extent of diabetes in the region. Until about 40 years ago, diabetes was considered rare in sub-Saharan Africa. The reported prevalence, using predominantly urine analysis, in localised settings in a number of countries including Ethiopia, Ghana, Lesotho, Uganda and Malawi between 1960 and mid-1985, was <1%. There were two exceptions, Ivory Coast (5.7%) and South Africa (2.2–2.7%).7 8 The low prevalence (table 1) was still evident in rural and urban Eastern and Western Africa when standardised WHO criteria for the diagnosis of diabetes were applied to cross-sectional studies from ∼1985 to 1995.7 9–11 In contrast, moderate prevalences were reported from South African studies undertaken in different cities and one peri-urban area (4–8%).12–14 These differences could be largely ascribed to considerably higher rates of obesity in the South African population compared with other countries in the region. More recently, there has been a clear demonstration that the prevalence of diabetes is rising in the region. In Tanzania and Cameroon, the only two countries where repeated local surveys have been undertaken using similar methodology, the prevalence has increased six- to 10-fold within a 10-year period (http://www.who.int/chp/steps/STEPS_Cameroon.pdf (accessed 22 July 2008)).15 These data together with a further gradient evident in prevalences derived from the African Diaspora indicate that steps need to be taken to stem the tide of rising diabetes in the region.16
Risk factors
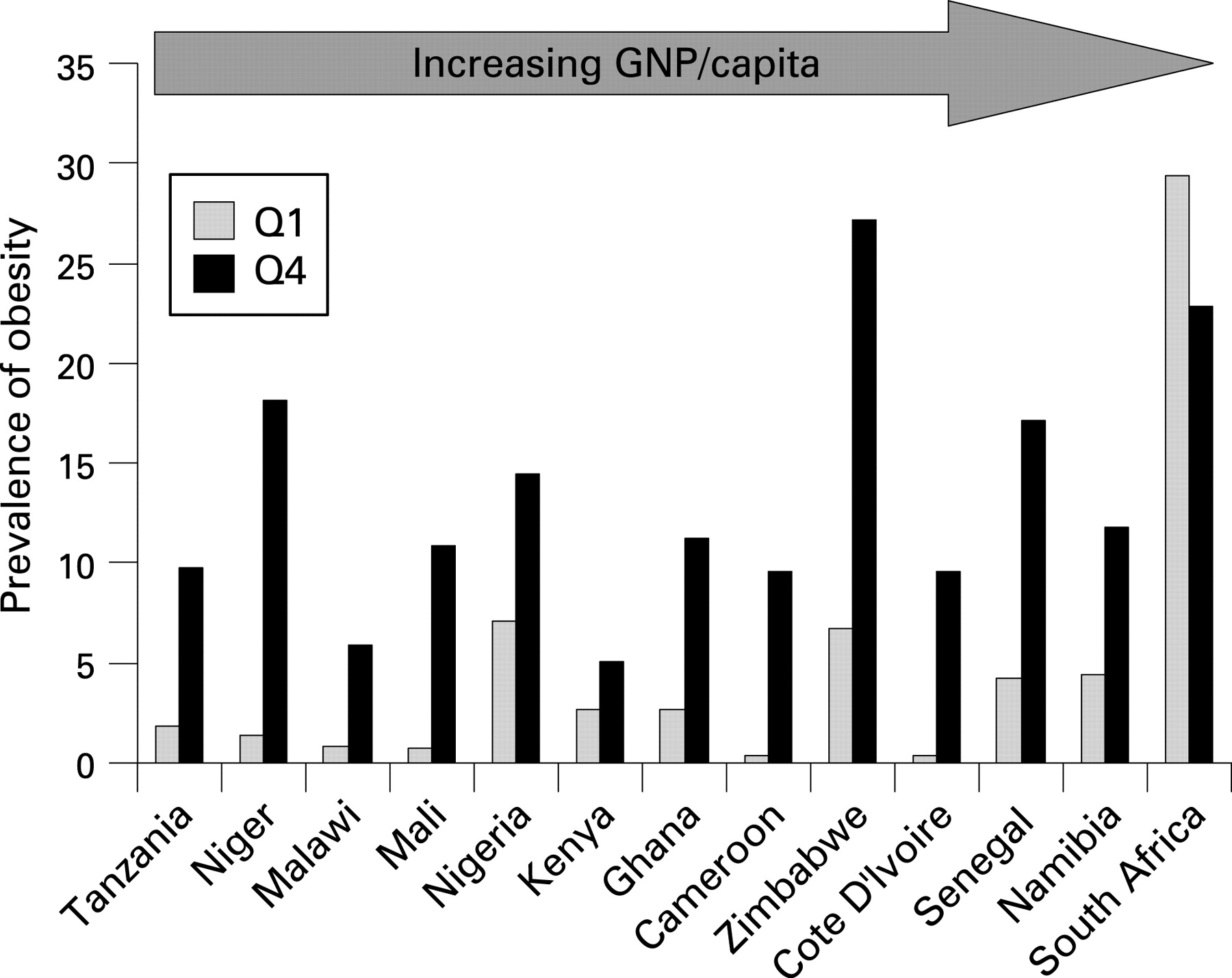
The major risk factors for diabetes in sub-Saharan Africa are similar to those in other regions of the world, whether this refers to the modifiable risk factors, such as urbanisation, obesity, physical inactivity, or those that are not mutable, such as increasing age and ethnicity. The rising prevalence of diabetes in the region has largely been ascribed to changes in lifestyle and urbanisation, resulting in greater levels of obesity and physical inactivity. However, obesity has traditionally been uncommon in many parts of the region, largely owing to scarcity of food and high levels of energy expenditure.17 18 As recently as 1995 only 1–7.1% of women aged 15–45 years of age in 18 sub-Saharan Africa countries were obese (body mass index (BMI) >30 kg/m2); Namibia and Zimbabwe alone had a prevalence of more than 5%.19 Yet at the same time, 31% of South African women were obese, even exceeding the 20.7% reported in US women.17 19 Given the marked fourfold difference in obesity between rural and urban areas, the strong relationship between level of education as a marker of socioeconomic status and obesity within countries with low gross national product (although this seems to fall away in countries with higher gross national product; fig 1)17–19 and the extent of urbanisation projected by 2025, suggesting that 70% of Africans will reside in cities at that time, increasing rates of obesity can be expected in the region. This in turn will fuel the rise in diabetes prevalence as obesity, expressed by BMI or centrally by waist circumference or waist:hip ratio, has been consistently an independent risk factor for diabetes in the region.12 15

{kind=link}
Cultural perceptions of body size may well hinder measures to reduce rates of obesity, which is an important concern. A larger body size has many positive connotations in black rural communities and similarly, in some groups of urban black women, a larger body size may be associated with affluence, health, attractiveness and happiness. Black African women also generally experience less pressure from male partners, family and friends to be thin.20 Further, there is a stigma attached to the syndrome of weight loss and wasting associated with HIV/AIDS21; however, some evidence indicates that cultural perceptions of body size may be changing, and that women may be willing to reduce their body size for improved health and social reasons.22 Nevertheless, much work still needs to be done in this area.
An additional factor in sub-Saharan Africa may well have an impact on rates of obesity and diabetes—the evidence that adverse events in early life are associated with an increased risk for obesity, diabetes and other chronic diseases in adults.23 Undernutrition is a common problem in children of the region. Rates of stunting varying from 20% to 40% have been reported in children <5 years of age.24 To compound the problem, stunting confers a two- to sevenfold risk for being overweight, even in children. Indeed the deleterious effects of weight gain in children with low birth weight on insulin sensitivity were already demonstrable in 7-year-old South African children in the birth to age 10 cohort.25
In contrast to the ease with which obesity can be ascertained in field studies, it has been difficult to measure physical activity with any degree of reliability in such studies, owing to the lack of standardised and validated methods. Consequently, few reports have been able to identify physical inactivity as a risk factor for diabetes in sub-Saharan Africa. Despite this, Sobngwi et al were able to show an inverse relationship between fasting glucose concentrations and energy expenditure.26 Thus physical inactivity, a consequence of urbanisation, due to changes in modes of work and transport from rural areas,27 is also expected to play a role in the increasing diabetes prevalence.
Further to this, in African countries for which there are reasonably representative data, physical inactivity has been linked to obesity, with this association being at least partially explained by economic development.28 Utilisation of the validated Global Physical Activity Questionnaire with the WHO STEPwise surveillance programme in the region is likely to redress the lack of comparative data on physical activity.
Investigation of the genetic determinants for type 2 diabetes in sub-Saharan Africa has received some attention, particularly through the Africa American Diabetes Mellitus (AADM) study, which is conducting a genome-wide search for susceptibility genes for diabetes in West Africans.29 This group has recently identified four major genetic loci (10q23, 4p15, 15q14 and 18p11) which influence C-peptide concentrations in West Africans with type 2 diabetes.30
Impact of HIV/AIDS
We cannot view the regional burden of diabetes in isolation. According to the UNAIDS 2006 report, sub-Saharan Africa is not only home to 63% (24.7 (21.8–27.7) million) of all people infected with HIV world wide, the region also accounts for the majority of deaths globally (72%, 2.8 (2.4–3.2) million), placing it at the centre of the global HIV epidemic.31 Although there is evidence that the spread of HIV is stable or diminishing in the bulk of East and West African countries, the same cannot be said for Southern Africa, which in any case accounts for the majority of cases of HIV. Unsurprisingly, given the extent of the HIV epidemic, the peak age-specific incidence of 20–40 years and the almost complete absence of antiretroviral therapy programmes in the region, a large premature mortality has been observed. In South Africa, for example, which is worst hit, the mortality rate for young women has risen fivefold and in men twofold.32 As a consequence, the number of people reaching the age of peak incidence of diabetes (>40 years) would be expected to fall, as would the population growth rate.
We have previously modelled the impact of the HIV epidemic on the burden of diabetes, but this was limited to South Africa. The analysis also examined the projected impact of the epidemic on the number of people with known diabetes who would be expected to use the health services in 2010.33 Despite a reduction in projected population growth rate between 1995 and 2010 of 1.8% to 1.3%, the analysis indicated that the number of people with diabetes can be expected to grow, merely as a consequence of the continued expansion (albeit at a lower rate) and ageing of the population.
The projected total number of people with diabetes in South Africa would be 1 340 000 in a situation of no rise in diabetes prevalence, 2 015 000 with a 50% rise and 2 631 000 with a 100% rise. The respective projected numbers of people with diabetes seeking medical care (patient load) would be 677 000, 1 008 000 and 1 316 000, respectively. Based on these data, there will be increasing numbers of people, who will not be infected by HIV and who will live long enough to develop diabetes and in turn require medical care. It is likely that these analyses are conservative: they did not take into account the potential impact of antiretroviral therapy on population growth rates, or the possible rise in diabetes incidence on antiretroviral therapy.34 Similar analyses undertaken in other sub-Saharan Africa countries with different rates of HIV infection and diabetes prevalence would provide a more complete picture in the region.
Type 1 diabetes
Little is known of the epidemiology of type 1 diabetes in sub-Saharan Africa. Two studies, one from Sudan and the other from Nigeria, both reported a low prevalence in populations of schoolchildren. Elamin et al reported a 0.95/10 000 prevalence after screening 42 981 schoolchildren aged 7–14 years from Khartoum, Sudan,35 while Afoke et al found a prevalence of 0.33/100 000 when they screened 77 862 Igbo schoolchildren aged 5–17 years from Eastern Nigeria.36 Two further studies have documented incidence rates, but these show marked differences. In Khartoum Elamin et al reported an incidence of 10.1/100 000/year in 1990 in children aged <15 years, which was higher than that found in the Middle East at that time.37 In contrast, Swai et al found a lower incidence of 1.5/100 000/year in children/young adults aged <19 years in Dar es Salaam, similar to the incidence in some African heritage populations in the Caribbean.38 The widely differing rates in Sudan and Tanzania may reflect methodological differences, underascertainment in Tanzania or true ethnic differences; the Tanzanian population are of African origin whilst the Sudanese are of mixed Arab and African origin.
The phenotype of indigenous African children and youth with type 1 diabetes does appear to differ from those of European extraction. Insulinopenia is present, but the peak age of onset is later, at 15–19 years in Tanzanians and up to a decade later at 22–23 years in indigenous South Africans, although they also demonstrated a smaller peak at 12–14 years of age.38 39 When type 1 diabetic patients with an older age of onset are included, islet cell autoantibodies, characteristically found in European type 1 diabetic patients at diagnosis with reducing occurrence as duration increases, are considerably less common: 8–11% in newly diagnosed type 1 diabetic patients from Tanzania and 30–44% in patients from Cameroon and South Africa, albeit with a longer duration of disease.7 40
Genetic susceptibility
There are some similarities in HLA susceptibility loci with reports from Caucasian populations, particularly with HLA-DR3, HLA-DR4 and HLA-DR3/DR4 heterozygosity, but there are population differences for many alleles and haplotypes.8 40 41 More recently, additional evidence has emerged of an autoimmune basis of type 1 diabetes in indigenous Africans. An association between a polymorphism (C159G) of CTLA4 (cytotoxic T-cell-associated antigen-4), a gene known to encode the T-cell receptor responsible for T-cell proliferation and apoptosis was found in West African children with type 1 diabetes and the presence of at least one islet cell antibody.42 Additionally, Pirie et al found an association between type 1 diabetes and intron 3 of the toll-like receptor 3 in subjects of Zulu descent.43
Ketosis-prone type 2 diabetes or type 1B diabetes
An atypical form of diabetes has been recognised in Africa since the 1970s; notably, patients who presented in ketoacidosis without an obvious precipitating cause, in whom insulin could be withdrawn safely over weeks or months, whose disease could be safely managed with oral agents or diet alone and in whom islet cell autoantibodies were absent.7 40 44 45 Phasic insulin requirements were also described. It has been estimated that up to a half of younger patients initially treated with insulin and assumed to have type 1 diabetes may have this atypical form. Careful clinical studies conducted primarily in African Americans and people of sub-Saharan Africa origin in France have provided detailed characterisation46–48: presentation in ketoacidosis, strong family history of diabetes, older age at onset, male predominance, higher BMI at diagnosis, absence of islet cell autoantibodies and lack of HLA association. It seems that this group may be further subdivided into a small number who remain dependent upon insulin and a larger group who experience periods of normoglycaemia, interrupted by episodes of hyperglycaemia, ketosis and phasic insulin requirements. The former are leaner at diagnosis, tend to require almost twice as much insulin at discharge and demonstrate a faster loss of residual β-cell function than the latter, but even at 10 years after diagnosis maintain higher C-peptide responsiveness to glucagon than patients with type 1 diabetes. The latter group on the other hand have a greater decline in insulin secretory capacity over time than controls and their ketotic relapses have been attributed to a temporary functional abnormality of the β cells induced by glucotoxicity. Obesity too seems to play a role particularly in the latter form. It generally occurs in people who are overweight and the initial and subsequent episodes of ketosis are preceded by a progressive rise in weight.
Genetic susceptibility
Genetic susceptibility to ketosis-prone type 2 diabetes is under investigation. Thus far, functional gene variants in the β-cell transcription factor PAX4 have been found to predispose to the disease in a subset of patients, while a high prevalence of glucose-6-phosphate dehydrogenase (G6PD) deficiency without G6PD mutations has also been found subjects with severe insulin deficiency.48 49
Other types of diabetes
Malnutrition or fibrocalculous diabetes was frequently reported from tropical areas in Africa, Asia and South America in the 1960s and 1970, but seems to be almost unheard of today. It was recognised by a history of poor nutrition and chronic pancreatitis, with pancreatic calcification in the vast majority in addition to diabetes and exocrine pancreatic dysfunction.7 8
MORBIDITY
Microvascular complications are highly prevalent owing to poor levels of glycaemic and blood pressure control so commonly noted in the region. Furthermore, these complications are found early in the course of the disease as diagnosis of diabetes is often delayed.50 Foot complications are a prime example of the morbidity and often premature mortality associated with these complications. In Tanzania, Abbas and Archibald found that patients present to hospital late once gangrene has developed or severe sepsis has set in, resulting in high mortality.51 Nephropathy too is a major problem given that dialysis and transplantation are almost completely inaccessible to all but the few who can afford private medical insurance or who are accepted onto the limited programmes available in the larger urban tertiary hospitals.52
Macrovascular disease
The prevalence of ischaemic heart disease (IHD), previously almost unknown in patients with diabetes, is now increasing in diabetic patients in sub-Saharan Africa, probably owing to westernisation of lifestyles. IHD currently, however, remains substantially less common (5–8% based on ECG stress tests and 4% based on history) in indigenous African diabetic patients than in diabetic patients of European heritage (23% based on positive history). This is because rates of the traditional risk factors are not yet at the same level, with the notable exception of hypertension, or present for the same duration of time.53–55 When coronary artery disease occurs, however, the rates of the traditional risk factors no longer differ and renal disease imparts an additional risk in the indigenous Africans.54 Of some concern is the finding by Ntyintyane et al that undiagnosed diabetes was present in 20% of indigenous Africans with angiographically proven coronary artery disease.56
There are scanty data on the frequency of stroke among diabetic patients in the region, with early reports suggesting that it is low. For example, only 1 of 221 diabetic patients attending the main hospital in Addis Ababa in 1986 had a stroke.57 Known diabetes was present in 2.8% of patients presenting with a stroke in rural Tanzania and at a referral hospital in The Gambia,58 59 but higher rates have been found in Mauritania, where 8% of patients with acute stroke had diabetes and in rural South Africa in 2001, 11.7% of 103 people with strokes had diabetes.53 60 These limited data show that the prevalence of cerebrovascular disease seems to match that of IHD in diabetic patients of the region.
The prevalence of peripheral vascular disease (1.7–28%) is dependent on the method of detection. When the absence of foot pulses is used, the prevalence is 4–8% but is substantially higher, 18–28%, when Doppler ultrasound examinations are performed.53
MORTALITY
Directly assessed mortality due to diabetes in sub-Saharan Africa has not been well documented. Table 2 shows data from studies reported since 1990. Similar 20-year survival rates in type 1 diabetic patients were found in Soweto, South Africa (57%) and Addis Ababa, Ethiopia (63%) as well as in African-American type 1 diabetic patients from Pennsylvania USA (60%).7 61–62 These mortality figures remain unacceptably high, although an even higher mortality (60% at 5 years) was found in a large group of insulin-requiring, presumably type 1 diabetic patients from Dar es Salaam, Tanzania about 16 years ago.64 The major cause of death in the Soweto study was renal failure, highlighting the lack of access to renal replacement treatment for people with diabetes in this region.63 Yet, acute metabolic emergencies, entirely preventable with good medical care, not requiring sophisticated or expensive equipment, were the major cause of death in the other two studies. Beran et al recently estimated that life expectancy varied from less than a year for a child with type 1 diabetes in rural Mozambique to 27 years for an adult in Lusaka, Zambia. Mortality rates in type 2 diabetic patients have received little attention.65 The only cohort data come from Dar es Salaam, and demonstrate much lower rates than for type 1 patients, but poorer than for those with an indeterminate type of diabetes.7 64
A number of global studies have attempted to ascertain the true extent of mortality due to diabetes. This is a difficult task because most mortality statistics are based on the recorded underlying cause of death on death certificates and in the case of diabetes, the associated renal or cardiovascular diseases are commonly documented, rather than diabetes itself. Additionally, many countries have a poor collection of even this information. When Roglic et al took this into consideration, diabetes rose from the eighth to the fifth leading cause of death globally for the year 2000 with an excess mortality of 2.9 million deaths which accounted for 5.2% of all deaths.5 The estimates for sub-Saharan Africa were amongst the lowest for all regions; diabetes accounting for 2.2% of all male deaths and 2.5% of all female deaths—that is, 142 500 men and 152 100 women. An analysis for South Africa, however, estimated that 4.3% of all deaths for that country in 2000 could be attributed to diabetes, probably reflecting the fact that South Africa is further along the epidemiological transition than many other sub-Saharan Africa countries.66
CHALLENGES TO HEALTHCARE AND MANAGEMENT
It is not surprising that healthcare delivery for people with diabetes in the region is inadequate and in many cases frankly poor.67 68 Limited resources are allocated to health in countries with such low-income economies and the needs consequent upon the multiple burden of disease are considerable. Yet even in this context, diabetes and the non-communicable diseases remain low on the list of priorities.
The challenges and thus solutions to the provision of healthcare that would improve outcome for diabetes in the region are many and can be found at multiple levels.67 69 70 Health systems plan care around the needs for acute and not chronic care, there are inadequately trained staff, a lack of guidelines and policies for diabetes care, drugs are unavailable, functioning equipment for routine monitoring is often not in place, healthcare facilities are not easily accessible in all areas and there are few education programmes for both patients and staff. In many countries medication and self-monitoring have to be paid for by the patient. This has resulted in a situation in which poor glycaemic control, inadequate levels of blood pressure control and lack of screening for complications are rife.
Throughout the region, with some notable exceptions such as Namibia and South Africa, payment for medication is the responsibility of the patient and unfortunately drug costs for diabetes are beyond the reach of many, particularly for those requiring insulin. In Ethiopia, for example, the mean annual expenditure of diabetes care for a child accounted for 65% of family expenditure on health, insulin needs consumed 36% of this amount.71 In other countries such as Zambia and Mozambique, insulin is on the essential drug list, but there are problems with supply and distribution. In addition, the annual cost of purchasing insulin to the health service is ∼40 times the national annual drug expenditure per person.65
Patient-related factors are also extremely important. These range from low levels of self-management practices, lack of adherence to lifestyle changes and medication and lack of faith in the biomedical model. Many African populations still regard alternative healing systems as the primary source of healthcare or, alternatively, consult both. Traditional or folk healers usually promote the concept that diabetes is curable and have been found to be reluctant to refer clients to medical practitioners.68 72 In a recent detailed study from Ghana, for example, biomedical management was the preferred first choice for diabetic patients from rural and urban areas.73 This, however, was undermined by two key factors; the high cost of drugs and recommended foods as well as the psychosocial burden imposed by the daily therapeutic routines. Spiritual causal theories of diabetes such as sorcery and witchcraft are still found in the region, particularly in rural communities, although these have largely been replaced by biomedical theories in urban residents.
Box 1 Unanswered research questions on diabetes in Africa
What is the epidemiology of type 1 diabetes in sub-Saharan Africa?
What is the epidemiology, pathogenesis and outcome of type 1B or ketosis-prone type 2 diabetes in sub-Saharan Africa?
What are the mortality patterns of the various types of diabetes in sub-Saharan Africa?
What is the impact of HIV on diabetes prevalence across the region?
What are the best methods for improving care and its assessment?
Nayaran et al recently reviewed potential solutions to the global burden of diabetes and found the following to be highly feasible, cost saving and to have the greatest implementing priority in all developing regions of the world, including sub-Saharan Africa: glycaemic control in people with an HbA1c of >9%, blood pressure control in people with a blood pressure of >160/95 mm Hg and foot care in people with ulcers. The challenge is how to achieve even these limited objectives.74 It is probably salient to note that current recommendations are for the initiation of treatment in diabetic patients at a blood pressure of 140/90 mm Hg. Yet there are encouraging signs suggesting that care for diabetes in the region is turning the corner. In December 2006, the African Declaration for Diabetes was finally announced.75 This called on governments of African countries, non- governmental organisations, international donor agencies, industry, healthcare providers and all partners and stakeholders in diabetes to ensure access to quality and affordable services for prevention and care of diabetes.
Two major initiatives of the IDF Africa region were launched at the same time as the Declaration, which will assist in achieving this mission—namely, clinical practice guidelines and an education manual for health workers specific for the region. Although there is a plethora of guidelines for clinical care in many industrialised societies, it is not the case for sub-Saharan Africa. Notwithstanding the well-recognised problems relating to the uptake of guidelines,76 77 they stand a good chance of being implemented, provided that there are concerted efforts at regional, national and district level and the lessons learnt elsewhere are heeded. The process has already started in some countries, owing to strong support from the relevant government authorities, healthcare workers, diabetes associations and outside agencies such as the World Diabetes Foundation. It will be critical to evaluate the impact of the guidelines, with early examination of process measures of care being used to guide changes in order to improve the implementation strategy.
Although improved care for people with diabetes is imperative, attention should also be given to diabetes prevention. The risk factors for type 2 diabetes are clear, as are the evidence-based interventions required—they require implementation. As argued by Colagiuri et al changes in social policy will be the key to changing the social and physical environment required to achieve widespread reductions in the incidence and prevalence of diabetes.78
In conclusion, not only are there are great challenges facing this region for diabetes prevention and management but there are also many unanswered questions to engage the interest of researchers both resident in the region and abroad (box 1).
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 55.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
Footnotes
Competing interests: NSL has received honoraria for speaking engagements from Servier Laboratories, Novo Nordisk and Novartis and for attending Steering Committee meetings for a pharmaceutical trial for prevention of type 2 diabetes.
Funding: Novartis, Lilly and Aventis are providing funds to the unit for pharmaceutical trials used in the prevention or treatment of type 2 diabetes. Novo Nordisk provides funds for a community diabetes educator. NSL has received funds from Servier Laboratories towards the costs of a diabetes prevalence study.