Article Text

Abstract
Background: Obesity is associated with increased cardiovascular morbidity and mortality. A direct effect of isolated obesity on cardiac function is not well established.
Objective: To determine the direct effect of different grades of isolated obesity on echocardiographic indices of systolic and diastolic left ventricular function.
Methods: 48 obese and 25 normal weight women were studied. They had no other pathological conditions. Obesity was classed as slight (n = 17; body mass index (BMI) 25–29.9 kg/m2), moderate (n = 20; BMI 30–34.9 kg/m2), or severe (n = 11; BMI ⩾ 35 kg/m2). Echocardiographic indices of systolic and diastolic function were obtained, and dysfunction was assumed when at least two values differed by ⩾ 2 SD from the normal weight group.
Results: Ejection fraction (p < 0.05), fractional shortening (p < 0.05), and mean velocity of circumferential shortening (p < 0.05) were increased in slight and moderate obesity. Left ventricular dimensions were increased (p < 0.001) but relative wall thickness was unchanged. No obese patients met criteria for systolic dysfunction. In obese subjects, the mitral valve pressure half time (p < 0.01) and the left atrial diameter (p < 0.001) were increased and the deceleration slope was decreased (p < 0.01); all other diastolic variables were unchanged. No differences were found between obesity subgroups. Subclinical diastolic dysfunction was more prevalent among obese subjects (p = 0.002), being present in two with slight obesity (12%), seven with moderate obesity (35%), and five with severe obesity (45%). BMI correlated significantly with indices of left ventricular function.
Conclusions: Subclinical left ventricular diastolic dysfunction is present in all grades of isolated obesity, correlates with BMI, and is associated with increased systolic function in the early stages of obesity.
- obesity
- systolic function
- diastolic function
- echocardiography
- A, maximum velocity of active mitral filling
- AA, area under the curve of the velocity range corresponding to active mitral filling
- AE, area under the curve of the velocity range corresponding to passive mitral filling
- BMI, body mass index
- E, maximum velocity of passive mitral filling
- E/A, ratio of passive to active filling velocity
- EDD, end diastolic diameter
- EDV, end diastolic volume
- EP, ejection period
- ESD, end systolic diameter
- ESV, end systolic volume
- FS, fractional shortening
- IVRT, isovolumic relaxation time
- MV½T, mitral valve pressure half time
- PEP, pre-ejection period
- PWT, posterior wall thickness
- RWT, relative wall thickness
- VCS, velocity of circumferential fibre shortening
Statistics from Altmetric.com
- A, maximum velocity of active mitral filling
- AA, area under the curve of the velocity range corresponding to active mitral filling
- AE, area under the curve of the velocity range corresponding to passive mitral filling
- BMI, body mass index
- E, maximum velocity of passive mitral filling
- E/A, ratio of passive to active filling velocity
- EDD, end diastolic diameter
- EDV, end diastolic volume
- EP, ejection period
- ESD, end systolic diameter
- ESV, end systolic volume
- FS, fractional shortening
- IVRT, isovolumic relaxation time
- MV½T, mitral valve pressure half time
- PEP, pre-ejection period
- PWT, posterior wall thickness
- RWT, relative wall thickness
- VCS, velocity of circumferential fibre shortening
It is well established that obesity influences cardiovascular morbidity and mortality.1–8 An association between severe obesity and left ventricular dysfunction was first observed in the mid 20th century.9 Later, clinical and necropsy studies on morbid obesity confirmed the entity of obese cardiomyopathy, characterised by volume overload and hyperdynamism, frequently leading to congestive heart failure.10,11
Studies using echocardiography, cardiac catheterisation, and necropsy examination have shown relations between morbid obesity, structural alterations of the heart, and systolic function.12–14 These associations appear to be present even in cases of slight or mild obesity.15,16 However, the relation between obesity and alterations in diastolic function, and the impact of different grades of obesity on cardiac structure and function, are less well documented.
Our aim in this study was to determine the direct effect of different grades of isolated obesity on echocardiographic indices of systolic and diastolic left ventricular function.
METHODS
Study population
We studied 48 obese women (mean (SD) age, 29 (10) years; range 14–54 years) and 25 non-obese control women (mean age, 28 (9) years; range 15–44 years). Obesity was defined as a body mass index (BMI) of ⩾ 25 kg/m2, with clear evidence on physical examination of excessive subcutaneous adipose tissue. The participants in the study were classified into four groups based on the BMI: a normal weight (control) group had a BMI of < 25 kg/m2; slight obesity was classified as a BMI between 25–29.9 kg/m2; moderate obesity, as a BMI between 30–34.9 kg/m2; and severe obesity, as a BMI of ⩾ 35 kg/m2. The number of participants in each group were 25, 17, 20, and 11, respectively.
Inclusion criteria
In order to exclude conditions that might influence the results, the following criteria were required: simple obesity; female, of child bearing potential; not suffering from hypertension, diabetes mellitus, or dyslipidaemia; no previous history or clinical evidence of coronary artery disease, heart failure, or cardiac valve disease; normal ECG; no respiratory disease; not suffering from any chronic or acute disease; not taking any drugs that could affect the heart; and not involved in competitive sports. Echocardiographic images had to be of sufficient quality to allow reproducible cross sectional, M mode, and Doppler studies.
All subjects provided fully informed written consent for their participation in the study, and the protocol was approved by the ethics committee of our hospital.
Clinical assessment
All participants provided information on age, family history, personal habits (alcohol intake, tobacco consumption, type and level of physical exercise, drug ingestion, known pathological conditions) and the duration of the obesity. A detailed physical examination was conducted to exclude endocrine and cardiac comorbidities. Height and weight were measured and the BMI was calculated as the weight (kg)/height2 (m2). A 12 lead ECG was obtained. Haematological and biochemical variables were determined from fasting blood samples and included glucose, total cholesterol, triglycerides, high density lipoprotein cholesterol, urea, full blood count, free T4, TSH, and urinary free cortisol.
Echocardiographic assessment
A cross sectional echocardiogram was obtained on all participants (Sonos 1000, Hewlett-Packard, Palo Alto, California, USA). Echocardiograms were undertaken in our echocardiographic laboratory following standard methods. They included cross sectional, M mode, and Doppler studies.17–19 Triplicate measurements of all variables were made off-line by one observer who was blinded to the patients’ clinical details.
The following indices of cardiac function were evaluated:
Left ventricular systolic function—Left ventricular end diastolic (EDD) and end systolic diameter (ESD) and fractional shortening (FS) were obtained in the parasternal long axis views using M mode; left ventricular end diastolic (EDV) and end systolic volumes (ESV) and ejection fraction were measured from apical four chamber view using the monoplane area–length method; the systolic intervals, pre-ejection period (PEP), and ejection period (EP) were determined using the combination of the M mode echocardiography of the aortic valve and the ECG; the mean velocity of circumferential fibre shortening (VCS) was calculated as (EDD − ESD)/(EDD × EP). The relative wall thickness (RWT) was calculated from the posterior wall thickness (PWT) and the EDD, as (2 × PWT)/EDD.
Left ventricular diastolic function—Pulsed Doppler measurements were obtained in the apical four chamber view: the Doppler beam was aligned as perpendicularly as possible to the plane of the mitral annulus and a 5 mm pulsed wave Doppler sample volume was placed between the tips of the mitral leaflets during diastole. The following variables were calculated: maximum velocity of passive mitral filling (E); maximum velocity of active mitral filling (A); ratio of passive to active velocity (E/A); area under the curve of the velocity range corresponding to passive mitral filling (AE); area under the curve of the velocity range corresponding to active mitral filling (AA); ratio of AE/AA; mitral valve pressure half time (MV½12T); deceleration slope, and isovolumic relaxation time (IVRT). The left atrial diameter was measured using M mode in the parasternal long axis view.
Prevalence assessment
A difference of more than 2 SD from the mean values of the normal weight group was used to estimate the prevalence of cardiac functional abnormalities. Subclinical dysfunction was assumed when two or more indices of altered diastolic or systolic function were present.
Statistical analysis
Descriptive statistics were done on each of the variables to obtain the frequency distributions. Quantitative variables were described as mean (SD). Comparisons between the obese group and the normal weight group were analysed by t tests. Analysis of variance (one way ANOVA) was used to compare obese subgroups. Post hoc testing was undertaken using the Bonferroni multiple comparisons test. Correlations between clinical variables and left ventricular function were determined by linear regression analysis. Probability values of p < 0.05 were considered significant.
RESULTS
Characteristics of the groups in the study
The characteristics of the patients studied are presented in table 1. Only weight and BMI were significantly different within the obese subgroups, or with respect to the normal weight group (that is, the criteria for group assignment).
Baseline characteristics
Echographic variables
Left ventricular systolic function
The measured indices of left ventricular systolic function are presented in table 2. Diameters and volumes were significantly increased in obese women, though relative wall thickness was similar to control. The contractility indices (ejection fraction, fractional shortening, velocity of circumferential shortening) were significantly higher in the obese women than in the controls. On subgroup analysis, only the slight and moderate obesity subgroups reached significance. Analysis of systolic intervals showed that only the PEP/EP ratio was significantly higher in the obese group. In the prevalence analysis, no obese patient met the criteria for systolic dysfunction.
Indices of left ventricular systolic function
Left ventricular diastolic function
The measured indices of left ventricular diastolic function are presented in table 3. In obese subjects, MV½12T and left atrial diameter were increased and deceleration slope was decreased significantly, though subgroup analysis showed no significant differences among the obesity subgroups for these variables. The values of E, A, E/A ratio, AE, AA, AE/AA ratio, and IVRT were similar in obese and normal weight subjects.
Indices of left ventricular diastolic function
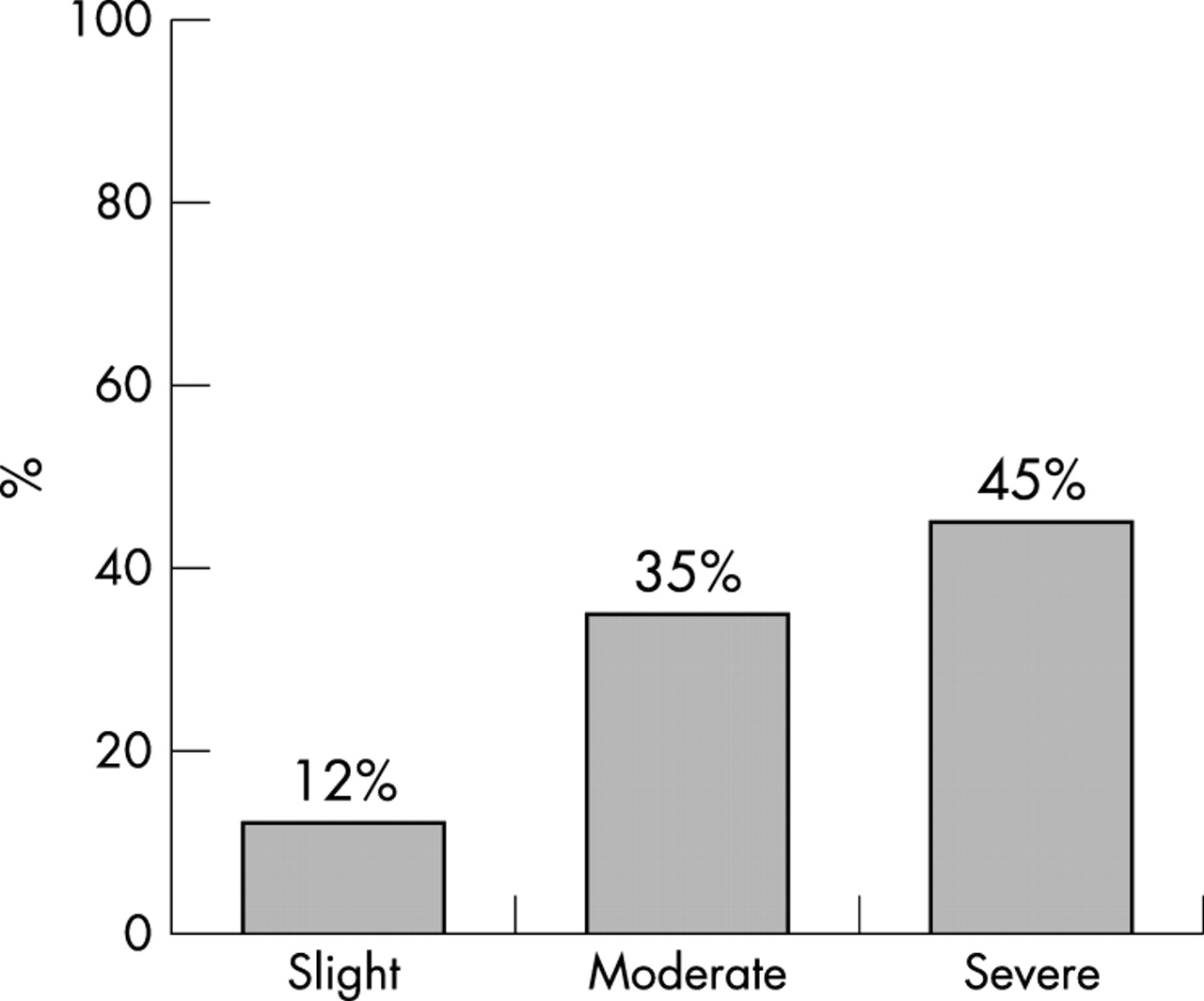
In the prevalence assessment (fig 1), subclinical diastolic dysfunction was significantly more prevalent among obese patients (p = 0.002) than in the control group: it was found in two patients with slight obesity (12%), in seven with moderate obesity (35%), and in five with severe obesity (45%). Overall, 14 women (29% of all the obese women) had diastolic dysfunction.

{kind=link}
Prevalence of subclinical diastolic dysfunction in the obesity subgroups.
Correlations
The correlations between clinical variables and left ventricular function are shown in table 4. Among the indices of systolic function, BMI correlated positively with %FS, VCS, and the PEP/EP ratio; EP correlated positively with age, and PEP with both systolic and diastolic pressure.
Matrix of correlations between the clinical variables and left ventricular systolic and diastolic function
Among the indices of diastolic function, BMI correlated positively with MV½12T and left atrial diameter, and inversely with deceleration slope. Similarly, age correlated positively with AA and left atrial diameter, and negatively with A, E/A, and AE/AA. Systolic pressure correlated positively with A, AA, and left atrial diameter, and inversely with E/A and AE/AA. Finally, only left atrial diameter correlated positively with diastolic pressure.
DISCUSSION
Indices of left ventricular systolic function
No patient with isolated obesity presented with subclinical systolic dysfunction. On the contrary, there was a significant increase in the ejection fraction, in the percentage of fractional shortening, and in the mean velocity of circumferential fibre shortening in obesity, but this only reached significance in slight and moderate obesity groups compared with the controls. These findings could be explained on the basis that in the groups with lesser degrees of obesity there is a compensatory increase in systolic function, which has not yet reached the stage of cardiac deterioration. The ejection fraction is a reliable index but is relatively insensitive to left ventricular contractile function, so its value may be maintained within normal limits even when there is substantial compensatory modification of the contractile state. However, the normality of the ejection fraction was in accordance with the normal relative wall thickness in our obese groups, which indicates that systolic function was preserved.
Most echocardiographic studies using measurements of the ejection phases to evaluate systolic function in obese subjects have shown normal results.20–25 Studies in which these indices have been found to be reduced, albeit modestly, were done on patients with a considerable degree of obesity, suggesting that left ventricular systolic function is affected late in the course of obesity.20
With respect to the systolic intervals, there were hardly any alterations except an increase in the PEP/EP ratio in women with moderate obesity. Other studies that evaluated these indices did not observe any major alterations either.26
Indices of left ventricular diastolic function
Our obese subjects showed alterations in the left ventricular diastolic function that were more frequent with increasing obesity. The MV½12T was found to be significantly prolonged in the obese women and correlated directly with the grade of obesity. This parallels the findings in other studies and suggests an abnormal relaxation of the left ventricle, with increased dependency on left atrial contraction for normal filling.26,27 Similarly, the deceleration slope was significantly decreased in the obese subjects and correlated inversely with BMI. Several previous studies have also shown a decrease in the mitral ejection fraction slope, although some others have not.24,26
IVRT was similar in our obese subjects and in our controls, and it was not correlated with BMI, in contrast to previously published data in which this variable was found to be prolonged in both moderate and gross obesity.24,26
The E, A, E/A, AE, and AE/AA values did not differ across the spectrum of obesity. The associations of these indices with obesity reported in previous studies have been variable. Zarich and colleagues observed a significant decrease in the maximum velocity of passive mitral filling (E) among obese patients, while the values for active mitral filling (A) were not significantly affected, resulting in a decrease in the E/A ratio.24 Conversely, Chakko and colleagues did not find significant differences in the values of E, but values of A were increased, resulting in a decreased E/A ratio.27 Stoddard and associates found a significant increase in both E and A values, which were positively correlated with the percentage of body weight in excess of the ideal, so that the E/A ratio was not altered.26
The Doppler method of measuring indices of left ventricular filling has been shown to be of great value in assessing diastolic function.28 However, when volume overload is present, as it is in obesity, normal values may result, as the increase in left atrial pressure caused by intravascular volume can mask the alterations observed in the early phases of abnormal diastolic relaxation.19
In contrast to systolic function, we found that alterations in diastolic function were common, not only in the severely obese women but in slightly obese and moderately obese subjects as well. These alterations in diastolic function correlated strongly with body mass index. In obesity, cardiac adaptation to chronic volume overload is associated with eccentric hypertrophy and abnormalities of diastolic function from the initial stages, indicating that structural changes and an obesity cardiomyopathy are present in all obese individuals.27 In consequence, greater awareness needs to be focused on weight loss in order to induce beneficial changes in cardiac morphology and function. The alterations that occur in obesity can be reversed easily and quickly by weight loss, to the long term benefit of the patient.29–34
Limitations
Obesity was measured using only BMI, and no measurements of body fat distribution were made. A better relation might have been found between abdominal obesity and echocardiographic alterations. Investigation of cytokines, leptin, sympathetic nervous system activity, and renin–angiotensin–aldosterone system activity could have added information about the underlying mechanisms. The selection of the study sample, which included only women, precludes extrapolation of our results to the general population.
Conclusions
Among patients with isolated obesity, subclinical left ventricular diastolic dysfunction is present in all grades of obesity, correlates with BMI, and is associated with an increased in systolic function in the early stages of obesity.